
Abstract
To date, the preponderance of research on infertility in the United States has been conducted with affluent, White couples seeking advanced medical interventions. However, racial/ethnic minorities are equally, if not more, likely to experience infertility in the United States. Drawing on qualitative interviews with 50 African American women of different socioeconomic backgrounds, our study uses an intersectional framework to explore the experiences of African American women who cope with infertility. First, we found that experiencing infertility greatly impaired women’s sense of self and gender identity. Moreover, the imperative to be an African American mother was influenced by an interplay of gendered, racial, and religious mandates. Second, women’s relationships with friends and family members were characterized by a deep sense of silence and isolation; several explanations for this finding are proposed, including stereotypes about African American women’s sexuality. Third, interactions with medical professionals were influenced by women’s multiple social identities, with no single identity conferring an advantage in medical settings. Finally, we highlight several interventions, such as the dissemination of information featuring a greater range of African American women’s reproductive experiences, and we underscore the clinical importance of normalizing African American women’s experiences with infertility, thereby lessening women’s sense of shame and isolation.
Keywords
Many women assume that if they decide to have a child, they will be able to do so when they are ready. Fertility is, in essence, a taken-for-granted aspect of our biological composition—something to protect and control (e.g., with birth control) until the time is right. However, approximately 12% of women (ages 15–44) in the United States have impaired fecundity (an impaired ability to have children, including carrying a pregnancy to term), and 7% of married women between the ages of 15 and 44 meet the criteria for infertility (Chandra, Martinez, Mosher, Abma, & Jones, 2005). For these women, little is experienced as easy or normative about striving to become pregnant. Further, racial/ethnic minority women and women with less education and lower incomes are equally likely, if not more likely, to experience infertility in the United States (Bitler & Schmidt, 2006; Chandra & Stephen, 2010; Jain & Hornstein, 2005). Ironically, however, African American, Arab American, and Latina women are less likely than White women to receive medical services for infertility (Greil, McQuillan, Shreffler, Johnson, & Slauson-Blevins, 2011; Inhorn, Ceballo, & Nachtigall, 2009). Hence, scholars have described this state of affairs as evidence of “stratified reproduction” (Ginsburg & Rapp, 1995), whereby medical resources are used to enhance the fertility of married, high-income, White couples but not the reproduction of less valued, less desirable, brown, and Black babies (Roberts, 1997).
Traditionally, the majority of research on infertility focused on European American, high-income couples seeking services at infertility clinics; this myopic focus on one demographic group occurred, in part, because researchers relied upon the convenience of easily accessible samples (Abbey, Andrews, & Halman, 1991; Abbey, Halman, & Andrews, 1992; Daniluk & Tench, 2007; Greil, 1997; Peterson, Newton, Rosen, & Schulman, 2006). Not until recently have researchers begun to specifically address the infertility experiences of low-income women and Women of Color (e.g., see Becker, Castrillo, Jackson, & Nachtigall, 2006; Bell, 2009; Ceballo, 1999; Greil et al., 2011; Inhorn et al., 2009; Szkupinski-Quiroga, 2007). By examining medical treatment-seeking among Women of Color and low-income women, recent studies highlighted a number of factors that impede help-seeking, such as economic constraints, the lack of private health insurance, perceptions of discrimination from medical providers, and ethical concerns (Bell, 2009; Greil et al., 2011; Inhorn et al., 2009). Despite the existence of a small and important body of work on poor and racial/ethnic minority women with infertility, many limitations in our knowledge about the experiences of racial/ethnic minority women and women who do not undergo highly technical medical interventions remain. In the present qualitative study, we rely on an intersectional framework to examine the experiences of infertile African American women and thereby begin to address this void in scholarly attention and research. Specifically, we examine how infertility influences African American women’s gender identity and relationships with friends, family members, and medical professionals.
An Intersectional Framework
Analytic approaches that are based on intersectionality attend to the meanings and experiences formed by multiple interactions among various social identities, such as gender, race, age, sexual orientation, and nationality (Cole, 2009; Hill Collins, 1986; D. K. King, 1988; Shields, 2008; Warner, 2008). No single social identity encapsulates any person’s experience at a given time. Instead, intersectionality represents the ways in which various social identities are experienced simultaneously, with some identities emerging as more or less prominent and offering greater or less privilege than others in different contexts. Most recently, feminist researchers have called for the need to examine the processes by which certain identities emerge more prominently in certain contexts than other identities (Nash, 2008; Shields, 2008; Warner, 2008). It is critical then to conceptualize identities as part of dynamic processes situated within cultural, social, and historic contexts (Cole, 2009; Stewart & McDermott, 2004; Warner, 2008).
Warner (2008) astutely advises intersectional researchers to explicitly state and explain the reasons why certain identities are chosen for interrogation. In the present study, we investigate how African American women experience infertility because this combination of gender and racial identities has long been overlooked in infertility research. In doing so, we use an intracategorical approach to intersectionality research (McCall, 2005). Additionally, we examine the role of socioeconomic status. Given our society’s adherence to a medicalized model of infertility and an emphasis on medical interventions (Greil, 1991; Harris, 2006), we focus on socioeconomic class as a social category with the potential to impact infertility experiences. Whereas race and gender remain constant in our sample, we include women from different socioeconomic classes in order to compare experiences among African American women across social class locations.
According to Purdie-Vaughns and Eibach (2008), individuals with multiple subordinate group identities, such as African American women (who are neither White nor male), will experience “intersectional invisibility,” a distinctive form of acute social invisibility and oppression. Such invisibility is not limited to academic research but rather includes marginalization in historical accounts, legal representation, political advocacy, and cultural narratives. Infertile African American women are indeed hidden from public view. As with much of the existing research, popular conceptions of infertility draw forth images of wealthy White couples seeking medical interventions. In keeping with a long-standing goal of feminist research (Stewart, 1994), a major aim of the current study is to focus scholarly attention and give voice to an excluded and marginalized group of women who have been left out of existing literature, theorizing, and cultural representations. It is imperative that we investigate those who have been rendered invisible because “rarely is invisibility a value-neutral state” (Warner, 2008, p. 457). For all feminist researchers, studying people who occupy positions of intersectional subordinate group identities provides a framework for examining how social and structural systems interact with different identities, how individuals cope with varying degrees of marginalization, and how different contexts may allow certain social identities to exert greater pull over other identities.
Infertility, Gender Identity, and Motherhood
In the present study, we specifically examine gender identities and the role of motherhood among infertile African American women. Whereas the “motherhood mandate” demands that all women in our society should become mothers, current ideologies of intensive mothering go even further, dictating that good mothering should be an all-encompassing enterprise (Johnston & Swanson, 2006; Koropeckyj-Cox & Pendell, 2007; Russo, 1976). Good mothers will personally, financially, and emotionally devote themselves and center their lives around their children. Based on middle-class, European American, heterosexual standards, these ideologies fuel conceptions of what is valued and defined as normative, while simultaneously devaluing what does not conform to these standards (Hays, 1996). In this overly simplistic, dichotomous paradigm, many conceptions of bad mothering and maternal deviancy center upon African American women as lazy and incompetent “welfare queens,” as mothers who produce “crack babies,” and as emasculating Black matriarchs (Hill Collins, 2000; McCormack, 2005; Roberts, 1997). Together, these images depict African American mothers as unfit, uncaring, immoral, or inadequate. Nonetheless, scholars have identified motherhood as having an especially strong cultural value in African American communities (Hill, 2009). Moreover, for many African American women, good mothering is not an independent, self-consuming endeavor; instead, mothering is embedded in supportive kin networks with the practical imperative of sharing childcare responsibilities (Blum & Deussen, 1996). Thus, the act of mothering by African American women can be, in and of itself, a sign of resistance against denigrating images of Black motherhood as well as a testament to the strength of African American families. What happens then to African American women who want to mother but cannot conceive children (regardless of the particular reason for their infertility)?
Infertility is typically accompanied by a host of negative emotions, such as anger, anxiety, depressive affect, and helplessness (Abbey et al., 1992; Greil, 1997; Greil et al., 2011; McQuillan, Greil, White, & Jacob, 2003). Compared to men, women in infertile couples are more likely to experience negative emotions and to perceive their fertility problems as more stressful (Abbey et al., 1991; Epstein & Rosenberg, 2005; Greil, Leitko, & Porter, 1988). Numerous accounts highlight the tendency for infertile women to feel a sense of inadequacy and failure as women (Greil et al., 1988). Infertility, thus, has a strong effect on women’s sense of self and gender identity. In contrast, men typically report experiencing infertility as “disappointing but not devastating” (Greil et al., 1988, p. 181). However, the preponderance of these findings is based on studies with European American couples. In the current study, we explore how the experience of infertility affects African American women’s sense of gender identity and how gender identity may be simultaneously influenced by race. In other words, how does race alter or compound the influence of infertility on African American women’s sense of themselves as women and potential mothers?
Friends, Family Members, and Medical Professionals
In a pronatalist society that reveres and privileges biological family unions (Mollen, 2014), infertility is likely to affect not only women’s sense of gender identity but their relationships and interactions with others as well. Many women experience the inability to conceive a child as a traumatic and isolating life event. For some, infertility is inextricably bound with feelings of loss, dysfunction, and shame, and infertile women note the social insensitivity of people who pry, question, and assume biological reproduction is a natural, normative, and even necessary adulthood transition (Abbey et al., 1991; Mindes, Ingram, Kliewer, & James, 2003). Not surprisingly, infertility is likely to have a potent impact on women’s relationships with friends, spouses, and family members. Marital relationships may become characterized by frustration and a lack of communication (Greil et al., 1988). Whereas unsupportive social interactions have been linked to greater psychological distress (Mindes et al., 2003), the availability of positive emotional support was associated with better psychological adjustment for infertile couples (Daniluk & Tench, 2007). Once again, however, the limited research in this area is primarily based on European American couples.
Finally, we examine African American women’s relationships with medical professionals and doctors in particular. The medicalization of infertility is firmly entrenched in our society, such that infertility is commonly viewed as a biological impairment or disease requiring medical intervention (Greil, 1991; Harris, 2006). By this definition, infertility is not simply a natural part of social life, but a medical condition requiring treatment. Medical professionals thus control the implementation of policies dictating who will and will not receive medical assistance to conceive children. In the United States, seeking medical services for infertility is positively associated with older age, a college education, high income, and being of European ancestry (Bitler & Schmidt, 2006; Chandra & Stephen, 2010; Jain & Hornstein, 2005; Staniec & Webb, 2007). Unable to make use of good health insurance or personal wealth, poor women are often excluded from obtaining medical care for infertility.
The lack of available medical care for some, but not all, women bolsters dominant narratives about good, deserving mothers, that is, those who are well educated and middle- or upper-class. In a study of 20 poor, racially diverse, infertile women, Bell (2009) depicted a large communication gap between highly educated doctors and low-income women. As a result of negative interactions with physicians, many of the poor women in Bell’s sample gave up on medical treatments entirely. By focusing on interactions between African American women and medical professionals, we examine the intersection of race and class in these professional relationships. Hence, it is important that we place these interactions within social and historical contexts. Numerous historical accounts document the racially biased and harmful treatment of poor African Americans, such as the Tuskegee Syphilis Study (1932–1972) and the eugenic programs of nonconsensual sterilizations in the 1960s and 1970s (Roberts, 1997; Stern, 2005; Washington, 2006). In this context, African American women may understandably harbor a healthy suspicion and distrust of medical professionals.
The Current Study
To the best of our knowledge, ours is the first study to focus exclusively on the experiences of African American women with infertility. As an initial foray into the experiences of African American women who cope with infertility, qualitative methods constitute an appropriate research approach. Scholars have long maintained that qualitative methods are advantageous when studying topics about which little is known (Marecek, Fine, & Kidder, 1997). In our society, certain women are encouraged to reproduce whereas other women, mostly poor women and Women of Color, are actively discouraged or denied the means to reproduce. Moreover, medical and political institutions support stratified reproduction as, for example, when Medicaid covers contraceptive methods to limit reproduction among poor women but rarely covers infertility treatments to enhance reproduction for low-income women (L. King & Meyer, 1997). Consequently, policies and social opinions favoring stratified reproduction are likely to influence poor African American women’s self-perceptions, relationships with friends and family, and interactions with medical professionals. Our study will thus explore the following three research questions from an intersectional perspective: (a) How does the experience of infertility affect African American women’s sense of gender identity? (b) How does the experience of infertility influence African American women’s relationships with friends, spouses, and family members? and (c) How are interactions between medical professionals and infertile African American women influenced by gender, race, and social class?
Method
Participants
Participants (N = 50) ranged in age from 21 to 52 years with a mean age of 37 years. The majority of the women (n = 36) were married, 7 were single, and 7 were separated, divorced, or widowed. These African American women represented a diverse range of educational backgrounds, incomes, and occupations. Fully 28 of the women had obtained college degrees, 19 had graduated from high school, and 3 women did not complete high school. Among the women who did not have college degrees, several were employed as custodians, factory workers, and nurses’ aides. Those with more advanced professional degrees were employed as social workers, nurses, and professors. Whereas most of the women (n = 37) reported working full-time, seven were employed part-time, and six were unemployed. About one third (36%) reported annual household incomes of under US$50,000. In total, our participants were a socioeconomically diverse group of women who met two criteria: (a) they self-identified as African American and (b) at some point in their lives, they met the medical definition for infertility. No age restrictions were applied to our recruitment procedures. Table 1 presents demographic information for each of our participants, identified by pseudonyms to ensure confidentiality, and it provides background information for each participant to complement the quotes presented in the Results.
Participants’ Background Information.
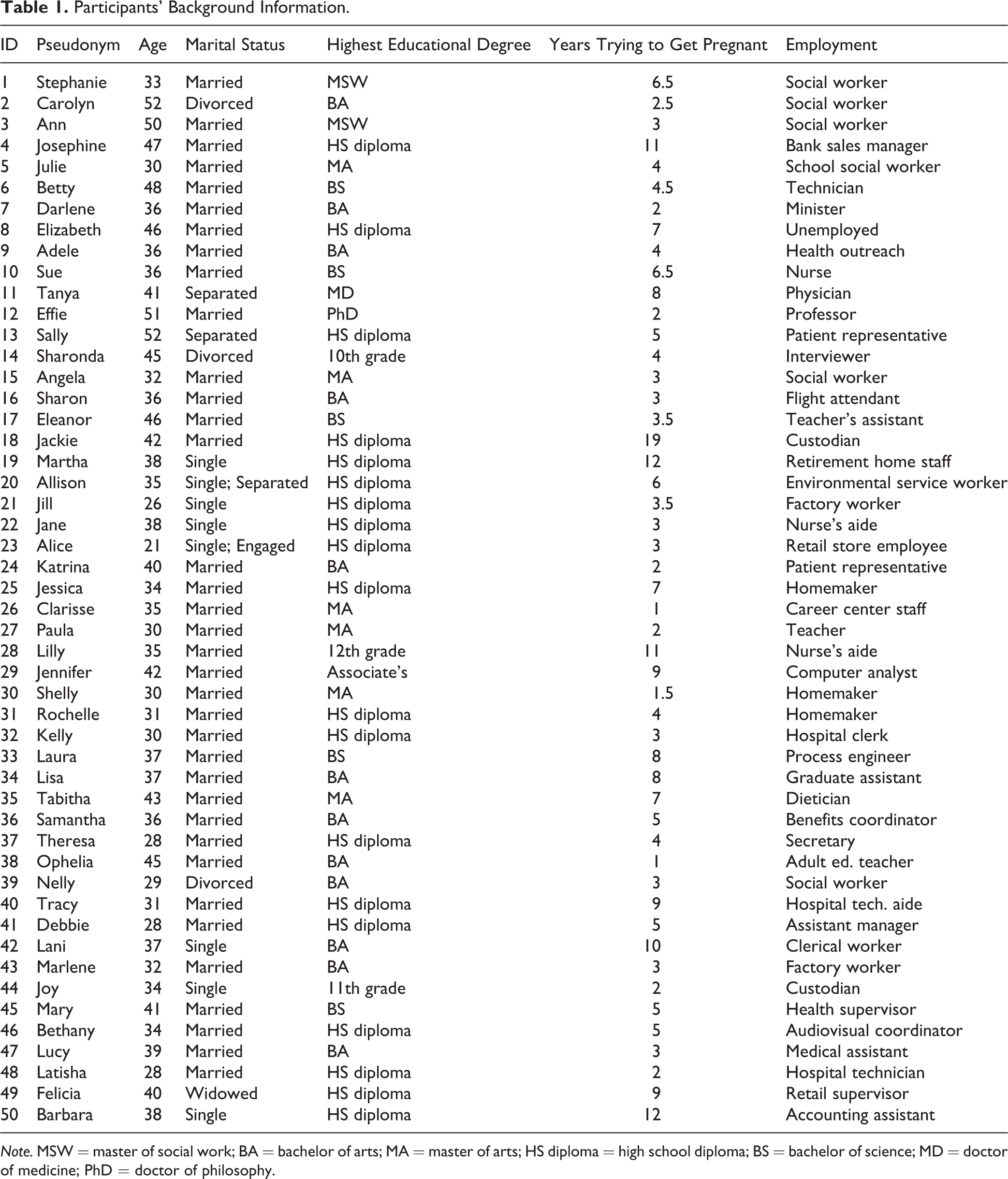
Note. MSW = master of social work; BA = bachelor of arts; MA = master of arts; HS diploma = high school diploma; BS = bachelor of science; MD = doctor of medicine; PhD = doctor of philosophy.
The standard medical definition of infertility refers to a woman who has been unable to conceive after 12 or more months of regular, unprotected sexual intercourse (American Society for Reproductive Medicine, 2008). The women in our sample had spent from 1 to 19 years, with an average of 5.4 years, trying to become pregnant, and at the time of the interview, 24 were trying to have a baby, and 2 women were pregnant. Nine of the women in our sample experienced secondary infertility, meaning that they could not conceive after 1 year of unprotected intercourse following a previous successful pregnancy and childbirth. Few of the women had tried assisted reproductive technologies, treatments that include the handling of eggs and/or embryos. Specifically, only three women in our sample had tried in vitro fertilization (IVF); all three were able to use insurance to cover some part of the cost of IVF. Finally, it is important to note that none of our participants was recruited from medical offices specializing in infertility treatments.
Procedure
Women were recruited in a U.S. Midwestern state, with no mandated insurance coverage for infertility treatments, via two recruitment strategies. First, recruitment relied upon posting flyers about the study in churches, community centers, Ob/Gyn waiting rooms, and adoption agencies. Second, the first author received assistance from the department of obstetrics and gynecology at a university hospital. The department chair agreed to mail recruitment letters to all African American female patients who had, at some point, received a diagnosis of infertility and who had visited their Ob/Gyn physician in the past 2 years. Both flyers and recruitment letters described the study and protections of confidentiality and instructed women who wished to participate to call the first author to schedule an interview at their convenience. Because our initial recruitment conversations indicated that some women did not like the sense of finality associated with the word, “infertile,” we stopped using this term. Instead, we changed our recruitment materials and interview protocol to refer to “difficulty getting pregnant for over a year.”
For this study, either the first or the third author interviewed each woman; at the time, we were a Black Latina professor of psychology and women’s studies and an African American female graduate student in public health with a doctoral degree in history. We conducted in-depth, semi-structured interviews with each of the participants. All interviewers and participants were thus matched on gender and race/ethnicity to increase participants’ comfort with discussing sensitive personal information regarding gender and race. The interviews lasted about 2 hours and were mostly conducted in the participants’ homes (but some were conducted in church offices, public parks, and coffee shops). Every interview was tape recorded and later transcribed by a professional transcriber. Participating women were paid US$35 as a token of appreciation.
After reading and signing the consent form, participants completed a brief demographic questionnaire. A recorded interview followed using a semi-structured, open-ended format. The interview began by asking women to describe their own narrative account of their difficulty getting pregnant. The interviewer explained, “I would like to learn about your experience as you would describe it to someone in your own words.…I’d like to start by having you tell me your story from the beginning, when you first started trying to have a baby, until now.” Next, specific interview questions were organized around the following themes: discussions with others (e.g., “Who did you talk to about your difficulty getting pregnant? How did talking about it with those people make you feel?”), relationships with partners (e.g., “How did the difficulty getting pregnant affect your relationship with your partner?”), seeking medical help (e.g., “Did you ever discuss your difficulty getting pregnant with a medical professional?”), and gender identity/images of mothers (e.g., “How important was it to you to become a mother?”). It is worth noting that the interview did not include any questions about race or discrimination specifically; however, if women raised these topics themselves, we inquired about their views and experiences as thoroughly as possible. Throughout the interview, we asked follow-up questions in order to seek clarity and to ensure we understood the woman’s intended meaning.
Qualitative Interview Coding
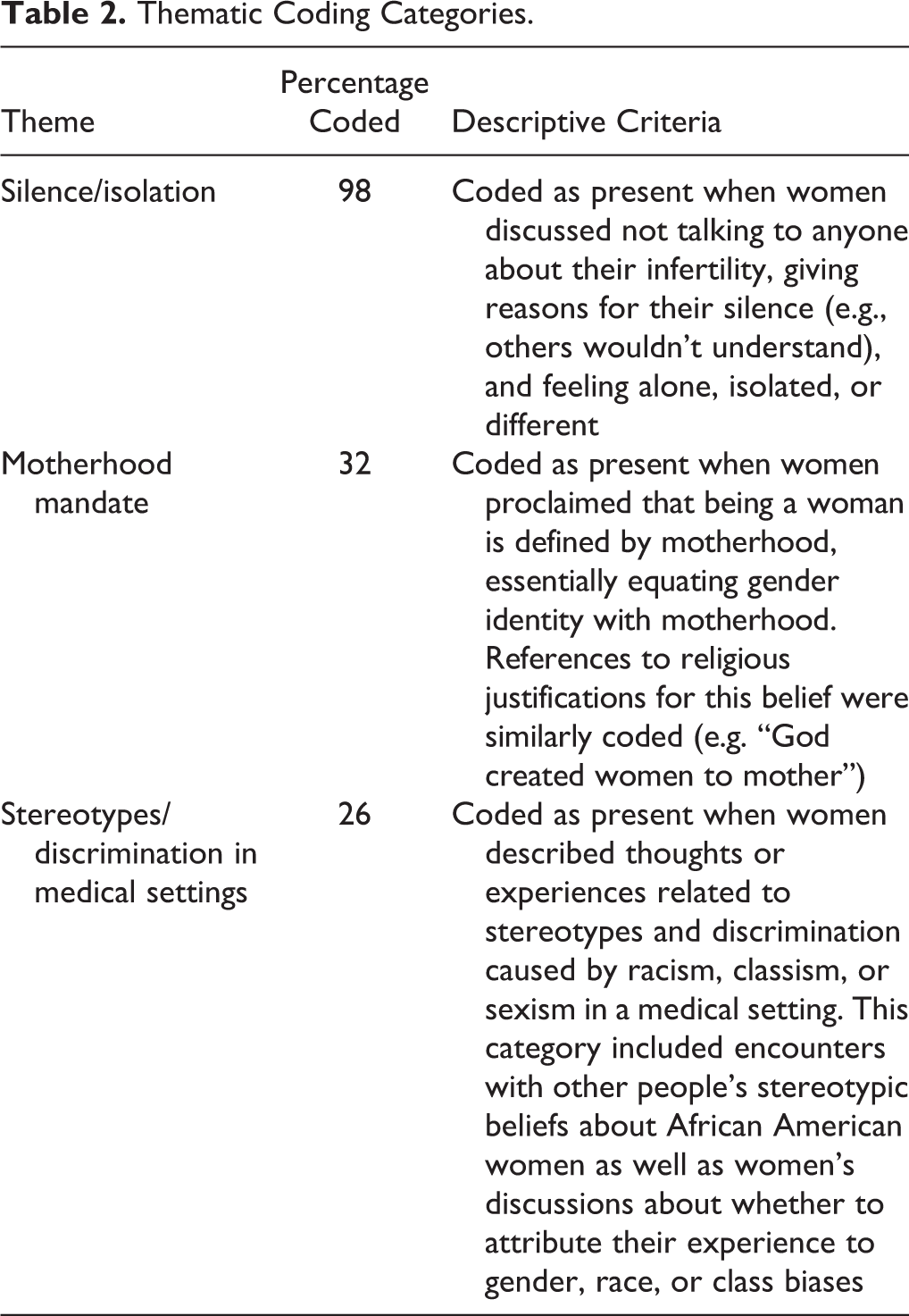
Initial analyses coded categorical responses to some of the open-ended interview questions that were asked of every participant. These included questions about medical interventions tried, things that made women feel better or worse, whether and how they reached a sense of resolution, advice for other women who have difficulty conceiving, and views about adoption. Relying upon multiple close readings of several interview transcripts and grounded theory principles (Strauss & Corbin, 1998), the first author next identified several emergent, recurrent themes. Following lengthy discussions about the parameters of these categories with the second author, both authors established detailed coding criteria. Detailed descriptive coding criteria for each of our themes are displayed in Table 2. The first and second authors coded each interview, highlighting the presence of themes whenever they emerged in the interview. For each interview transcript, we coded every passage that indicated the presence of three themes: (a) silence and isolation, (b) the motherhood mandate, and (c) stereotypes and discrimination in medical settings. Percentage agreement was used as the index of inter-rater reliability, with our reliability falling above 85% and above 90% on a majority (n = 42) of the interviews. Afterwards, discrepancies in codes were resolved by extensive conversations and continued reliance upon our initial criteria for thematic coding. In addressing the potential for confirmation bias, our procedures identified “negative cases” in our coding whereby a majority of the sample did not meet the coding criteria for the motherhood mandate or “stereotypes/discrimination in medical settings.”
Thematic Coding Categories.
Results
In addressing our first research question about the influence of infertility on women’s gender identity, we relied on coding for the theme of the motherhood mandate (e.g., being a woman means being a mother). Our second research question centered on the influence of infertility on women’s relationships with friends, spouses, and family members. For this question, we highlight our coding of women’s experiences with “silence and isolation.” Lastly, we focus on the coding of “stereotypes and discrimination experienced in medical settings” when examining women’s interactions with medical professionals.
Gender Identity and the Motherhood Mandate
In response to our first research question, the women described infertility as impairing their sense of self and their sense of being a woman. Our qualitative coding of the motherhood mandate revealed that 32% of the women discussed stereotyped beliefs that equated being a woman with mandatory motherhood. These women shared similar refrains, such as, “All women feel like there’s this maternal instinct.… If you have that instinct and you don’t get the opportunity to do it, it does take something away from your womanhood” (Sharonda); “Emotionally, I felt that I was not complete, because I had not had a child. I didn’t feel like I was a complete woman” (Tracy); and “I think that having a child would complete me” (Jessica). Moreover, once women identified themselves as incomplete women, they subsequently viewed themselves as flawed and deficient in fundamental ways. Sue described it this way: “It [having no biological children] would label you as a failure, as a failure in being a whole male or a whole female.” Explaining the effect of infertility on her self-esteem, Adele said, “It does a lot to your self-esteem. That’s a hurt feeling, that you can’t do something, in my mind, as simple as have a baby. I mean, there are a lot of women that don’t have college degrees or a lot of women that don’t drive. There are a lot of women that can’t do math. Have a baby, I mean, that’s not a lot to ask.”
Scholars have identified the motherhood mandate as our society’s directive that all women should mother; in essence, the mandate posits that to be a woman is to be a mother (Johnston & Swanson, 2006; Koropeckyj-Cox & Pendell, 2007; Russo, 1976). For some of the African American women who endorsed the motherhood mandate, the mandate did not stand alone. Rather, it was infused with religious significance and import. For instance, Marlene explained, “That’s what God created women for—to produce,” and Lucy similarly asserted, “It’s like my whole purpose is to have children and multiply, like it says in the Bible.” Lucy went on, describing her strong desire to use her body as “a gift from God to create new life.”
At times, the motherhood mandate was interwoven with racialized expectations of motherhood. African American women were expected to marry and reproduce, thus fulfilling their roles as Black wives and mothers. This is perhaps best illustrated in a passage from Effie who explained how motherhood was equated with being a “good” Black woman as well as a good Black wife: I was not a good woman. Good women got pregnant. Good women, I married a Southern person, so there’s a lot of stuff wrapped up in this geographic regional difference thing. You didn’t ask questions. You did what you were told. And you certainly produced an heir, within the next year. (Effie)
We next examined whether there were social class differences among the 16 women in our sample who expressed a belief in the motherhood mandate. We used having a college degree as a proxy for socioeconomic class. Interestingly, we found no differences in women’s endorsement of the motherhood mandate: all eight women without college degrees and all eight women with college degrees supported the motherhood mandate. Similarly, there were no social class differences in women who did not endorse the motherhood mandate. Further, we investigated whether women who were advocates of the motherhood mandate would engage in more medical interventions. For all the women in our study, we created a total sum of the number of medical interventions tried. We counted a total of 16 possible interventions from minimally invasive treatments (e.g., semen analysis, basal body temperature charting, and postcoital test) to more cumbersome interventions (e.g., artificial insemination, IVF, and use of a surrogate mother). Once again, we found no difference in the number of medical treatments tried between women who endorsed the motherhood mandate, averaging 3.7 medical interventions, and those women who did not express support for the motherhood mandate and averaged 3.6 interventions. Relatedly, women who supported the motherhood mandate were not more likely to be women who did not have children (biological or adopted) or women who were currently trying to get pregnant. Thus, expressions of support for the motherhood mandate appeared to operate independently from women’s educational attainment, from their decisions to pursue medical treatments, and from their current status as someone trying or not trying to get pregnant.
Even though some women did not endorse the motherhood mandate, only three women directly contradicted the motherhood mandate in their interviews. Jackie, a 42-year-old, married woman who worked as a custodian, once believed that “if you can’t have a baby, you’re not a full woman,” but at the time of the interview, she reflected, “that’s not true.” Likewise, Jill, a 26-year-old factory worker, declared, “I don’t feel that I’m less of a woman because I can’t have children, because I know that’s not the case.” In line with the motherhood mandate, virtually all the women identified becoming a mother as very important to them personally. Moreover, some women expressed belief in ubiquitous Black fertility. In this sense, a parallel to the motherhood mandate emerged, an equally strong belief in what we will call a Black fertility mandate. The Black fertility mandate represents the simple, yet stereotypical, assumption that all African American women are fertile; in our sample, it was discussed by women across all social class groups. For instance, Adele conceptualized infertility as an experience that “didn’t happen to us [African American women].” Similarly, Josephine explained, “For so many of my sisters, it’s just not a problem getting pregnant. The problem is trying not to get pregnant,” and Laura recounted, “Most of the Black people that I have known have not had a problem with it [infertility] ever.” Finally, belief in the Black fertility mandate and the motherhood mandate are not, by any means, mutually exclusive; some women endorsed the motherhood mandate while also expressing belief in ubiquitous Black fecundity.
Silence and Isolation
Our second research question explored the influence of infertility on African American women’s relationships with friends and family members. Virtually all the women in our sample described silence and isolation as defining features of their relationships with other people. All but one of the women (98%) interviewed mentioned silence, loneliness, and/or isolation at some point during the interviews. Even when there were a handful of people (e.g., a friend, a mother) who knew about a woman’s difficulty conceiving, the women did not discuss their experiences and feelings with others in a meaningful way. In describing her experience, Stephanie, who tried to get pregnant for 6.5 years, said, “I didn’t even tell my close friends. I didn’t even tell my mother, we were very close, or my sister. My sister’s a year younger than me. I didn’t even tell her.” She went on, “I hid it for so long … keeping it as a shameful secret.” Felicia disclosed, “I haven’t let people get close to me or in my life since this.” Providing a rationale, Bethany said, “I just don’t want to bother anybody with it. I just feel like it’s a private thing.”
According to some women interviewed, the experience of infertility was not as emotionally painful for husbands and partners. For example, Laura, a married woman with no biological children, said, “I don’t really feel like we’re going through it [the medical treatments for infertility]. I’m going through it. I feel like I’m really going through it. I’m the one that’s troubled and he’s not.” Similarly, Carolyn recounted, “I don’t feel that he [her husband] was committed as much as I was, in terms of having a baby. And, it was really me, and I knew it was me. It was my need. And, I was willing to go through whatever it took.” Still, it is important to note that these were the women’s perceptions, not their partners’, and similar interviews were not conducted with the women’s male partners. Further, it is important to tease apart whether gender differences in emotional responses to infertility are due to actual differences in experiences or to gendered differences in talking about emotionally laden topics.
Indeed, the women in our sample imposed distance in their relationships with spouses and partners. For example, Tabitha matter-of-factly said, “I prefer not to talk to him [her husband].” Stephanie described purposely crying alone, “When I would cry, I wouldn’t let my husband see me, but would go cry to myself and pray, and just ask God for deliverance.” Samantha somewhat apologetically said, “I know it’s [a baby] something he [her husband] definitely wants, and he knows it’s something that I definitely want. But, for some reason, we don’t talk about it. I mean, we talk about it—only to the extent that it’s necessary.” In fact, some women justified their silence by describing their husbands as “non-talkers.” Even if they wished to discuss things with their partners, these women nonetheless refrained, accommodating their husbands’ preferences and prioritizing their husbands’ needs above their own. From this perspective, Lani did not want to burden her partner: “He didn’t really want to talk about it a lot. I guess ‘cause to him, he said if he kept talking about it or thinking about it, it would make him sad. The opposite of that was, I told him, that talking about it for me was comforting.” Although not all couples underwent these experiences in relative silence and distance from each other, the majority of women in our sample described experiencing extreme loneliness and identified few, if any, people with whom they felt comfortable talking about their experiences with infertility.
The pervasiveness of the experience of silence and isolation among the African American women in our sample is noteworthy. As a theme that was present in all but one of our interviews, silence existed across all educational levels, household incomes, and degrees of involvement with medical treatments. The one exception was a participant who was diagnosed with a chronic illness that explained her infertility. Based upon our participants’ responses, we propose five explanations to account for the frequency with which silence and isolation were expressed and use interview quotes to illustrate our explanations. We do not, however, intend these explanations to be mutually exclusive and propose that several factors are likely to simultaneously influence women’s silence.
First, reproductive difficulties are, by nature, a personal and private matter. When compounded by an impaired sense of self and gender identity, as is often the case with infertility, feelings of shame and failure may understandably lead to withdrawal and isolation. Debbie illustrated these feelings by explaining, “It’s kind of embarrassing not to be able to produce. It’s embarrassing because everybody, I mean, mostly everybody is producing [children]. I’m sitting here not, and my husband’s wanting it, and, you know, I feel kind of ashamed.” Moreover, because pregnancy is visibly located in women’s bodies, women may be more likely than men to feel ashamed and to blame themselves for infertility.
Second, women may not talk about their difficulty conceiving because they believe there is little utility in doing so. Women may reason that other people can neither change their infertility status nor understand what they were experiencing. In our sample, this sentiment was especially true for women who were struggling with secondary infertility. Joy recounted, “Most everybody I know has kids. They would probably say, ‘Well, what do you want to do with more kids?’” Similarly, Allison, who had one biological daughter, tried to explain her longing for another child: “I only want one more. I only want one more. You know everybody be like, ‘You’re crazy. Why would you want more kids?’” Confirming the general lack of sympathy for secondary infertility, Lisa said, “They all say, ‘Well, at least you have one.’” Women with secondary infertility, in particular, learned that they were unlikely to receive sympathy or empathy from talking to others.
A third explanation for African American women’s silence on this topic may be linked to cultural expectations about privacy in African American communities. For example, Samantha said, “You don’t want people in your business. You know, we’re taught to keep things to ourselves.” From this perspective, keeping personal matters private provides protection from authority figures (e.g., teachers, social workers, doctors) and people outside the community who may be unlikely to understand how African American families negotiate survival. For some women, a code of silence may be part of belonging to a disadvantaged and stigmatized racial/ethnic group. Ann, a married social worker, explained, “I never said anything to anyone else, because in our culture … it was not something that you shared.” In essence, some African American women view their silence about reproductive difficulties as supporting racial solidarity by hiding their own personal vulnerabilities from public view.
Fourth, Hill (2009) posits that negative cultural images surrounding African American women have, more recently, been replaced by exotic images of strength and motherhood, characterizing African American women as having unusual stamina, independence, and perseverance. In this light, African American women may remain silent about reproductive problems because they believe they should be able to handle these difficulties alone, as strong self-reliant women. Rationalizing her silence, Marlene said, “It was something I had to sort out within myself and deal with it.… I dealt with a lot of issues on my own.” In a similar vein, Kelly explained her desire not to talk to others, “I’m not talking about that, you know what I’m saying? Yeah, I don’t have kids, but girl, I’m alright.” According to this cultural stereotype, African American women can handle problems without help, companionship, or support from others. As Hill (2009) posits, however, such a response to traumatic life events may be detrimental to African American women’s psychological well-being.
Finally, fueling the sense of isolation described by the women in our sample was the internalization of stereotypes about African American women’s hyper-fertility or belief in a Black fertility mandate, claiming that all Black women are invariably fertile. This particular stereotype about reproduction applies specifically to women who occupy the intersection of female gender and African American race. Despite their personal experiences with infertility, as previously discussed, many of the African American women in our sample believed that they were an anomaly—an abnormal exception to the status quo—and thus different from other African American women who have a propensity for reproducing. For instance, Lisa recalled, “Like my friends who weren’t able to get pregnant, they weren’t African American. So I didn’t know anybody who was [African American] that had [a problem]. It just seemed all the Black women I knew were just pretty fertile.” Similarly categorizing all African American women as fertile, Eleanor explained, “I think they [Black women] have a problem with not having so many [babies], but not with getting pregnant.” Ironically, stereotypes about the promiscuity and hyper-fertility of African American women served to silence and render invisible those African American women who did not conform to these images.
Feeling different or abnormal went hand-in-hand with images of what the typical infertile couple was supposed to look like in our society: infertile couples were wealthy and White. None of the African American women whom we interviewed discussed seeing images of other women who looked like them coping with infertility. The sense of being the only one, the only African American woman with this problem, was compounded by experiences in medical clinics and hospitals. Shelly recalled, “I felt alone out there, you know. And so with me, every time I went to the doctor’s office, I was like the only [African American] one in there.” Likewise, Ophelia described viewing the publicly posted baby photos at a hospital’s infertility clinic: “I saw all these pictures of these babies, but I didn’t hardly see any Black babies.… When I looked at those pictures, I think I saw one Black baby.” Going beyond medical settings, Samantha discussed the role of the media in perpetuating these stereotypes: I didn’t think there were that many African American women out there that were having this problem. I mean, you know, because nobody talks about it and you know, there’s nothing ever on the media about it. I mean, the media represents us as popping out babies left and right. You know, we’re welfare mothers, we’re this and that, you know, so I didn’t think there was a problem with us. (Samantha)
Stereotyping and Discrimination in Medical Settings
In our final research question, we examined how interactions between medical professionals and infertile African American women are influenced by gender, race, and social class. On a practical level, it is important to note the typically large differences in power and status between physicians and patients. In their positions of authority, physicians hold access to medical knowledge and information while simultaneously serving as gatekeepers who can provide or limit treatment options. Bell (2009) highlighted the fact that medical settings accommodate middle-class interests by easily serving those who can flexibly schedule appointments and use medical insurance. The women in our study all occupied multiple subordinate group identities, as women, as African Americans, and for some, as low-income women. Given social stereotypes about African American women’s promiscuity, hyper-fertility, and bad neglectful mothering, it is not surprising that some of the women in our sample reported experiences of discrimination in medical settings.
In coding stereotypes/discrimination in medical settings, we found that 26% (n = 13) of the women interviewed described encounters with medical professionals that may have been influenced by gender, race, and/or class discrimination. These women talked about doctors who made assumptions about their sexual promiscuity and their inability to pay for services or support a child. Whereas only four women who were not presently trying to conceive were coded for this category (Josephine, Sue, Sharonda, and Mary), nine women who were currently trying to get pregnant (Katrina, Lilly, Kelly, Ophelia, Lani, Joy, Bethany, Lucy, and Latisha) discussed stereotypes and discrimination in medical settings. It stands to reason that women who were trying to become pregnant and pursuing medical treatments at the time of the interview would be more likely to discuss experiences in medical settings in general. Further, we do not know to what extent women who were no longer trying to get pregnant may have forgotten unpleasant encounters in medical settings or simply wished not to talk about them.
It is equally important to note that there were also women who described positive and supportive interactions with doctors. For example, Angela’s first pregnancy ended in a stillbirth, but as a positive outcome, she described meeting a physician with whom she would develop a strong and trusting relationship. She remembered: Thank God for him [the maternal fetal expert] because one of the things that he said to me was, “I want you and your husband to come in for preconception counseling before you decide to try again.” And he said, “Because it’s a lot harder to lose a baby a second time, and I want to make sure that you don’t have any questions or doubt, any problems, physical or emotional.” (Angela) And the doctor that I was seeing at that time, I expressed my concerns about children and me wanting to have children [in the future], and so he knew exactly … I felt that it was the only option that I had. I thought that when they say, “tie your tubes,” because I was so young and so naïve, when they say, “tie your tubes,” I thought they just tied them or clamped them [so they could later be untied]. They never educated me.… I was starting to just can’t stand men. You know, they treat you so bad. Then, when I meet someone that’s nice and treats me good, then maybe I can go ahead and have the surgery and have it reversed, and we can have children. (Bethany) I have ran into other women that have had the same physician and I talked to this one White lady and she told me if you ever needed me to tell someone else what he told me. She said, “I had been through a divorce and everything.” She was 25 and she already had three kids. And he told her, “No, you’ll find another nice guy and you’ll probably get married again,” and he refused to do it [sterilize her]. (Bethany)
In contrast to the discriminatory experiences reported by Bethany, we expected that having an advanced educational degree and a professional career would help shield women from discrimination in medical settings. In this conceptualization, social class would confer privileges that could buffer women from the disadvantages associated with their race and gender identities. However, as before, we did not find social class differences in the reporting of stereotypes and discrimination in medical settings. Utilizing college degrees as a proxy for socioeconomic status, seven women without college degrees (Josephine, Sharonda, Lilly, Kelly, Joy, Bethany, and Latisha) and six women with college degrees (Sue, Katrina, Ophelia, Lani, Mary, and Lucy) were categorized as discussing stereotypes and discrimination in their interactions with medical professionals.
Contrary to our expectations, highly educated women with higher incomes were equally likely to report experiences of discrimination and doubt when recounting interactions with medical professionals. In talking about the doctors whom she saw, Mary concluded, “I don’t think they [the doctors] had that concern for me as a Black woman trying to get pregnant.” Here, Mary clearly tied the absence of receiving serious medical care to her identity as a “Black woman,” identifying the intersection of both her gender and racial identities as salient. As a college-educated woman, Mary did not identify her education or social class position as providing any advantage in the care she received. Even African American women with advanced educational degrees and professional careers described feeling a loss of control and an absence of agency when interacting with doctors. Julie, a 30-year-old social worker, wished her doctors had shared more information with her. She said, “I would have liked more information about different varieties of drugs …. I feel like, [it was] just, ‘Trust what I say type of thing.’” Effie, a college professor, succinctly explained, “You didn’t get to talk. You, the patient. You got to lie on the table, let them play with you.”
Additionally, middle-class African American women reported that the costs of fertility treatments were prohibitively high. In discussing IVF, Sharon, a college-educated flight attendant, said, “We’re talking for this whole procedure, I think it was going to be about $30,000 …. There’s some people out there that really have a lot of money to burn, and they want this child to be their husband’s child, and they’re willing to spend that, and they’re willing to do it over and over and over again.” By contrast, Sharon explained that she did not come close to having that kind of affluence. Whereas low-income women in our sample could not even try certain medical interventions, women with higher incomes might attempt certain treatments, but their efforts were typically quite limited. Women discussed both the high cost of treatments, alongside their low probability of success, as deterrents to pursuing these types of medical interventions.
As women who occupy several subordinate social identities, some of the women who reported experiencing stereotypes and discrimination also discussed thinking about which of their identities might account for the way they were treated. Although a cornerstone of intersectional theory is the idea that our experiences are best captured by the interactions between people’s multiple social identities, some of our participants tried to identify which one of their identities was most responsible for a particular experience. Debating the possible role of race, for example, Sharonda remembered, “The fertility specialist that I was referred to was a Caucasian man in an all-White suburb, and I didn’t feel comfortable. There were some issues, and I don’t know if you could say they were personality clashes or racial.” Also wondering about the influence of race, Sue said, “You would think people in the medical profession would be more sympathetic, but you would be surprised. I don’t know if it’s my race.”
Nor were these internal ruminations limited to questions of race. The nuances and subtleties of social interactions left some women questioning whether a prejudicial or discriminatory experience was due to their race, marital status, weight, or social class. Katrina, a college-educated woman with no biological children, recalled that within a span of 10 days, she learned that she was pregnant, her doctor suspected a tubal pregnancy, her tube ruptured, she had emergency surgery, she lost her tube in surgery, and she lost her baby. Katrina could discount social class, to some extent, because she had medical insurance, but she specifically wondered about the role of race and weight in her experiences. She explained, “Well, I mean, there is always the racial issues. You have health insurance and all that. I wonder about that, you know, race, and then too, my being a large woman, because people are very biased about that.”
Discussion
Drawing upon narrative and qualitative interview data, our study is one of the first known studies to exclusively examine the experiences of African American women with infertility. Moreover, we study experiences with infertility by interrogating the points of intersecting gender, race, and social class identities. In this way, we delve into “the place where African-American women live, a political vacuum of erasure and contradiction … existing within the overlapping margins of race and gender discourse … it is a location whose very nature resists telling” (Crenshaw, 1992, p. 403). We hope that our findings represent a first step toward de-cloaking the intersectional invisibility (Purdie-Vaughns & Eibach, 2008) that has hidden the experiences of infertile African American women for so long. Accordingly, an intersectional analysis helps illuminate how policies of stratified reproduction combine with dominant social narratives about good, deserving, White mothers to facilitate the reproductive health needs of more economically privileged women while virtually erasing the needs of poor women and Women of Color.
For many women, including those in our study, infertility is not experienced as a single event but rather is experienced as a “chronic crisis” and a “secret stigma” (Whiteford & Gonzalez, 1995). Not surprisingly, women also report that infertility erodes one’s sense of self and gender identity (Abbey et al., 1991; McQuillan et al., 2003). About one third of our sample expressed belief in the motherhood mandate, equating being a woman with being a mother. For these African American women, the inability to fulfill a motherhood directive was imbued with meanings related to racialized gender expectations. Against a backdrop of social inequalities, an imperative to reproduce is promulgated among African Americans. Further, this reproductive imperative is strongly tied to religious doctrines and expressions of racial solidarity, fostering resistance to a historical legacy of slavery and oppression (Mitchell, 2004) and to present-day, controlling images of African American women as unfit, promiscuous, irresponsible mothers (Hill Collins, 2000; McCormack, 2005; Roberts, 1997). Consequently, when African American women cannot conceive a child, it harms their sense of themselves not only as women but as Black women. Interestingly, in our sample, African American women of all educational levels were equally likely to endorse the motherhood mandate as well as the Black fertility mandate. Moreover, women who pursued medical interventions were not more likely to endorse the motherhood mandate. Understandably, then, if a woman views Black fertility as ubiquitous and motherhood as a necessary component of being a woman, infertility threatens the core of one’s gender identity.
Relationships with friends and family members were also influenced by infertility; indeed, silence was the primary characteristic defining African American women’s relationships with others. Every woman in our study (except for one woman who suffered from a chronic illness that explained her infertility) referred to silence and isolation as part of her experience with infertility. Even relationships with partners and spouses were not spared from a sense of loneliness and distance. Thus, silence emerged as a defining characteristic of African American women’s experiences—irrespective of income level, educational attainment, primary versus secondary infertility, and the pursuit of medical treatments. The sense of silence pervading our participants’ narratives was most likely caused by a number of interacting factors. More specifically, we proposed five possible explanations for women’s silence: (a) feelings of shame and personal failure; (b) a sense that other people would not understand; (c) cultural expectations about privacy in the African American community; (d) the cultural myth about African American women’s strength, self-reliance, and ability to overcome challenges; and (e) the internalization of stereotypes promoting Black sexuality with abundant fertility.
It is equally possible that self-imposed silence may serve as a survival strategy that is used by African American women as a protective shield. This may be particularly true for women who occupy multiple devalued social positions by virtue of their race, social class, and absence of children. In this manner, silence shields women’s sense of shame, difference, and personal failure from public view while also preserving African American cultural notions of keeping personal issues private. Relatedly, Dodson and Schmalzbauer (2005, p. 950) proposed that poor women cultivate a “culture of silence” as a way to manage daily discrimination and derogatory stereotypes. Rather than try to explain their situations to unsympathetic welfare workers, for example, poor women remained silent, avoiding lengthier interrogations. Further, Thomas, Hacker, and Hoxha (2011) noted that young girls are socialized to develop a sense of strength and self-determination as an important part of their social identity as African American women. In contrast to the fragility attributed to White female firefighters, Yoder and Berendsen (2001) similarly demonstrated that African American female firefighters were stereotyped as being strong and capable of managing heavy work, thereby forcing them towards greater self-reliance. Although maintaining strength in silence as a coping strategy may bestow certain benefits, it may also bring disadvantages. By embodying the myth of the superhumanly strong Black woman silently managing difficulties on her own, African American women may miss important opportunities to receive emotional support from others (Hill, 2009). Paradoxically, coping in silence further compounds a sense of isolation via the silencing of other African American women experiencing infertility.
Stereotypes and cultural ideologies construct what we come to view as reality and truth, thereby imposing different roles on members of different social groups. Importantly, stereotyped images not only influence advantaged members of society but also impact the beliefs and ideologies of the very people who are being stigmatized. As Patricia Hill Collins (2000, p. 69) theorized, such “controlling images” become “instruments of power” over others. As an example, many of the African American women in our study wholeheartedly believed that they were abnormal, socially bizarre outliers among the populace of African American women because they could not have children. They did not see other people like themselves—African American, female, and infertile. Infertile African American women internalized the public, hegemonic images of abundant Black female sexuality and fertility with their own personal and private experiences of infertility. Ultimately, they came to believe the controlling images of infertility as an upper-class, White woman’s problem and thereby facilitated their own marginalization and social invisibility.
It is important to note that the women we interviewed did not subscribe to the many negative stereotypes about African American women. Although they were strongly influenced by the preponderance of images representing White infertility and Black fecundity, they did not describe themselves or other African American women as unworthy of mothering or as sexually promiscuous. Perhaps African American women have acquired an arsenal of strategies to deflect blatantly negative stereotypes. Even so, the African American community’s silence around reproductive problems leaves women with little support to counter stereotypes about race and fertility. In a similar vein, we expected that socioeconomic privilege would assist higher income women in negotiating interactions with medical professionals. Instead, we found that women highlighted instances of discomfort, mistreatment, and discrimination in medical settings regardless of their socioeconomic status. Although financial resources (e.g., health insurance) provided access to medical treatments and care, economic resources did not buffer women from gender and racial discrimination. Thus, money does matter, but in these circumstances, it did not supersede race or somehow bar racial discrimination.
Interestingly, as women with multiple subordinate social identities, our participants sometimes ruminated over which particular social identity accounted for the way others treated them. Whereas in most instances they described their experiences as strongly influenced by the interplay of racial, gender, and class identities, in these self-ruminations, they tried to tease apart which singular identity was accountable. At first glance, this appears to contradict theories of intersectionality. However, Bowleg (2008) similarly described women who did not know if an experience was due to sexism or racism or heterosexism. In the end, we concur with Bowleg that in the process of questioning, these women posed a fundamentally intersectional question. They were not denying the importance of multiple identities; rather, they were wondering about the prominence of different identities in a particular context. In other words, they were inquiring about the salience of their identities (e.g., race, marital status, weight, social class) in a specific contextualized setting. Presumably, ruminating over multiple devalued social positions is likely to be more stressful than considering just one devalued identity. Equally as important, the awareness that a social identity marker (e.g., race) may have influenced their experiences did not make these women feel better or more empowered in their interactions with medical professionals.
Limitations
As with all research, our study presents several limitations. First, some women provided retrospective accounts of highly traumatic events, and personal biases may certainly influence such recollections. For instance, compared to women who were trying to get pregnant at the time of the interview, the women who had had a biological child may recall experiences differently. Second, about half our sample was recruited from an Ob/Gyn department patient list. Although this was not an infertility clinic patient list, it may nevertheless have biased our sample towards women who were more positive about medical services. Finally, it is important to note that we used solely open-ended questions in our semi-structured interview protocol. In other words, we did not directly ask women if they believed in the motherhood mandate or if they experienced discrimination in medical settings. Therefore, our coding of themes allows us to report that 32% of the women expressed belief in the motherhood mandate, but it does not allow us to confirm that other women did not endorse the motherhood mandate. It may be that the motherhood mandate was not discussed because it was not supported; however, it is also possible that it was not discussed because an opportunity to do so did not emerge during the interview. Similarly, although we can report that 26% of the women discussed experiences of discrimination in medical settings, it would be wrong to infer that 74% of the women had solely positive interactions with medical professionals.
Practice Implications
In spite of these limitations, our study helps to illuminate African American women’s experiences with infertility. In doing so, our interviews were also a form of intervention. Many women were pleased by the simple fact that a study was focusing on African American women. Some expressed comfort, affirmation, and relief in learning, after the interview, that infertility was not a rarity among African American women. Katrina described her reaction to receiving a recruitment letter: “When I get this letter, I was like, ‘What? Other African American? What? Really!’” Similarly, in explaining why she did not talk to anyone, Adele said, “Because I never knew before you [the interviewer] told me that the literature supports that there are Black women that have this problem.” At the end of the interview, women often told us that they thought it would be enormously reassuring for other Black women “to know that they’re not the only one” (Lisa).
The implications of our findings firmly support the dissemination of information that counters stereotyped images of Black women’s fertility and portrays a greater range of Black women’s reproductive experiences. Care should be taken to display images of women from many different racial groups on educational and medical materials regarding infertility. Clinically, the importance of normalizing the experience of African American women who face infertility is paramount. Our study suggests that self-imposed silence results, in part, from women’s internalization of racial and gender stereotypes about Black women’s abundant fertility. Hence, simply knowing that you are not alone—that there are other African American women with infertility—can lessen women’s experiences of shame and isolation. Additionally, having an opportunity to talk to other Women of Color who have experienced infertility was also frequently suggested by the women in our study. As an example, a “support list” of racial/ethnic minority women who have experienced infertility and are willing to be contacted could be given to Women of Color seeking advice from primary care physicians, therapists, or ministers. These are rather low-cost interventions that may positively influence women’s psychological well-being in important ways.
Further, medical efforts that attend to a range of treatments for infertility are equally important; health care professionals should not neglect low-cost medical alternatives and preventative efforts that may curtail the development of infertility in the first place. Although it was not a focus of the current article, we would be remiss not to emphasize the importance of changing societal structures and policies that serve to limit options for poor women and Women of Color, such as the absence of national health care (until recently) and punitive welfare policies.
Conclusion
Although far more work needs to be done on the experiences of poor women and racial/ethnic minority women and men coping with infertility, our study, as the first known to focus exclusively on African American women, makes an important contribution. For virtually all the women in our sample, silence emerged as a defining and painful feature of their experience; this was true irrespective of women’s income, education, and involvement with medical interventions. Similarly, endorsement of the motherhood mandate, equating being a woman with motherhood, occurred across income and educational levels, explaining, in part, why infertility impaired women’s sense of gender identity. Finally, higher socioeconomic status did not buffer women from experiences with stereotypes and discrimination in medical settings. As previously noted, these findings have important implications for public health policies, medical outreach efforts, and feminist theories about daily, lived experiences of intersectionality.
Footnotes
Authors’ Note
Erin T. Graham is now in the U.S. Navy, and Jamie Hart is now at Atlas Research, Washington, DC.
Acknowledgment
We are indebted to the women whose courage inspired their willingness to participate in our study. Additionally, we are grateful for the research assistance provided by the following undergraduate students: Dayana Kupisk, Cecilia Kraus, Jennifer Ortiz, Rukiya Wideman, Gina Willis, and Sonya Zarkhin. Finally, we wish to express our deep appreciation for vital assistance with this research and thoughtful feedback on this article provided by Matthew Countryman, Timothy R. B. Johnson, Sara McClelland, and Abby Stewart.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Institute for Research on Women and Gender (IRWG), the Office of the Vice President for Research (OVPR), and the Department of Obstetrics and Gynecology at the University of Michigan, Ann Arbor.