
Abstract
Purpose
To investigate corneal microstructural alterations in patients with trigeminal neuralgia using in vivo confocal microscopy and to compare these findings with healthy controls.
Methods
In this prospective, cross-sectional study, sixty patients with unilateral trigeminal neuralgia and sixty matched healthy controls underwent central corneal imaging using in vivo confocal microscopy. Images were obtained from all corneal layers. Quantitative analysis of the subbasal nerve plexus assessed corneal nerve fiber density (CNFD), corneal nerve fiber length (CNFL), and corneal nerve branch density (CNBD). Qualitative evaluation of epithelial morphology, dendritic cell density, stromal keratocyte activation, and endothelial features was performed. Associations between corneal findings and disease duration were analyzed.
Results
Compared with controls, trigeminal neuralgia patients demonstrated significant reductions in CNFD, CNFL, and CNBD (all p < 0.001), accompanied by increased nerve tortuosity, fragmentation, and focal nerve dropout. Dendritic cell density and anterior stromal keratocyte activation were increased, particularly in patients with longer disease duration, while posterior stromal layers and endothelial morphology remained preserved. Disease duration was independently associated with greater subbasal nerve loss and inflammatory changes.
Conclusions
Trigeminal neuralgia is associated with significant neurodegenerative and inflammatory alterations of the cornea, primarily involving the subbasal nerve plexus. In vivo confocal microscopy provides a sensitive, non-invasive tool for detecting these changes and may aid in assessing disease severity and progression. To our knowledge, this is the first study to demonstrate disease duration-dependent multilayer corneal microstructural alterations in trigeminal neuralgia using in vivo confocal microscopy.
This is a visual representation of the abstract.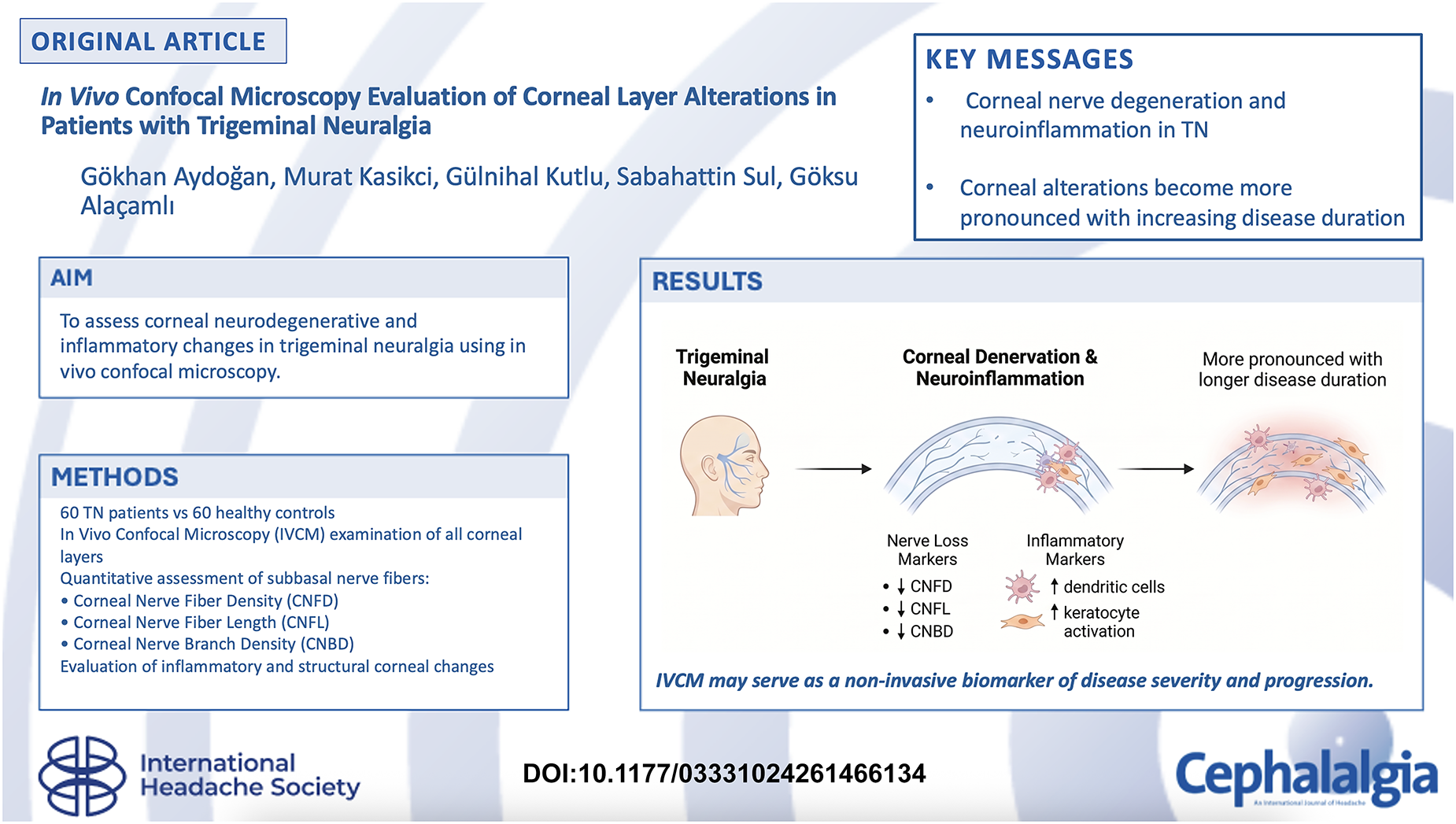
Keywords
Introduction
Trigeminal neuralgia (TN) is a chronic neuropathic pain disorder characterized by sudden, severe, and recurrent episodes of facial pain affecting one or more divisions of the trigeminal nerve. 1 Although the classical pathophysiological concept of TN has emphasized central mechanisms such as neurovascular compression and central sensitization, increasing evidence suggests that peripheral nerve degeneration and neuroinflammatory processes also contribute significantly to disease onset and persistence.2,3
Peripheral involvement of trigeminal nerve fibers may result in altered sensory input, impaired neurotrophic support, and dysregulated immune–neural interactions, which together may perpetuate chronic pain. 4 The cornea is innervated primarily by the ophthalmic division (V1) of the trigeminal nerve. Trigeminal afferent fibers enter the cornea through the long ciliary nerves and form the subbasal nerve plexus, which plays an essential role in corneal sensation, epithelial trophism, wound healing, and neuroimmune regulation.5–7 This anatomical relationship makes the cornea a useful surrogate for evaluating peripheral trigeminal small fiber integrity.
Objective assessment of peripheral nerve pathology in TN, however, remains challenging in routine clinical practice. The cornea represents a unique model for evaluating peripheral trigeminal nerve integrity, as it is one of the most densely innervated tissues in the human body and receives its sensory innervation primarily from the ophthalmic branch of the trigeminal nerve.5–7 Corneal nerves are essential not only for sensory perception but also for epithelial maintenance, wound healing, and immune homeostasis.8,9 Disruption of corneal innervation has been associated with epithelial instability, inflammation, and stromal remodeling. 10
In vivo confocal microscopy (IVCM) is a non-invasive imaging modality that allows real-time visualization of corneal layers at a cellular level, including corneal nerves, immune cells, and stromal components. 11 Previous studies have demonstrated corneal nerve alterations in systemic neuropathies and neurodegenerative disorders.12–14 However, comprehensive, layer-by-layer evaluation of corneal involvement in trigeminal neuralgia remains limited.
The aim of this study was to evaluate microstructural alterations across all corneal layers from epithelium to endothelium in patients with trigeminal neuralgia using IVCM and to compare these findings with healthy controls.
Materials and methods
Study design and ethics
This prospective, cross-sectional, controlled study was conducted in accordance with the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board/Ethics Committee of Izmir Bakircay University (Decision No: 1925, Research No: 1905). Written informed consent was obtained from all participants prior to enrollment. This study was conducted in accordance with the STROBE guidelines for observational studies.
Study population
Sixty patients diagnosed with unilateral trigeminal neuralgia by a neurologist based on the International Classification of Headache Disorders criteria were enrolled. Patients with classical unilateral trigeminal neuralgia involving any trigeminal division (V1, V2, or V3) were eligible for inclusion. Sixty age and sex matched healthy volunteers served as the control group.
Healthy control participants were recruited from hospital staff members and individuals presenting for routine ophthalmologic examination. Controls were frequency-matched to the trigeminal neuralgia group according to age and sex. All healthy participants underwent detailed ophthalmologic and neurological evaluation to exclude systemic or ocular conditions potentially affecting corneal nerve morphology, including diabetes mellitus, autoimmune disease, peripheral neuropathy, ocular surface disease, prior ocular surgery or trauma, contact lens use, and chronic neurological or pain disorders.
Exclusion criteria included diabetes mellitus, autoimmune or inflammatory systemic disease, contact lens use, history of ocular surgery or trauma, corneal disease, dry eye disease, glaucoma, systemic neuropathy, and use of topical ocular medications. Additionally, patients with secondary trigeminal neuralgia related to multiple sclerosis, intracranial tumors, or other structural lesions were excluded to ensure a homogeneous cohort of patients with classical trigeminal neuralgia.
In vivo confocal microscopy
All participants underwent central corneal imaging using the Heidelberg Retina Tomograph III with Rostock Corneal Module (HRT III/RCM). A disposable TomoCap and 0.2% carbomer gel were used for optical coupling. The examination was performed under topical anesthesia (proparacaine hydrochloride 0.5%) with patients instructed to fixate on a distant target to maintain alignment.
A minimum of 8 high-resolution image stacks were obtained per eye, covering all major corneal layers in sequential order: superficial epithelium, basal epithelium, Bowman's layer, subbasal nerve plexus, anterior stroma, posterior stroma, Descemet's membrane and endothelium. Each stack consisted of 80–100 images (384 × 384 µm frame size; 1 µm optical slice thickness).
For quantitative analysis of the subbasal nerve plexus, six non-overlapping, high-quality images were selected per eye using a standardized protocol. Images were selected based on optimal focus, contrast, and absence of motion artefacts. To minimize selection bias, images were obtained from the central cornea and analyzed in a masked fashion by two independent observers. In cases of disagreement, consensus was achieved through joint review.
Quantitative nerve analysis was performed using ACCMetrics software (University of Manchester, UK), including measurements of:
CNFD: total number of nerves/mm2 CNFL: total nerve length (mm/mm2) CNBD: number of branches/mm2
Epithelial and stromal cell morphology, dendritic cell characteristics, keratocyte reflectivity and endothelial features were evaluated qualitatively by two blinded observers. Qualitative nerve morphology was graded using a semi-quantitative scale. Nerve tortuosity was graded as: 0 = none, 1 = mild, 2 = moderate, and 3 = severe tortuosity. Nerve fragmentation and focal thinning were recorded as present or absent. Dendritic cells were considered activated when displaying enlarged cell bodies with prominent dendritic processes, consistent with established morphological criteria. In addition, dendritic cells were further characterized descriptively based on their morphology and their spatial relationship with corneal nerve fibers, in accordance with previously reported approaches. 15 Cells exhibiting dendritic processes were distinguished from those without such features, and their apparent proximity or contact with nerve fibers was noted. This assessment was performed qualitatively without formal quantitative subclassification. Formal quantitative dendritic cell density measurements (cells/mm2) were not systematically performed. Epithelial irregularity and keratocyte activation were also recorded using predefined morphological criteria. Interobserver agreement for qualitative variables was assessed using percentage agreement. Quantitative parameters (CNFD, CNFL, CNBD) were evaluated using intraclass correlation coefficients. These parameters were evaluated qualitatively due to the absence of validated automated quantification tools for all corneal layers. The frequency of qualitative morphological features was recorded as the proportion of eyes exhibiting each feature within each group and compared statistically.
Statistical analysis
Statistical analyses were performed using SPSS software. Continuous variables were expressed as mean ± standard deviation. Comparisons between groups were performed using independent-sample t-tests or Mann–Whitney U tests. Normality was assessed using Shapiro–Wilk test. Between-group comparisons were performed using independent t-test (parametric) or Mann–Whitney U test (non-parametric). Effect sizes (Cohen's d) were calculated for significant differences. Pearson/Spearman correlation tested associations between disease duration and IVCM parameters. Multiple linear regression evaluated whether disease duration predicted CNFD, CNFL, CNBD and dendritic cell density after adjusting for age and sex. Prior to regression analysis, assumptions of normality and linearity were evaluated. Residual distributions were assessed visually, and variance inflation factors (VIFs) were calculated to exclude significant multicollinearity. Bonferroni correction was applied to control for multiple comparisons. A p-value <0.05 was considered statistically significant. Although no a priori sample size calculation was performed due to the exploratory design of the study, a post-hoc power analysis was conducted based on the observed differences in primary subbasal nerve parameters between trigeminal neuralgia affected eyes and controls. The estimated statistical power exceeded 90% for the primary outcome measures at an alpha level of 0.05. Additional three-group comparisons were performed between affected eyes, contralateral eyes, and healthy controls using one-way ANOVA for normally distributed variables or Kruskal-Wallis tests for non-normally distributed variables, followed by Bonferroni adjusted post-hoc analyses.
Furthermore, patients with trigeminal neuralgia were divided into subgroups based on disease duration. Patients diagnosed within ≤12 months were classified as the early-diagnosis group, while patients with a disease duration of >12 months were classified as the delayed-diagnosis group. Subbasal nerve parameters (CNFD, CNFL, CNBD), dendritic cell density, and stromal keratocyte reflectivity were compared between these subgroups using independent-sample t-tests or Mann–Whitney U tests, as appropriate. Correlations between disease duration and IVCM parameters were evaluated using Pearson or Spearman correlation analyses. Receiver operating characteristic (ROC) analysis was performed to evaluate the ability of corneal nerve parameters to distinguish early-stage trigeminal neuralgia (≤12 months disease duration) from delayed-stage trigeminal neuralgia (>12 months disease duration). Optimal cut-off values were determined using the Youden Index.
Results
Demographic and clinical characteristics
The trigeminal neuralgia and control groups were comparable in terms of age and sex distribution (p > 0.05). The mean disease duration in the TN group was 6.2 ± 3.1 years. Thirty-two patients had right-sided and twenty-eight had left-sided trigeminal involvement.
Corneal epithelium
IVCM revealed significant epithelial alterations in the TN group. Epithelial cell density was reduced, and cell borders appeared irregular and poorly demarcated compared with controls. Increased epithelial reflectivity and areas of cellular heterogeneity were predominantly observed in eyes ipsilateral to the affected trigeminal nerve and were significantly more frequent than in control eyes
Bowman's layer
Bowman's layer demonstrated focal structural disorganization in TN patients, characterized by irregular reflectivity and loss of homogeneity. These alterations were significantly more frequent on the affected side compared with control eyes and were absent in the majority of controls
Subbasal nerve plexus
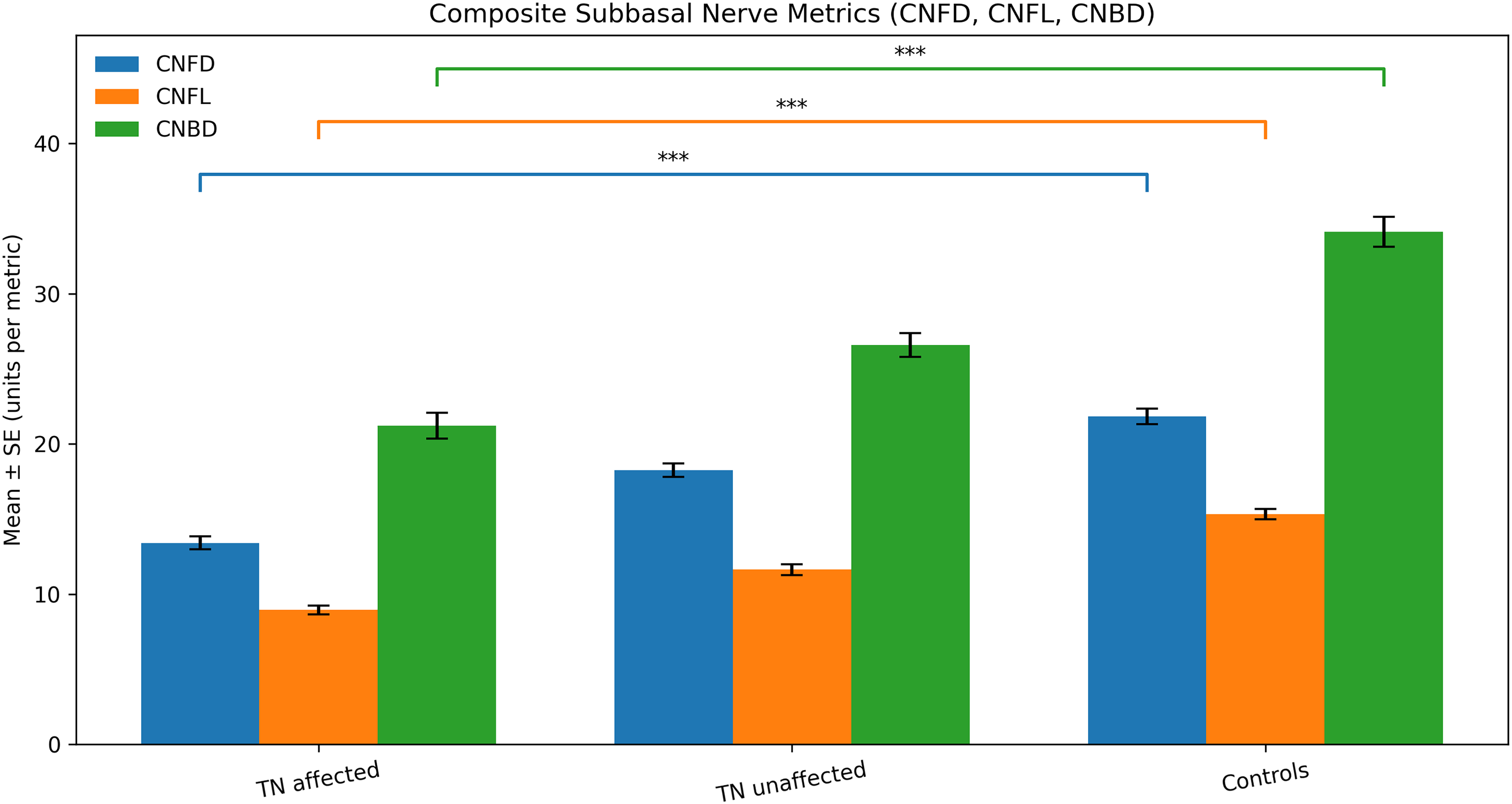
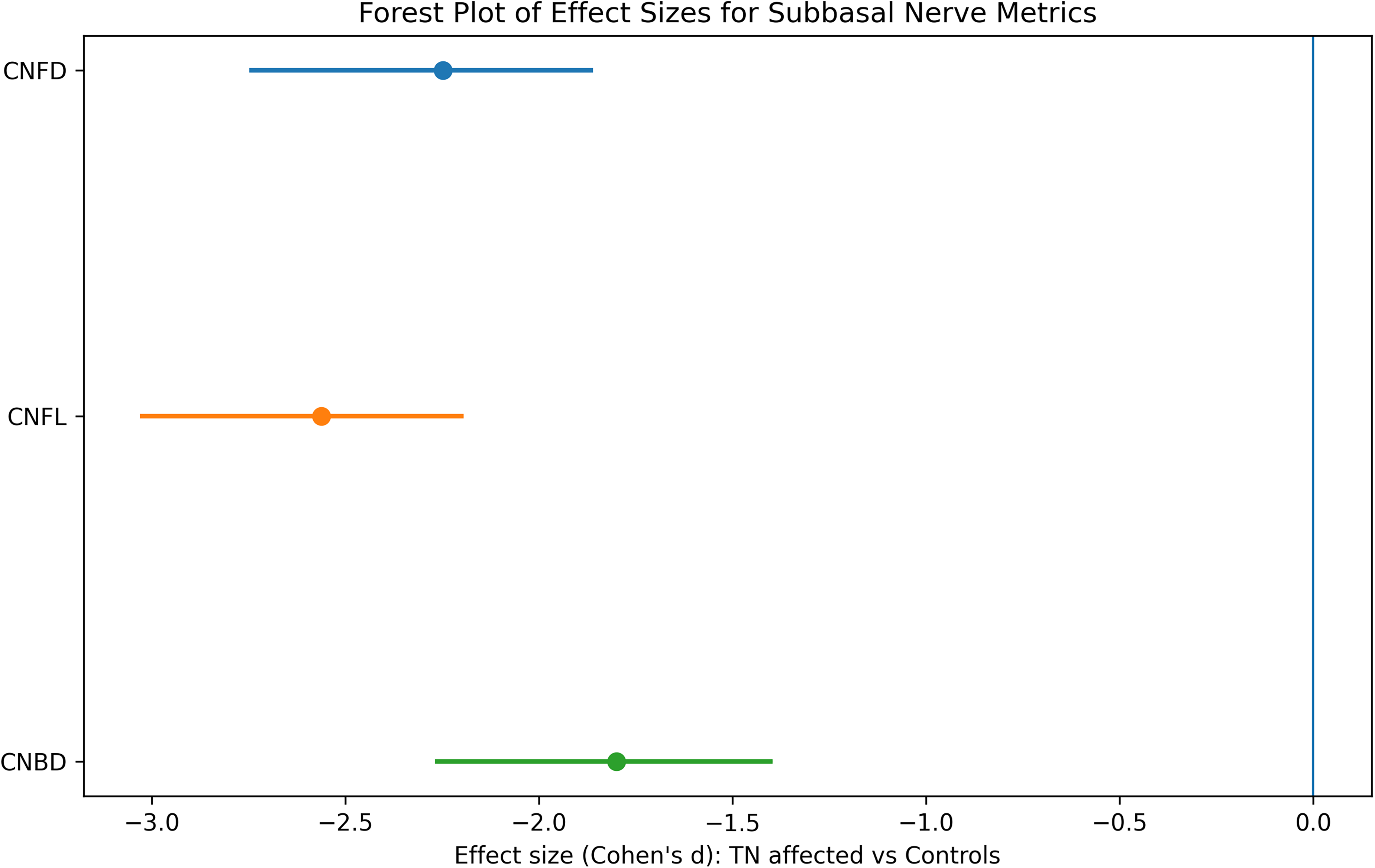
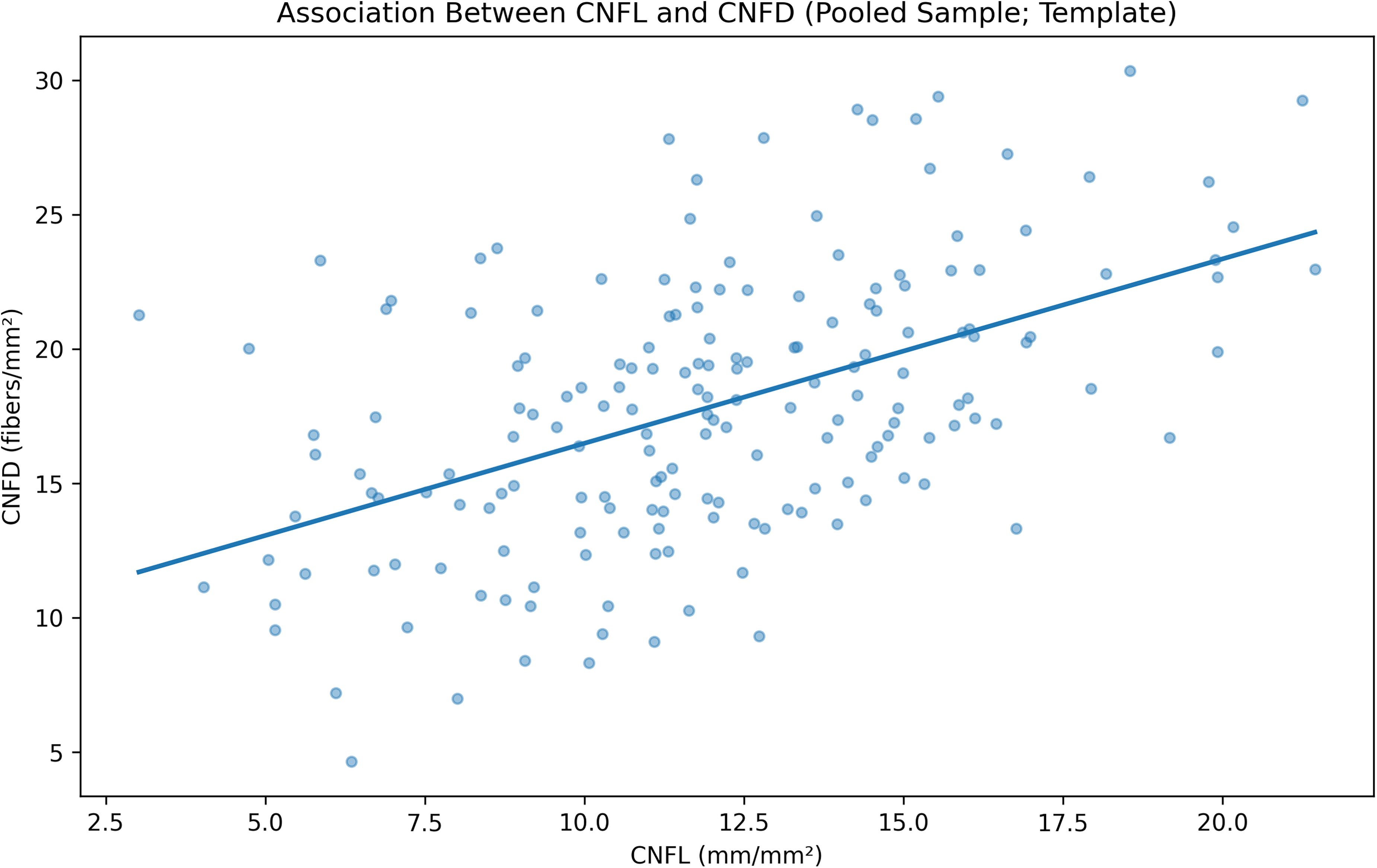
Quantitative analysis of the subbasal nerve plexus demonstrated significant reductions in all nerve parameters in trigeminal neuralgia affected eyes compared with healthy controls (Figure 1). CNFD was lower in affected eyes than in controls (13.4 ± 1.8 vs. 21.8 ± 2.2 fibers/mm2, p < 0.001). Contralateral eyes showed intermediate CNFD values (18.2 ± 2.0 fibers/mm2), with borderline significance compared with controls before correction for multiple comparisons. However, these differences did not remain statistically significant after Bonferroni correction. CNFL was also lower in affected eyes than in controls (9.1 ± 1.2 vs. 15.0 ± 1.5 mm/mm2, p < 0.001). Similarly, contralateral eyes demonstrated intermediate CNFL values (11.8 ± 1.3 mm/mm2), showing borderline uncorrected significance compared with controls; however, statistical significance was not maintained after Bonferroni correction.(Figure 2) Similarly, CNBD was lower in affected eyes than in controls (21.2 ± 1.7 vs. 34.1 ± 1.9 branches/mm2, p < 0.001). Contralateral eyes also demonstrated intermediate CNBD values (26.5 ± 1.6 branches/mm2), although these differences did not remain statistically significant after correction for multiple comparisons. Effect size analysis demonstrated large differences between affected eyes and controls for all subbasal nerve parameters, with Cohen's d values of 1.42 for CNFD, 1.51 for CNFL, and 1.47 for CNBD (Figure 3). In addition, a significant positive association was observed between CNFL and CNFD across the pooled dataset (Figure 4). Representative in vivo confocal microscopy images illustrating subbasal nerve loss and increased dendritic cell density in trigeminal neuralgia are shown in Figure 5.
Composite bar graph of subbasal nerve Plexus parameters. Composite bar graph comparing corneal nerve fiber density (CNFD), corneal nerve fiber length (CNFL), and corneal nerve branch density (CNBD) among trigeminal neuralgia affected eyes, unaffected eyes, and healthy controls. Three group statistical comparisons were performed using ANOVA or Kruskal-Wallis tests with post-hoc multiple comparison correction. Bars represent mean values with standard error of the mean. Statistical significance between groups is indicated by brackets.
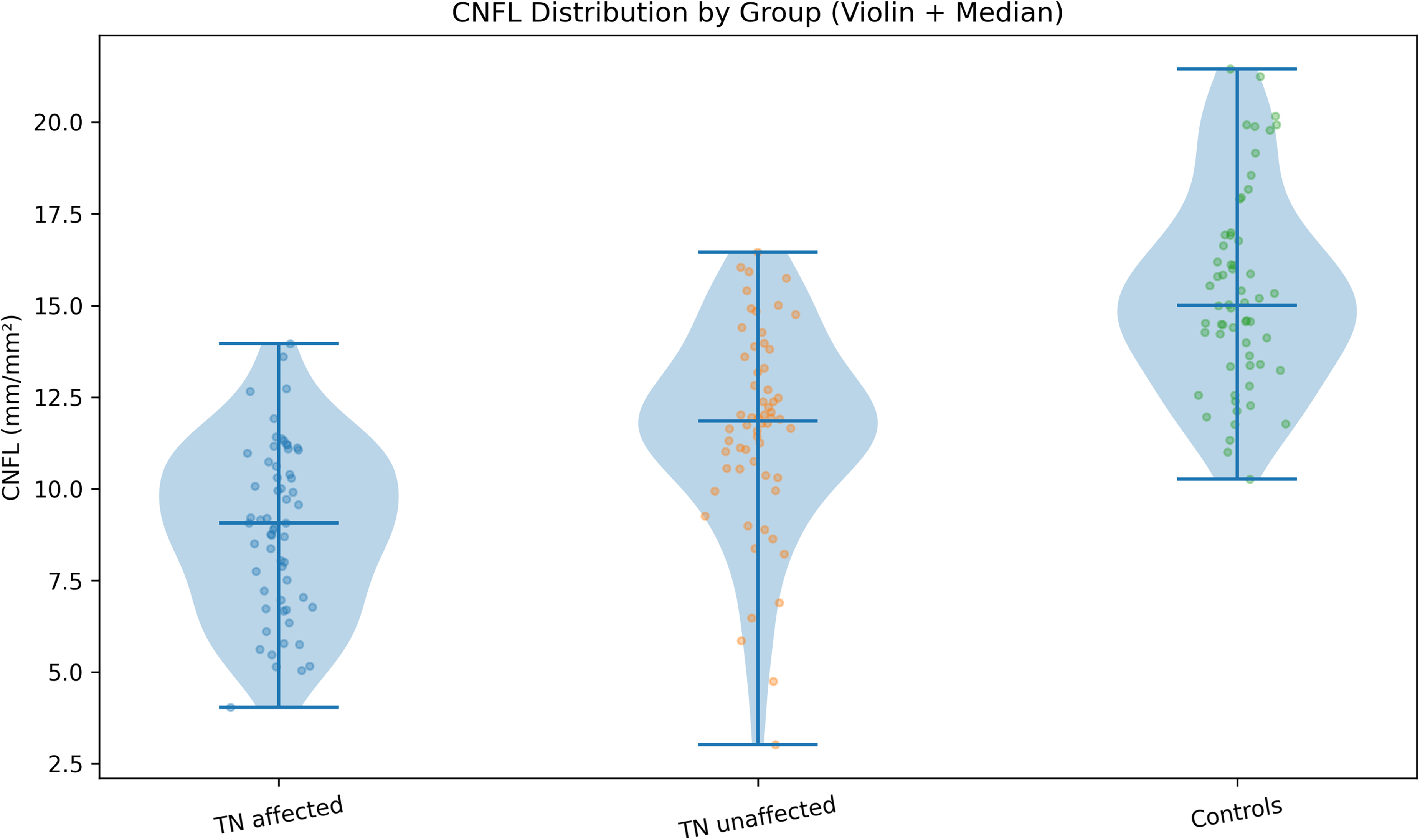
Violin plot showing distribution of corneal nerve fiber length (CNFL). Violin plot illustrating the distribution of corneal nerve fiber length (CNFL) in trigeminal neuralgia affected eyes, unaffected eyes, and healthy controls. The width of each violin represents kernel density, the central line denotes the median, and overlaid jittered points represent individual measurements, highlighting within-group variability.
Forest plot of effect sizes for subbasal nerve parameters. Forest plot displaying effect sizes (Cohen's d) with 95% confidence intervals for corneal nerve fiber density (CNFD), corneal nerve fiber length (CNFL), and corneal nerve branch density (CNBD), comparing trigeminal neuralgia affected eyes with healthy controls. Negative effect sizes indicate lower parameter values in affected eyes.
Scatter plot demonstrating the association between CNFL and CNFD. Scatter plot showing the association between corneal nerve fiber length (CNFL) and corneal nerve fiber density (CNFD) across the pooled study population. Each point represents an individual eye, and the solid line represents the fitted linear regression.
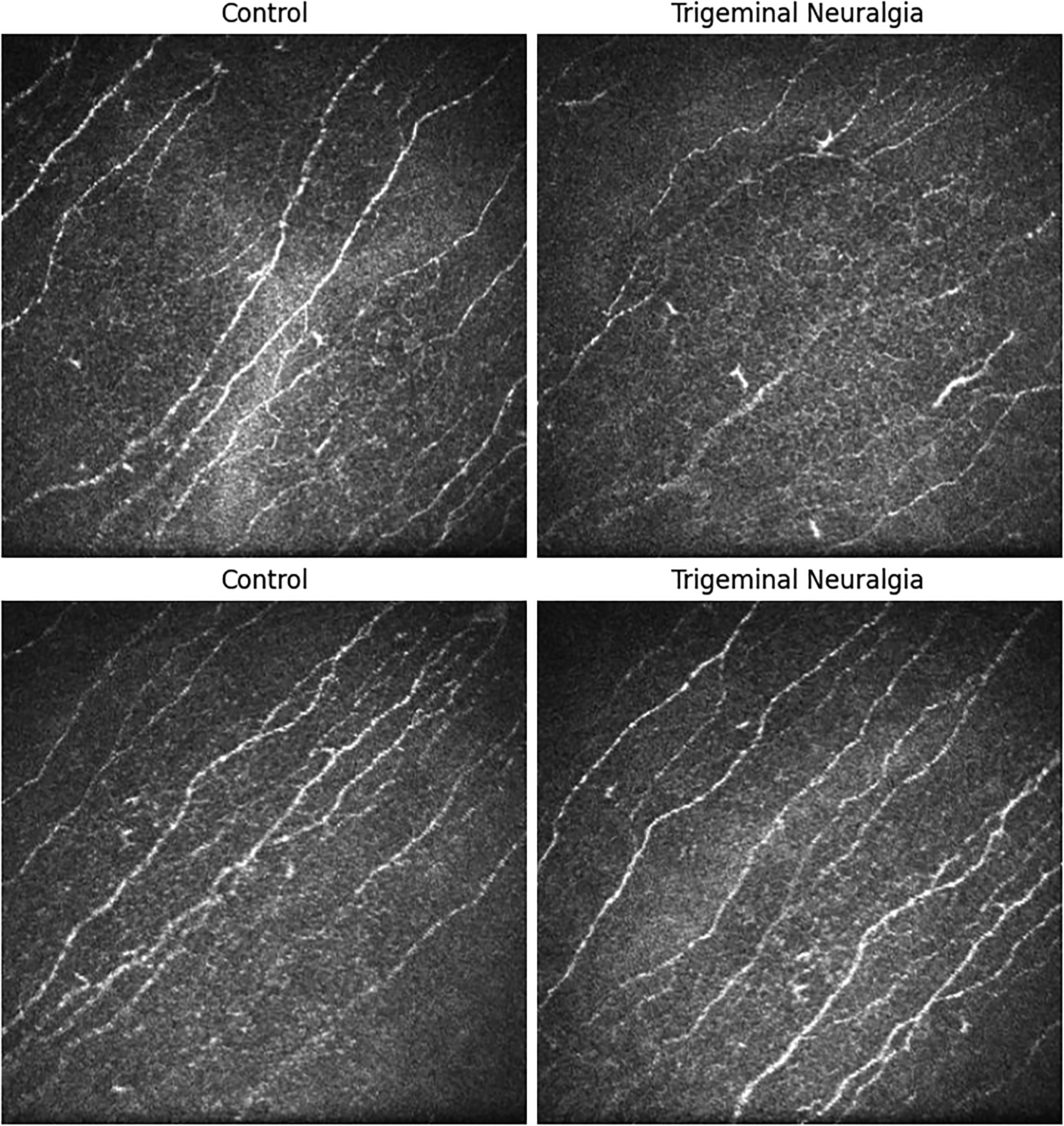
In vivo confocal microscopy images of the subbasal nerve plexus obtained from study participants. Images acquired from healthy control eyes (left panels) show a dense, continuous, and well-organized subbasal nerve plexus, characterized by long, uniformly thick, and predominantly parallel-running nerve fibers with minimal tortuosity and preserved nerve continuity. In contrast, images obtained from patients with trigeminal neuralgia (right panels) demonstrate marked disruption of subbasal nerve architecture, including pronounced reduction in corneal nerve fiber density and length, increased nerve tortuosity, focal nerve fragmentation, and areas of nerve dropout. Numerous hyperreflective dendritic cells with activated morphology are also evident in the subbasal region, indicating an associated inflammatory microenvironment. These qualitative in vivo findings directly support and visually corroborate the quantitative reductions in corneal nerve fiber density (CNFD), corneal nerve fiber length (CNFL), and corneal nerve branch density (CNBD) observed in Figures 1–4. Scale bar = 50 µm.
Quantitative subbasal nerve parameters for all groups are summarized in Table 1.
Quantitative subbasal nerve plexus parameters in trigeminal neuralgia affected eyes, contralateral eyes, and healthy controls.
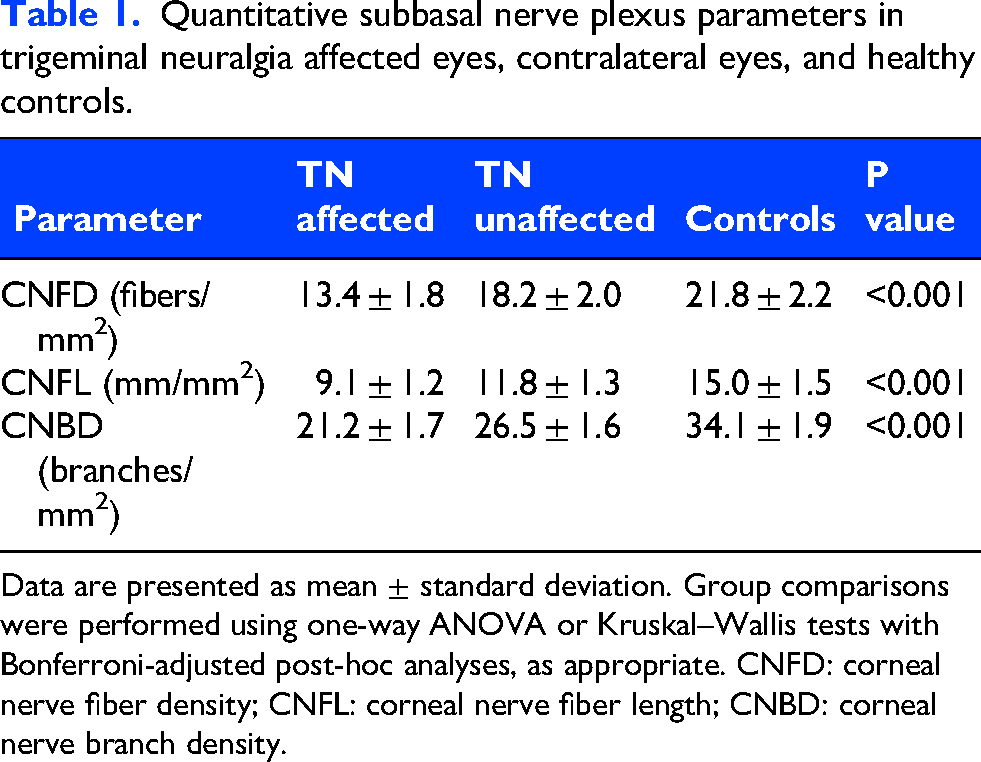
Data are presented as mean ± standard deviation. Group comparisons were performed using one-way ANOVA or Kruskal–Wallis tests with Bonferroni-adjusted post-hoc analyses, as appropriate. CNFD: corneal nerve fiber density; CNFL: corneal nerve fiber length; CNBD: corneal nerve branch density.
Dendritic cells and axonal structures
Activated dendritic cells and qualitative inflammatory changes were observed more frequently in trigeminal neuralgia eyes compared with controls (p < 0.001). Activated dendritic cells displayed enlarged cell bodies with elongated dendritic processes, while subbasal axonal structures appeared disorganized with irregular orientation and fragmentation. Descriptive evaluation suggested close spatial association between dendritic cells and subbasal nerve fibers, with occasional apparent contact between dendritic processes and nerve fibers, supporting the presence of local neuroimmune interactions. Qualitative corneal alterations were more frequent in trigeminal neuralgia eyes than in controls. Irregular epithelium was observed in 24 of 60 TN eyes (40.0%) and 8 of 60 control eyes (13.3%, p = 0.003). Bowman's layer disorganization was present in 22 TN eyes (36.7%) and 6 control eyes (10.0%, p = 0.002). Increased nerve tortuosity was detected in 42 TN eyes (70.0%) compared with 10 control eyes (16.7%, p < 0.001), and nerve fragmentation was observed in 38 TN eyes (63.3%) compared with 5 control eyes (8.3%, p < 0.001). Activated dendritic cells were present in 45 TN eyes (75.0%) and 12 control eyes (20.0%, p < 0.001). Keratocyte activation was detected in 30 TN eyes (50.0%) and 9 control eyes (15.0%, p = 0.001). Spearman correlation analysis demonstrated a significant positive correlation between disease duration and dendritic cell density (r = 0.64, 95% CI: 0.48–0.76, p < 0.001). Disease duration was an independent predictor of CNFD (β=-0.48, adjusted R2=0.29), CNFL (β=-0.52, adjusted R2=0.33), CNBD (β=-0.46, adjusted R2=0.27), and dendritic cell density (β=+0.51, adjusted R2=0.31) after adjustment for age and sex (p < 0.01 for all). Regression diagnostics demonstrated no evidence of significant multicollinearity (all VIF values <2.0), and residual distributions were visually acceptable.
Interobserver reliability
Interobserver reliability analysis demonstrated high reproducibility for both quantitative and qualitative IVCM assessments. Intraclass correlation coefficients (ICC) for quantitative subbasal nerve parameters were 0.92 for CNFD, 0.89 for CNFL, and 0.88 for CNBD. Percentage agreement for qualitative morphological assessments was 91% for epithelial irregularity, 93% for nerve tortuosity, 90% for activated dendritic cell identification, and 88% for keratocyte activation.
Early vs delayed diagnosis subgroup analysis
The early-stage trigeminal neuralgia subgroup (≤12 months disease duration) included 15 patients, whereas the delayed-stage subgroup (>12 months disease duration) included 45 patients. Patients with disease >12 months showed significantly lower CNFD, CNFL, and CNBD values, higher dendritic cell density, and increased stromal keratocyte activation compared with patients diagnosed at an earlier stage.
ROC analysis demonstrated that CNFL had the highest discriminative performance (AUC = 0.81). The optimal cutoff value determined using the Youden index was 12.2 mm/mm2, yielding 82% sensitivity and 78% specificity.
Stromal keratocytes
Anterior stromal keratocytes in TN patients showed increased reflectivity and signs of cellular activation, particularly on the affected side. Posterior stromal keratocytes remained largely unaffected (p > 0.05)
Descemet's membrane and endothelium
No significant abnormalities were detected in Descemet's membrane. Endothelial cell density, hexagonality, and pleomorphism were comparable between TN patients and controls (p > 0.05).
Table 2 provides a structured summary of the frequency of qualitative corneal alterations across different corneal layers, supporting the descriptive findings observed above and demonstrating a higher prevalence of epithelial irregularity, Bowman's layer disorganization, nerve tortuosity, nerve fragmentation, dendritic cell activation, and keratocyte activation in trigeminal neuralgia patients compared with controls.
Frequency (%) of qualitative corneal morphological findings in trigeminal neuralgia and control groups.
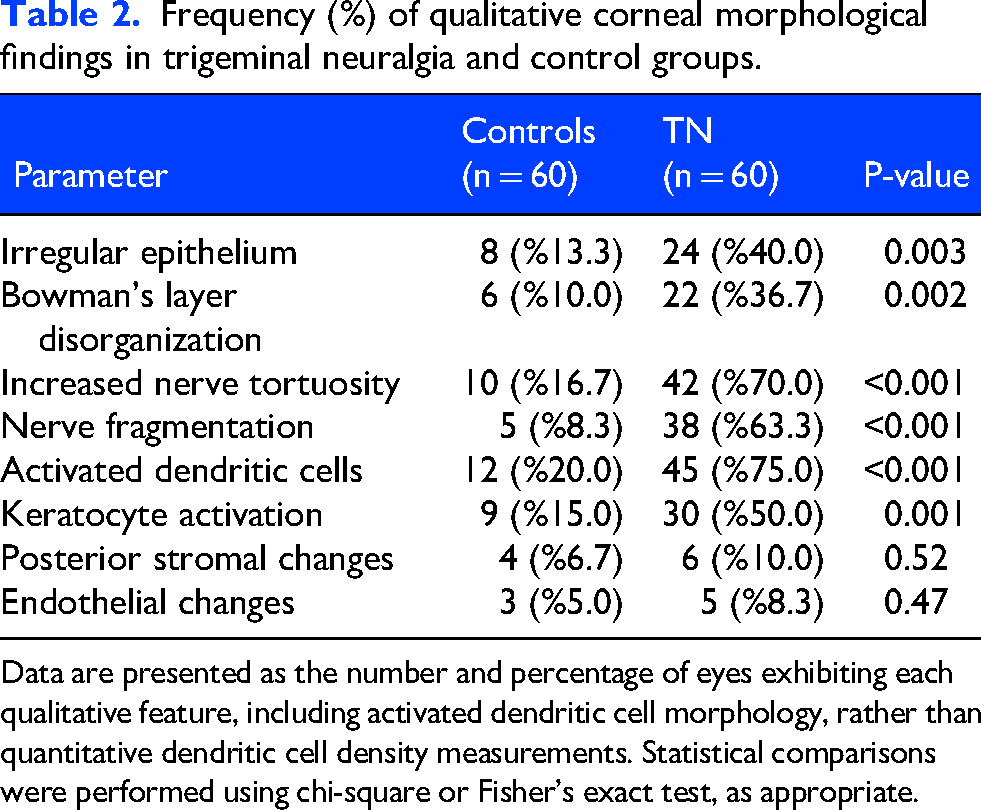
Data are presented as the number and percentage of eyes exhibiting each qualitative feature, including activated dendritic cell morphology, rather than quantitative dendritic cell density measurements. Statistical comparisons were performed using chi-square or Fisher's exact test, as appropriate.
Discussion
This study demonstrates that trigeminal neuralgia (TN) is associated with significant multilayer corneal microstructural alterations detectable by in vivo confocal corneal microscopy (IVCM), supporting the concept that TN is not solely a central neuropathic pain disorder but also involves progressive peripheral trigeminal small fiber pathology accompanied by neuroinflammatory activation. These findings are consistent with mechanistic models suggesting that demyelination and ectopic impulse generation at the trigeminal root entry zone may lead to distal axonal degeneration involving peripheral sensory terminals, including corneal nerves. 16
Our results demonstrate selective multilayer corneal involvement, predominantly affecting the epithelium, Bowman's layer, subbasal nerve plexus, and anterior stroma, while deeper corneal layers such as the posterior stroma, Descemet's membrane, and endothelium remain largely preserved. This distribution pattern strongly supports a nerve-dependent pathogenic mechanism rather than diffuse corneal degeneration. Previous histological and confocal investigations have established that corneal subbasal nerves and the limbal nerve plexus originate from trigeminal afferent fibers, providing anatomical continuity between the ophthalmic branch of the trigeminal nerve and corneal neural architecture.5,6
Degeneration of the subbasal nerve plexus represents the most prominent structural abnormality observed in TN. Significant reductions in corneal nerve fiber density (CNFD), corneal nerve fiber length (CNFL), and corneal nerve branch density (CNBD), accompanied by large effect sizes, indicate a distinct neurodegenerative signature detectable by IVCM. The magnitude of corneal nerve loss observed in this study was substantial, with approximately 38% reduction in CNFD, 39% reduction in CNFL, and 38% reduction in CNBD in affected eyes compared with controls, indicating pronounced small fiber degeneration. These findings are supported by prior studies demonstrating that corneal confocal nerve parameters are sensitive and reproducible biomarkers of peripheral small fiber neuropathy in systemic neuropathic disorders, including diabetic neuropathy.12,13 Additionally, morphological abnormalities such as increased nerve tortuosity, fragmentation, focal thinning, and localized nerve loss further suggest an active and progressive neurodegenerative process rather than static nerve damage.
The marked lateralization of corneal nerve alterations to the eyes ipsilateral to the symptomatic trigeminal nerve further supports the functional relationship between trigeminal sensory pathways and corneal innervation. Contralateral eyes demonstrated intermediate corneal nerve parameter values between affected eyes and healthy controls. However, these differences did not remain statistically significant after Bonferroni correction, suggesting that the predominant pathological involvement remains localized to the clinically affected trigeminal side. Nevertheless, the presence of intermediate contralateral values may indicate subtle bilateral neurophysiological changes or early central sensitization mechanisms, which have previously been described in chronic neuropathic pain disorders. To further clarify the interpretation of contralateral eye findings, additional three-group statistical comparisons were performed between affected eyes, contralateral eyes, and healthy controls. While contralateral eyes demonstrated intermediate corneal nerve parameter values, these differences did not reach statistical significance after correction for multiple comparisons. Therefore, although subtle bilateral alterations may suggest early subclinical involvement or central sensitization mechanisms, our findings primarily support localized peripheral neurodegeneration in the symptomatic trigeminal distribution. This cautious interpretation strengthens the biological plausibility of our results while avoiding overestimation of bilateral disease involvement. Because corneal innervation is derived exclusively from the ophthalmic division (V1) of the trigeminal nerve, the observed corneal changes primarily reflect involvement of this branch, even in patients with clinically predominant maxillary (V2) or mandibular (V3) symptoms.Beyond structural neurodegeneration, our findings demonstrate a prominent neuroimmune response at the corneal level in TN patients. Increased dendritic cell density and activated cellular morphology indicate an inflammatory microenvironment associated with trigeminal nerve injury. Previous studies have also demonstrated corneal nerve loss in trigeminal neuralgia without significant differences in dendritic cell density in small patient cohorts, suggesting that inflammatory responses may vary depending on disease stage. 15 Dendritic cells are key mediators of neuroimmune signaling and play a central role in regulating inflammatory cascades and peripheral sensitization following nerve injury. 17 In the present study, descriptive evaluation suggested close spatial association and occasional apparent contact between dendritic cells and subbasal nerve fibers. Although not quantitatively assessed, these findings are in line with previous reports and further support the presence of active neuroimmune crosstalk at the corneal level. Increasing evidence indicates that neuroimmune interactions among neurons, immune cells, and glial cells play a critical role in the development and maintenance of neuropathic pain.18–22 Experimental and clinical studies have demonstrated that chronic peripheral axonal injury may alter immune cell activity and stromal cell behavior through sustained neuroinflammatory signaling, potentially creating a self-perpetuating cycle of inflammation and neurodegeneration.
Anterior stromal involvement observed in patients with longer disease duration provides further evidence supporting progressive corneal tissue remodeling in TN. Increased keratocyte reflectivity and cellular activation have previously been associated with chronic inflammation, oxidative stress, and dysregulation of neurotrophic signaling pathways essential for corneal homeostasis. 23 The preservation of posterior stromal and endothelial structures reinforces the selective nature of TN-associated corneal alterations and supports the hypothesis that peripheral trigeminal nerve pathology is the primary driver of secondary stromal changes.
A major contribution of this study is the demonstration of disease duration-dependent corneal alterations. Correlation and regression analyses revealed that prolonged disease duration is associated with worsening corneal nerve degeneration and increased inflammatory cell density, suggesting that peripheral trigeminal neuropathy in TN represents a progressive biological process. Emerging evidence indicates that delayed diagnosis and prolonged disease duration may result in irreversible peripheral nerve remodeling characterized by reduced regenerative capacity and altered neuroimmune balance. Furthermore, corneal confocal microscopy studies in chronic neuropathic pain conditions have shown that prolonged nerve injury is associated with increased immune cell infiltration and stromal remodeling.24–26 To the best of our knowledge, this study represents one of the first comprehensive demonstrations of disease duration-dependent multilayer corneal microstructural alterations in trigeminal neuralgia using in vivo confocal microscopy.
Receiver operating characteristic analysis in this study identified CNFL as a high-performance parameter for distinguishing disease chronicity, highlighting its potential clinical utility as an objective biomarker for disease staging and longitudinal monitoring. These ROC findings should nevertheless be interpreted cautiously given the subgroup-based exploratory design and require validation in larger prospective cohorts. The identification of reliable imaging biomarkers capable of quantifying peripheral trigeminal involvement is of substantial translational importance, as current TN evaluation primarily relies on clinical symptom assessment and neuroimaging findings, which may not adequately reflect peripheral nerve integrity.
Epithelial alterations observed in TN patients likely reflect impaired neurotrophic support resulting from trigeminal sensory dysfunction. Corneal sensory nerves play a critical role in epithelial maintenance through the release of neuropeptides and growth factors essential for epithelial stability and regeneration. 8 Reduced innervation may therefore predispose to epithelial instability and altered cellular turnover. Similarly, structural disorganization of Bowman's layer may represent secondary changes related to chronic epithelial stress and altered corneal biomechanics. 27
From a clinical and translational perspective, the high interobserver agreement values obtained for corneal nerve measurements confirm the reliability and reproducibility of IVCM as a diagnostic modality. The non-invasive nature of IVCM, combined with its ability to directly visualize peripheral trigeminal nerve terminals, makes it a promising tool for evaluating peripheral nerve involvement, monitoring disease progression, and assessing treatment response. Integration of corneal confocal microscopy into clinical practice may facilitate earlier detection of peripheral neuropathy and improve patient stratification for targeted therapeutic interventions.
The strengths of this study include comprehensive layer-by-layer corneal evaluation, combined quantitative and qualitative morphological analysis, and inclusion of a well-defined cohort of unilateral TN patients with matched controls, which enhances the internal validity and biological plausibility of our findings.
This study has several limitations. First, the cross-sectional design precludes causal inference. Nevertheless, the strong correlations between disease duration and corneal nerve parameters as well as dendritic cell density support the presence of a progressive peripheral neuropathic process in trigeminal neuralgia. Second, the relatively small sample size may limit generalizability; however, the large effect sizes and high measurement reproducibility indicate robust and methodologically sound findings. In particular, the subgroup distribution for ROC analysis was not fully balanced, which may have affected the stability of AUC estimates. Additionally, specific neuropathic features such as microneuromas and bead-like axonal swellings were not systematically quantified, which may have provided further insight into neuropathic structural alterations. Although dendritic cells were descriptively characterized based on morphology and their relationship with nerve fibers, quantitative subclassification was not performed, which may have provided additional insight into neuroimmune interactions. Furthermore, clinical pain severity scores and corneal sensitivity measurements were not included, limiting correlation between structural corneal changes and functional sensory impairment. Neurovascular conflict status was not systematically analyzed, and therefore potential differences in corneal findings according to neurovascular compression could not be evaluated. In addition, medication status was not systematically analyzed in the present study. Because many patients with trigeminal neuralgia receive antineuropathic treatments such as carbamazepine or oxcarbazepine, potential treatment-related effects on corneal nerve morphology cannot be completely excluded. Third, the lack of pre- and post-treatment comparisons restricts evaluation of the potential role of in vivo confocal microscopy in monitoring treatment response. Future longitudinal studies are warranted to assess the effects of medical and surgical interventions on corneal nerve regeneration and neuroinflammatory changes. Finally, the analysis was limited to the ophthalmic branch of the trigeminal nerve, and peripheral extensions of the maxillary and mandibular branches were not directly assessed. Nonetheless, the cornea and limbal region provide a unique and accessible window for evaluating peripheral trigeminal small fiber integrity.
In conclusion, trigeminal neuralgia is associated with significant corneal neurodegeneration and neuroinflammatory activation, primarily affecting anterior corneal layers and the subbasal nerve plexus. These findings support the concept that TN involves progressive peripheral trigeminal small fiber neuropathy. In vivo confocal corneal microscopy emerges as a sensitive, reproducible, and clinically valuable imaging modality capable of detecting these alterations. The strong association between disease duration and corneal microstructural deterioration highlights the importance of early diagnosis and timely therapeutic intervention. Future prospective and interventional studies are warranted to determine whether medical or surgical treatments can reverse or stabilize peripheral nerve alterations and to evaluate the role of IVCM-derived biomarkers in guiding individualized therapeutic strategies and improving long-term clinical outcomes.
Clinical implications
Trigeminal neuralgia is associated with significant corneal nerve loss and increased corneal inflammation.
Corneal microstructural changes become more pronounced with longer disease duration.
In vivo confocal microscopy offers a non-invasive method to assess peripheral nerve involvement in trigeminal neuralgia.
Corneal nerve parameters may serve as potential biomarkers for disease severity and progression.
Footnotes
Acknowledgements
The authors gratefully acknowledge Dr Deniz Kurşun Massimo for her valuable assistance with the statistical analysis of this study.
Ethical Consideration
This study was conducted in accordance with the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board/Ethics Committee of Izmir Bakircay University, Izmir, Türkiye (Decision No: 1925, Research No: 1905, Date: 11 December 2024).
Consent to participate
Written informed consent was obtained from all participants prior to enrollment.
Consent to Publishing
All authors have read and approved the final manuscript and agree to its publication in Cephalalgia if accepted.
Author contributions
Gökhan Aydoğan: Conceptualization, Methodology, Investigation, Data Curation, Formal Analysis, Writing – Original Draft. Murat Kaşıkcı: Conceptualization, Methodology, Supervision, Writing – Review & Editing. Sabahattin Sül: Investigation, Data Curation, Writing – Review & Editing. Gülnihal Kutlu: Investigation, Resources, Writing – Review & Editing. Göksu Alaçamlı: Formal Analysis, Visualization, Writing – Review & Editing. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.