
Abstract
In this qualitative study, I offer a feminist reflection on motherhood from the perspectives of 25 women with various types of physical and sensory disabilities. Disability was treated not only as an individual experience but also as a social construct. I conducted 25 non-standardised narrative interviews with women with various types of physical disabilities. Using grounded theory method, with a particular emphasis on symbolic interactionism, I identified three important themes from the non-standardised narrative interviews: the effects of insufficient health care on pregnant women, the lack of acceptance and support for mothers, and a welfare system inadequate to the needs of mothers. These themes affect the way Polish women with disabilities experience motherhood. Findings highlight the different ways that mothers with disabilities challenge the prevailing normative categories of gender and disability and, in so doing, demythologise and delegitimise the traditional Polish model of motherhood. While this study points to needed reforms in Poland to support women with disabilities, it also reveals a model of motherhood based on interdependence and mutual care. The women with disabilities in this study identify new possibilities for all families.
Motherhood among women with disabilities has rarely been a topic of social research. Disability research almost never includes a gender perspective, and feminist research often omits the experience of women with disabilities. One of the most important issues in contemporary feminist thought is the right to make informed decisions about procreation. Among women with disabilities, the central issue is how to combat prejudices that deny their femininity by preventing them from confronting and challenging stereotypically feminine roles (Lloyd, 2001). Supporting the reproductive decisions of women with disabilities is an important avenue for redefining social perceptions regarding femininity and motherhood (O’Toole & Doe, 2002). In this article, I explore motherhood among women with disabilities, defined both as an individual experience and as a social construct. I attempt to demythologise and delegitimise the stereotypic image of a mother in Poland. My results reveal that women with disabilities often deconstruct the traditional parental practices and, thus, show that motherhood is variable and multidimensional.
Motherhood in Polish Culture
In Polish society and culture, the roles of men and women are clearly separate and considered to be both natural and normatively appropriate. For a woman, the central point in her self-definition is motherhood. As Anna Titkow (2007) noted, in Poland there is a “social imperative to give birth” (p. 196). The figure of the Polish Mother is the dominant role model, which limits other social roles of women. It is one of the most culturally ingrained representations of femininity in Poland. The cultural standard for women is the “good mother.” An extremely durable component of this standard is the imperative for the mother to be independent, self-sufficient, and willing to make sacrifices for the good of the family (Titkow, 2007).
Both male and female politicians emphasise that the role of a woman is primarily to be a wife and a mother (Kotowska, Sztanderska, & Wóycicka, 2007). At the same time, the real needs of women in the sphere of social benefits and the welfare system are being neglected. Some examples of that neglect are discrimination against mothers in the labour market, low welfare benefits for single mothers, the dissolution of the alimony fund, and the mass closure of public nurseries and kindergartens (Hryciuk & Korolczuk, 2012). It can be said that the social policy in Poland corresponds to a “managerial matriarchy” model (Titkow, 2007), according to which a woman has to deal with numerous obligations herself, without any support, while being treated as a cultural icon. Such a conception of the maternal role, also held by women themselves, is used by the state in requiring women to act as a buffer, absorbing the social costs of any systemic change (Lister, 2003). The current system undermines the legitimacy of the demands made by women and consequently hinders collective emancipatory actions.
Demographic indicators and sociological research (Hryciuk & Korolczuk, 2012; Titkow, 2007) suggest that the archetype of the Polish Mother is slowly becoming an inadequate model in the current sociocultural environment. Yet, it still has enough prestige to delegitimise certain behaviours of women. Women who decide to choose another way of life (e.g., childlessness by choice, economic migration) or different practices of motherhood (e.g., motherhood in single-sex families) are met with silence, negative social assessment, and stigma (Hryciuk & Korolczuk, 2012). In addition, the existing abortion ban (The Family Planning, Human Fetus Protection, and Conditions of Permissibility of Abortion Act of 1993), which limits access to contraception and sex education, nullifies a woman’s right to decide about her own life. Despite changes in the character of motherhood and women’s identity in the last 30 years in Poland, the societal constructs described earlier have remained generally unchanged. In spite of the new vision of a civil society promoted after the end of Communist rule in Poland in 1989, the tendency to reduce women to the roles determined by gender has only intensified (Titkow, Duch-Krzystoszek, & Budrowska, 2004).
Motherhood Among Women With Disabilities
The total number of women with disabilities of childbearing age is uncertain; and little is known about their rates of fertility, pregnancy, or birth. Still less is known about their individual experiences related to motherhood. However, the available international research shows that women with disabilities face various obstacles regarding their reproductive rights (Grue & Laerum, 2002). According to that research, the family rights of women with disabilities (e.g., the right to start a family and live in relationships of their own choosing, the right to procreation and motherhood, the right to have access to current knowledge about contraception and to contraceptives) are not respected worldwide mainly because of stereotypes and strong prejudices (Arnade & Haefner, 2011). These stereotypes and prejudices portray women with disabilities as dependent on others, passive, weak, and lonely. Women with physical disabilities are viewed as not able to undertake family and care roles or to assume responsibility for the lives of others. They are also excluded from fulfiling traditional female roles because they are perceived as childlike and asexual (Nosek, Howland, Rintala, Young, & Chanpong, 2001b). These stereotypes often have a deleterious impact on their self-esteem, self-determination, and self-efficacy (Crawford & Ostrove, 2003; Malacrida, 2007).
Women with physical disabilities are also confronted with the stigmatisation of their disabilities. They have to deal with social assumptions about their lack of aptitude for parenthood, which may in turn provoke social exclusion and surveillance (Malacrida, 2007). The feeling of being under a societal magnifying glass, coupled with the fear that their mothering will not “measure up,” can lead to stress and anxiety (Malacrida, 2007; Prilleltensky, 2003). Societal attitudes discourage mothers with disabilities from applying for services that could facilitate their mothering and force them to make huge efforts in order to show that they are able to provide care for their children (Thomas, 1997). Moreover, the societal belief that women with disabilities cannot handle responsibility, reinforced by concerns that a woman could pass on her disability to her child (Kent, 2000; Saxton, 2000), makes mothers with disabilities highly susceptible to the risk of major human rights violations, such as forced abortions (Arnade & Haefner, 2011; Asch, 2000; Kent, 2000) or forced adoptions (Kerr, 2000). Tarleton and Ward (2007) reported that only marginal support is offered to parents with learning disabilities, and in many cases it is limited to crisis interventions. In addition, women with disabilities have limited access to adequate obstetric care and consultation during pregnancy because they are considered a high-risk group (Radomski, Jarząbek-Bielecka, Sowińska-Przepiera, & Milewczyk, 2010). However, research shows that properly invested resources and a consistent support system allow women with disabilities to satisfactorily fulfil the role of a mother (Walsh-Gallagher, Sinclair, & McConkey, 2012).
Women with physical disabilities are aware that they are embedded in networks of dependencies, which they often use in order to meet maternity needs and responsibilities (Malacrida, 2007). Dependency is not always negative; it can be a source of strength, connection, and identity. The lives of individuals with disabilities are characterised by “interconnections with, and interdependencies upon, the body, others, and the structures of the world” (Ells, 2001, p. 600). This positive model of human interaction and self-development is accomplished via relations of care and interdependencies. The importance of retaining control over the parental role has been identified as an important factor among mothers with physical disabilities who needed assistance to perform caring tasks (Prilleltensky, 2003).
Motherhood Among Polish Women With Disabilities
In Poland, the state’s role in supporting people with disabilities and their families is limited. Social welfare institutions for people with disabilities are scattered, and there is no mechanism that would automatically trigger a public welfare response to difficulties faced by an individual. A person must request support, and the state is not required to meet the need (Woźniak, 2008). This, in effect, shifts the responsibility for navigating the system from the state institutions to a person in a difficult situation. Moreover, the system of social benefits for people with disabilities and their families offers little financial support and depends on many factors, such as the degree of disability, the financial situation of the person applying for assistance, prior and current professional activity, and inability to work. The only form of non-financial support offered is care service, which may be granted to a single person who is deprived of help from others, including family (Woźniak, 2008). Care service may include time-limited support in meeting everyday needs as well as hygienic care prescribed by a doctor (The Social Assistance Act of 2004, 2013).
Polish women with disabilities often remain in partner relationships because of economic dependency, inadequate social policy, and structural constraints. The lower social status of women, compared to the social status of men, and the low value placed on the work they do for the family (Titkow et al., 2004), leads to frequent economic dependence on a partner or family members. Lack of sufficient institutional support further limits opportunities for women with disabilities to enter the labour market. All of these factors affect the capacity of women with disabilities to assume maternal roles.
While legal regulations in Poland do not prohibit people with disabilities from exercising parental authority, there is still a lack of sensitivity concerning the rights of a person with disabilities to be a parent. In 2012, Poland ratified The Convention on the Rights of Persons with Disabilities (United Nations Organization, 2006). However, at the same time, the government made a statement of interpretation and reservation to Art. 23 paragraph 1 of the Convention, which refers to the right of persons with disabilities to start a family and to the elimination of discrimination with respect to marriage, parenthood, and relationships. This statement raises questions about (a) the conditions that must be met by a woman with a disability who wishes to have offspring and (b) the degree of her disability, which may be seen as an obstacle to parenthood or can even exclude her from the group of persons who have the right to start a family.
The Current Study
My aim in the current qualitative study is to offer a feminist reflection on motherhood from the perspectives of Polish women with physical and sensory disabilities. The research also was designed to apply the concept of gender to disability research. There is a lack of research in this area, especially in the Polish social and cultural context. Twenty-five non-standardised narrative interviews (Schütze, 2011) were conducted with women with various types of physical disabilities. Each interview was developed around the central research question: “What does being a mother with a disability mean to you?” I examined the experiences of women with physical and sensory disabilities who are in opposition to normative cultural systems within the categories of both gender and disability. I argue here that the qualitative study can be viewed as a systematic attempt to provide a new model of motherhood.
Method
Participants
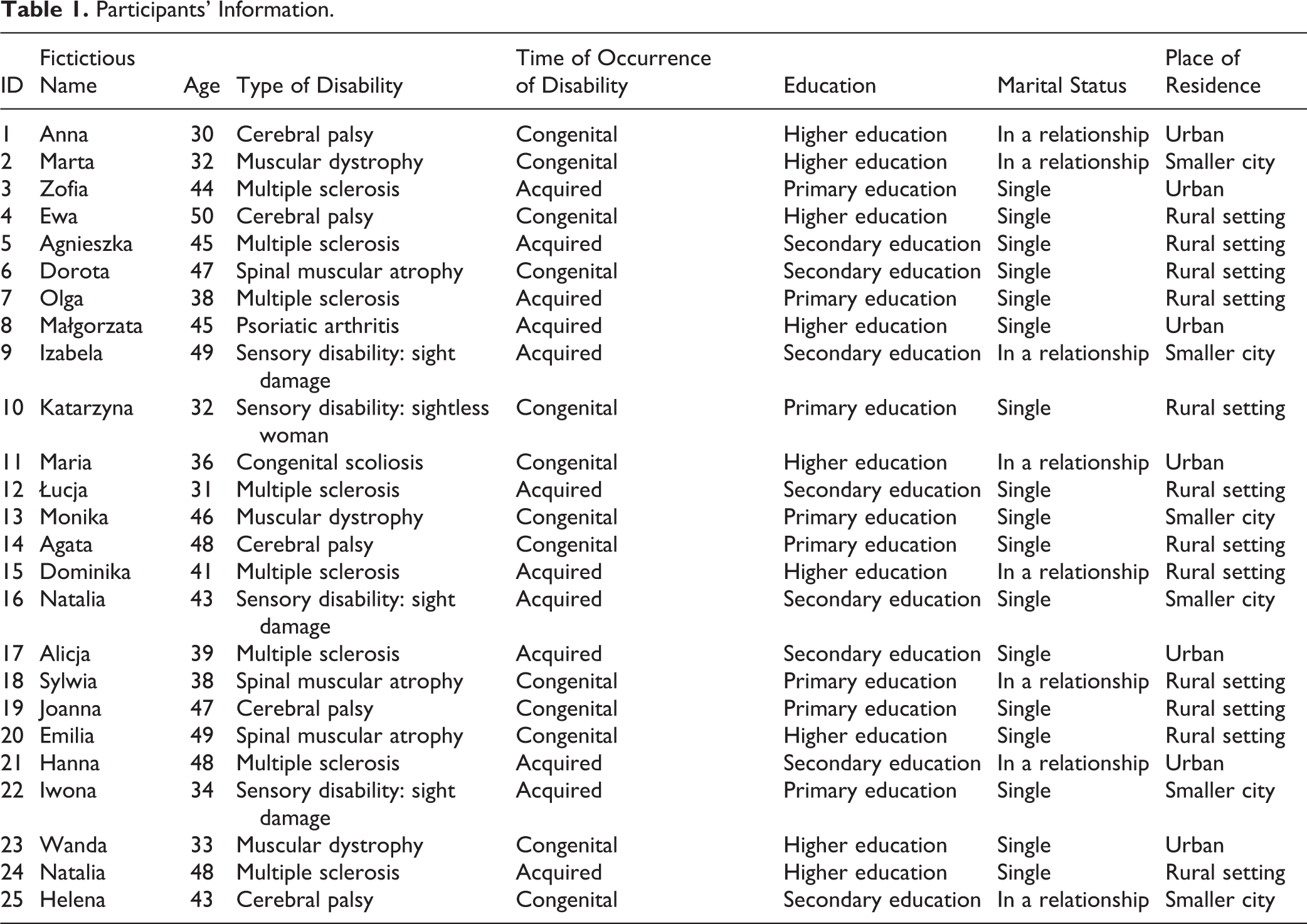
I conducted narrative interviews with 25 Polish mothers with physical and sensory disabilities. The selection of interviewees was deliberate and based on age (over 18 years old), education level (at least completion of secondary school), legal situation (the certificate of disability), and residential environment (I sought geographical diversity). Each interviewee signed a written consent confirming her participation in the study. The respondents’ ages varied between 30 and 50 years (M = 41.44, SD = 6.58). Thirteen women had a congenital disability and 12 had an acquired (e.g., from illness or accident) disability. The women had attained different levels of education: tertiary (n = 9), secondary (n = 8), and primary (n = 8) and were from different regions of Poland, including urban (n = 7), smaller city (n = 6), and rural settings (n = 12). Eight of the interviewees were married or were cohabiting with a partner, while the rest (n = 17) were single mothers, six of whom were divorced. See Table 1 for detailed information. Women with mental illness and intellectual disabilities were not included in this study.
Participants’ Information.
Researcher as a Non-Disabled Person
My encounters with interviewees explored traditional power relations, multiple meanings of disability, and the researcher’s “temporary able-bodiedness” (Whyte & Ingstad, 1995). During the interviews with women with disabilities I, as a non-disabled researcher, tried to emphasise and understand their subjectivities. The choice of a qualitative method required me to abandon the privileged position of a distant observer. As interviewer, I was an engaged, open person interested in establishing direct contact with the interviewees. In addition, I presented my findings to each of the interviewees to ensure that the categories that were used in the analyses accurately reflected their view of the world (communicative validation). This procedure helped me to avoid both a paternalistic approach and any distortion of meanings ascribed by the interviewees to their experiences.
Procedure
Recruitment
I identified interviewees using snowball and criterion methods (Rubin & Babbie, 2010). Respondents were sought through organizations (e.g., nongovernmental organizations that work with people with disabilities) and on Internet blog sites. I gave no external pressure to participate, and no one indicated any discomfort during or after the interview regarding my recruitment strategy. Participants did not receive any type of remuneration for the interviews, and they were informed of this during the first interview.
Interviews
The study was conducted in Poland between September 2013 and January 2014. All interviews were conducted in Polish because all interviewees and the researcher are Polish citizens. The interviews were tape recorded and transcribed in Polish. The data from the interviews were coded using Atlas-ti (version 6), a qualitative data analysis software package. All interviewees were assigned fictitious names. Analyses were conducted in Polish. The article was translated into English by a bilingual translator for purposes of publication in this journal.
I conducted the interviews in comfortable conditions specifically adjusted to the interviewees’ needs and capabilities. The interviews took place in an area proposed by the interviewees, mostly in their homes. Interviewees were told they might stop the conversation at any time. The interviews lasted from 90 to 120 minutes and were recorded on a voice recorder. I used a narrative interview (Schütze, 2011), which is similar to in-depth, free conversations. Through follow-up questions, I sought to provoke the interviewees to tell a story of their experiences with motherhood.
Grounded Theory Analysis
I used qualitative research methods, which play an important role in psychological and sociological feminist studies (Olesen, 2007; Prilleltensky, 2003; Willig, 2013) and in research on disability (Mayes, Llewellyn, & McConnell, 2011; Morris, 1995; Soares & Carvalho, 2009). I analysed the information shared during the participant interviews using analytical methods that align with grounded theory (GT; Charmaz, 2006; Glaser, 2001; Schütze, 2011), with a particular emphasis on symbolic interactionism (Strauss & Corbin, 1990). GT was chosen as the methodological framework because it involves building a theory on the basis of systematically obtained data that directly relate to the observed aspect of social reality (Clarke, 2003; Glaser, 2001; Levitt & Ippolito, 2014). GT methods make it possible to comprehend the individual’s subjective experiences in relation to the studied phenomenon.
My analysis of the transcribed interviews was guided by GT principles, which include limiting the researcher’s preconceptualisation and focusing on theoretical sampling. I divided the data into smaller units, called incidents, which I then conceptualised and related to other incidents. My general analytical procedure was to constantly and iteratively compare incidients (Charmaz, 2006).
In open coding, which was the first phase of the analysis, incidents were coded and compared so they could then be categorised using the language in the data. In this process, I observed the emergence of initial categories, which were compared to one another according to their common meanings and grouped into higher order categories. This procedure led to the identification of the commonalities and differences among interviewees. Using inductive analysis, I was able to support, revise, or abandon a category title (Rennie, 2012). In this way, I developed a hierarchy of categories, culminating in one core category that reflected the central meaning in the analysis (Charmaz, 2006). This process was continued as new units were added to the analysis until the point at which incoming data no longer seemed to evoke new understandings. The decision to stop the data collection process was determined by saturation—the point where new data appeared to be redundant and no new categories emerged from the inclusion of additional data. The saturation point occurred after the 25th interview.
Credibility checks
I conducted several credibility checks to assess the thoroughness of the interviews and to safeguard that the research was reliable. The reliability, accuracy, and relevance of the data were examined by (a) making continuous comparisons, looking for another case to confirm the initial sets of themes; (b) analysing cases that deviated, listening to divergent ideas until the recurring themes were derived; and (c) by repeatedly listening to the recordings, during which previously overlooked themes were discovered.
To check my interpretation of the interviews, I invited three competent judges to analyse the data. They were mothers with disabilities, who did not participate in the study but had knowledge and experience of being a mother with physical disabilities. Each judge evaluated each of the 25 interviews twice. For the first evaluation, I gave judges the interviews with the incidents that I had identified highlighted. The judges were instructed, “Read the text [interview transcript] carefully. Then re-read the highlighted fragments of the text, and assign each fragment a label that describes the problem identified in this fragment. You can select any number of fragments and use any number of labels.” Each judge assigned labels to the highlighted incidents (e.g., unpreparedness of doctors, unpreparedness of midwives, and lack of procedures). When the labels given by the judges agreed with the categories I had earlier assigned to the same incidents, I assigned the category to the fragment.
The judges conducted a second reading of each of the interviews with each fragment highlighted and coded with a category. They rated each fragment on a 7-point scale (1 = lack of consistency and 7 = very high consistency) to assess the degree to which they agreed with categories assigned to the interview data. Judges’ average assessment was 6.7. I concluded that the judges agreed with my interpretation of the data, that it was not an over-interpretation, and that it represented authentic patterns of experiencing motherhood among Polish women with disabilities.
Results and Discussion
In my analysis of the narrative interviews, I sought to understand the experience of motherhood among women with physical and sensory disabilities and to discover the multidimensionality of their experiences. I divided the results of my analysis of the interview data into three main emergent themes: (a) the effects of insufficient health care on pregnant women, (b) the lack of acceptance and support for mothers, and (c) a welfare system inadequate to the needs of mothers. Each theme contains a number of subthemes, which I analyse further. In the following sections, I present a number of practices that undermine motherhood among women with disabilities, the consequences of these practices, and women’s ways of coping with the consequences. I identify challenges posed by social systems that exlude women, and I describe strategies for dealing with challenges in everyday experience, revealing an important area of knowledge about social relations (Crisp, 2002; Parish, Magaña, & Cassiman, 2008). The Polish women I interviewed exposed a fracture in the traditional model of motherhood.
The Effects of Insufficient Health Care on Pregnant Women
Participants described a number of organisational and psychological barriers to the comfortable experience of pregnancy and childbirth. The most commonly reported barrier to the full expression of the maternal role was a health care system unprepared to take care of and support pregnant women with disabilities. The women criticised the standard institutions for being unable to support maternal functions or to offer specialized services dedicated to women with disabilities. The theme of a health care and welfare system unprepared for cases of pregnancy of women with disabilities occurred in most interviews.
Organisational barriers
Among the most common organisational barriers pregnant women with disabilities faced were: hospitals were unprepared to deal with these patients, facilities were unavailable in general, patient rights to information were denied, and facilities were not tailored to the needs of this group of patients. The women reported they usually had difficulties in finding a doctor and a pregnancy midwife because they were considered a high risk group. The interviewees reported that the lack of professional help, and the fact that the gynaecological room and hardware were not adapted for women’s disabilities, often led to an environment devoid of intimacy.
While the doctor was kind and helpful, it was difficult for me to bear the humiliation. Together with a paramedic—one grabbed me by the hands, the other by the legs—they literally had to rock me and “toss” me on the armchair. I would not want to go through this once again.
Psychological barriers
The women also suffered from the practices of personnel who infantilized their patients, for instance, by addressing them in the third person and expressing negative opinions regarding their maternity plans. The interviewees described barriers including a general lack of understanding and awareness, lack of constructive mechanisms to resolve a situation, and the staff’s lack of knowledge. In combination with humiliating experiences with gynaecologists, these barriers lead to the conclusion that “if you’re a woman with a disability, sex is no longer an unambiguous matter” (Anna). Scholars have argued that society treats disability as a major status which marginalizes other statuses and excludes other identities (Olsen & Wates, 2003). “To see ‘disability’ is never to see ‘a person’” (Sprague & Hayes, 2000, p. 681). As Natalia said, “The wheelchair seems to suggest the existence of a medical microcosm around me, in which there is no room for anything else. As if I did not exist outside of my disability.” The women described how the medicalization of pregnancy and childbirth led to downplaying the significance of their experience. Some of them also experienced unnatural, intensive, even aggressive observation from a number of professionals while in the hospital after giving birth; this constant presence resulted in a sense of abnormal isolation and vulnerability.
Everyone looked significantly at each other; no one has talked to me, not even responded to my questions. That was when I felt most alone.
Isolation leads to the objectification of women. This may manifest as an expert discourse, which intrudes on women’s individual choices (Hryciuk & Korolczuk, 2012). Women described their experience with medical staff who either showed disbelief about their maternity plans or imposed certain reproductive choices.
She bluntly assessed my idea of having a child as stupid, though there were no medical contraindications.
I heard midwives talking among themselves, “and this one is pregnant?”
When I was diagnosed with a small lump in my womb, the doctor said, authoritatively, “Cut it out, after all, you would not give birth anyway.”
Some interviewees experienced total indifference from medical staff. They also pointed to the lack of specialist knowledge about pregnant women with disabilities.
In maternity wards, women with disabilities were faced with degrading treatment. They were assumed to be incompetent at reading the signals from their own body, or professionals believed they underestimated the impact of their disability on parturition. This attitude denied the rights of patients to health care and took away women’s control of their pregnancy and childbirth even further.
When I told the doctor that I thought I was having cramps, he shouted at me, “It is impossible, you cannot feel the contractions!” I shouted back in desperation: “I’m not paralyzed, just blind!”
The birth was difficult because the midwife told me to give birth naturally; it was the fashion then for such births. I told her that I could not monitor the birth, because I did not feel the contractions. I had to beg long for caesarean section.
Many women also said that medical staff attempted to convince them to have an abortion or put the baby up for adoption. Suggestions to acquire alternative childcare are in violation of women’s rights. Such ideas create the sense that disability is the basis of their self-definition and that disability status completely determines their ability to care for and educate their children (Olsen & Wates, 2003). A woman with a disability having a child is therefore frowned upon and subject to an unfavourable evaluation from the outside society, indicating a still-functioning discourse of negative eugenics (Zames Fleischer & Zames, 2011).
The doctor stated that in her opinion—even though no one asked her for her opinion—it’s an unnecessary risk of “breeding crippled beings.”
The decision to have a child is an individual matter. However, the interviews show that it is common practice to invade the privacy of women with disabilities who are deciding whether or not to have a child. Women reported great difficulties in accessing health care that meets high standards. They reported that professionals relegate decision-making regarding the sexual life of women with disabilities to private medical care. The limitations described above have emotional and economic costs, making it difficult for women to implement decisions related to the role of the mother (Meekosha, Shuttleworth, & Soldatic, 2013). It should be noted, however, that all interviewees have overcome barriers associated with a drastic lack of institutional support, by developing creative ways to cope with and fulfil maternal functions (Grue & Laerum, 2002; Malacrida, 2009).
It looks like that if one of us finds a sympathetic gynaecologist, who is a good doctor, and in addition does not make big eyes because of a woman in a wheelchair, he’ll fall a victim to women with disabilities who recommended him among themselves and he begins to specialize in women [with wheelchairs].
The Lack of Acceptance and Support for Mothers
Polish society is not ready to accept and provide specialized support for mothers with physical and sensory disabilities in at least three different areas. First, as described by participants, society lacks acceptance of motherhood among women with disabilities. Second, society questions the quality of motherhood these women can provide and undermines parental competence. Finally, the Polish government provides insufficient supports.
From the perspective of women with disabilities, the greatest difficulties they face in fulfiling a mother’s role are social mechanisms that undermine their motherhood. Mothers with disabilities are particularly vulnerable to stigma and social exclusion, as the public does not perceive them fully as women. They are often seen as asexual, and the reaction of society to news that a woman with disabilities is pregnant seems to support the view that motherhood is a role that should be inaccessible to these women. These beliefs affect both the self-esteem of women and their decisions regarding motherhood. Although women with disabilities have a right to be a wife and mother, all of their reproductive rights are still considered a taboo subject.
I was at a rehabilitation camp where I met with a reception close to pathology. One guy even asked me if I knew who the father was. As if his imagination could not accommodate that someone impregnated the disabled. The whole camp gossiped about it and debated the legitimacy of my choices.
We are having a walk with my son and people ask, “Where is your mother? Ah, this is your mother.” They see me with a child but subconsciously think that it cannot be my child.
The taboo regarding sexuality is strongly related to the type of disability; the assumption of asexuality mostly affects women with visible physical disabilities. This seems to be related to the act of visualizing a relationship between a man and a woman. Visualization, according to the responses of interviewees, refers to a need for a visual stimulus, anchoring attention on the woman. This definition supports the notion of female physical identity and at the same time indicates an excess of sexual meanings that culture assigns to the body and transfers to women. As a result, womanhood itself is placed in the physical sphere (Kaschak, 2001). Corporeality has a significant impact on the self-perception of women with disabilities, and interviewees often identified physical loss with the loss of femininity. The result of this visual approach to women is a “third sex” phenomenon. Some interviewees identified a category that places women with disabilities at a low status in the social hierarchy, depriving them of gender. The analysis revealed that women with disabilities are treated as second-class citizens in terms of their femininity—as women they are like invisible beings (Wołowicz-Ruszkowska, 2013). The interviews with mothers with disabilities clearly showed that disability is a social concept that largely depends on variable thresholds of tolerance and approval.
Lack of acceptance of motherhood for women with disabilities
The right to decide to have a child is challenged by two lines of argument. The first relates to the negative impact of pregnancy on the health and lives of all women. The second applies to the negative impact of mother-to-child inheritance of disability or disorder and on the child’s educational development. Women with disabilities often face allegations that they get pregnant for selfish motives and that they destroy children’s lives and deprive them of a chance for a “normal” life. These two messages threaten the motherhood of women with disabilities. Their source is found in the local discourse of fear and ignorance (Walsh-Gallagher et al., 2012).
People think that this [is] extreme selfishness that [a] new human being is sentenced to life with a mother with disabilities. Believe me, I really try to see to it that my beautiful and wise son serves as resource to the world, rather than nursing services to his mother.
The discourse of fear and risk appears in statements of women with disabilities. It is a distinct feature of their reproductive journey, created by a social message. It manifests through social evaluations indicating beliefs that such women are incompetent, irresponsible, and incapable of motherhood. Maternal hostility to pregnancy plans grows along with intolerance and social distance—underestimating, ignoring, rejecting and, ultimately, removing the right to be a mother.
Interviewees explicitly questioned this view, which creates a vicious circle of suffering. They discussed the experience of disability in terms of the severity of restrictions. But they also described the positive effects their disability had on the child, the developmental benefits of having a mother with disabilities. This is in line with the concept of developmental gains and losses (strengths perspective; Evans & de Souza, 2008). For example, one of the benefits a child can obtain from the mother’s disability status is a great amount of time and attention.
I suspect that if I weren’t disabled, I wouldn’t have had so much time for my child.
Undoubtedly, having a child is often a source of satisfaction, strength, and self-esteem for women with disabilities.
Son gives me the strength and motivation to stand it all and try to do at least half a step forward in rehabilitation.
Women repeatedly stressed that their children are equipped with the resources and skills they could not have developed without receiving a specific type of reinforcement, namely, by overcoming the limitations of a parent with disabilities. The women contradicted the common vision of their children’s life as being of a reduced quality. They modified such beliefs by emphasising their children’s experience of greater independence and self-reliance, more developed social and emotional competences, willingness to take on challenges, and coping with difficult situations and responsibilities.
Questioning the quality of motherhood and undermining parental competence
The participants also emphasised their need to make a huge effort to prove their ability to care for their children. The interviews provide numerous examples of the fact that mothers with disabilities are subjected to public scrutiny, criticism, and stigmatism to a much greater extent than mothers without disabilities.
Since I am a mother, I see that I am subject to judgments. That people want to see whether [I can] cope in this role. To the world, my disability is an insufficiency.
The analysis of the interviews shows that being a mother with a disability requires incomparably greater commitment and determination than being a mother without a disability and that the social sanctions associated with improper execution or omission of maternal duties by women with disabilities are incomparably greater than the sanctions of mothers who do not have a disability.
After the birth I had a temporary health setback. The hospital personnel looked at me with interest and finally reported this fact to the social welfare. Someone decided that love was not enough. The decision to take away my child was made by the soldiers of the system, which does not envisage a family for the impaired. How can you take a child away from the mother who is crying because they are taking the baby away from her? I understand the drunk, but the disabled?
The interviewees also mentioned that in the current discourse on motherhood there is not enough space for mothers who are defined as “imperfect.” It probably results from the Polish “ideal of motherhood,” in which a woman alone is fully responsible for the child and is required to provide children with the “perfect” upbringing (Hryciuk & Korolczuk, 2012). The participants of the study pointed out that their disability prevents them from fulfiling the modern model of intensive mothering. This model assumes the mother’s constant presence and her exclusive care for a child. What is more, this view is based on the assumption—although usually not expressed explicitly—that children are born and are raised only in relatively affluent nuclear families where the mother can count on the support of her partner. Like the majority of women who give birth to their first child, women with disabilities experience difficulties after birth and need to master many new skills. But they must do so in the difficult context of reduced physical ability. Their inability to independently perform a full range of physical tasks related to parenthood and their lack of parental competence are common themes of the social perception of women with disabilities. The interviewees repeatedly stressed that mothers who are not able to look after their children independently are often seen as incapable of performing the role of a parent. In a society where the view of femininity is primarily based on women’s caring functions, the lack of capacity to conform with this model deconstructs the motherhood of women with disabilities, pushing them to function beyond the categories of socially acceptable femininity.
An additional concern that arose from analysis of the interviews was the societal belief that a woman who needs support is not able to fulfil the maternal role (Parish et al., 2008). However, as shown in the current study, women with disabilities are people who simultaneously receive and provide support. The interviewees often emphasised the problem of receiving improper assistance and of then being labeled an incompetent “disabled mother.” The women often mentioned attempts of health professionals and relatives to take control of a mother and her child, which might—in the opinion of the interviewees—have led to difficulties in shaping the identity of a mother.
When I was breast-feeding there was always someone accompanying me. They were giving me instructions, asking me if I can manage. I quickly started to feed my daughter with a bottle because I could do this on my own.
My husband, because he took over the majority of caring responsibilities, also took on the decision-making process regarding our child, which is usually done by the mother. Sometimes I feel excluded from making important decisions concerning our child.
The aforementioned practices add to the perception that people with disabilities must be dependent on the knowledge and the help of experts. In society, there is also a strong pattern of normalizing executive maternity (Titkow, 2012), ordering the woman to take over the exclusive rights in the material and emotional support of their children. This situation negatively affects mothers who are not able to meet these criteria because of financial or organisational difficulties or who experience physical limits to their performance (Malacrida, 2007).
Support instead of care
Women with disabilities yearned for tailored support that would facilitate their parenting but denounced attempts to take it over.
Only recently did I realize that when I ask somebody to get involved in lifelong help, I must adjust myself to a specific type of support… It is a constant balancing act between the sense of freedom and domination.
The interviewees expressed the need for support that would enhance their role as mothers, but would not remove their authority, and would leave them alone to make final decisions regarding their children.
A number of people look after my child; everyone wants to weigh in with some valuable advice and the disabled [person] is easily dominated. I want him to know that his mum is me.
The narratives show that there is a negative strain in the concept of care for those with disabilities, so the concept of care should be removed and replaced by a concept of support. Support opens up the possibility of a wide range of alternative sources of social support and informal community networks, grounded in moral values of altruism and friendship (Shakespeare, 2000, 2006). According to the study participants, there are fundamental differences between the concepts of support and care: support promotes self-reliance, while care, in the above sense, replaces it. Support applies to actions that are necessary and partial, facilitating everything that a disabled person can do to support her own performance. In the case of care, the caretaker assumes responsibility for the “weaker one.” While support is directed at a person, care is focused on a task. Support is primarily a partnership in which a person may choose which relationships correspond most closely to her needs; on the other hand, care is a subordinated relationship. Finally, support gives strength, courage, a sense of agency, and independence, while care is addictive and weakening.
What distinguishes my motherhood from the one of able-bodied women is the fact that every day I’m fighting for a little independence in the care situation, which is forced by my disability.
A Welfare System Inadequate to the Needs of Mothers
An inadequate and unsatisfactory welfare system forces mothers with disabilities to look for alternative sources of support. In this context, the interviewees mentioned the following: shared mothering, limiting motherhood to private spheres, a new gender contract, and children as independent and resilient.
The Polish law and welfare system do not recognize the needs of mothers with disabilities; the state treats them in the same way as mothers without a disability, not giving them any additional support in the upbringing of their children. Women often do not apply to the state for disability benefits because there have been cases where this has intensified monitoring of their mothering by public institutions or, in extreme cases, increased the danger of having their child removed from their care. The situation is doubly unfavourable. First, women are discouraged from seeking support intended to facilitate their mothering for fear of the consequences, including separation from their children. Second, the unfriendly, isolating human support system offered by the state does not meet their real needs. This creates a dilemma: They need to emphasise their disability and its implications to receive the security of health care, but doing so is in opposition to the image of a competent mother. As Thorne (1991) noted, “Thus, the predicament of these women was that the more they tried to take responsibility for their lives, the more they jeopardized the support and services they needed to succeed in raising their children” (p. 217). In the absence of a responsive state support system, the quality of life of women with disabilities and their children may depend on one person only.
Many inteviewees described the process of embedding women in a network of relationships. Often this process was evaluated by the interviewees—in the absence of a systemic solution—as supportive and serving their parental needs, sustaining their motherhood.
Love really takes care of almost everything. The rest is taken care of by my husband.
The basis for me was that the child was cared for, while I croak. Fortunately, I have a good relationship with my mother, who took it all on her. I admit that if I knew I did not have anyone who will compensate for my shortcomings in various areas, I would be safe and I would avoid pregnancy. I think that I should protect the child from the consequences of my disability. And thanks to my mother, I managed to sort things out.
Shared mothering
Parents who are unable to independently care for a child are perceived by society as incapable of performing parental roles. However, most of the mothers I interviewed at some point needed someone in their lives who would help to meet the needs of their children. Motherhood, in the narratives of women with physical and sensory disabilities, appears as a social practice in which not only parents are engaged but also other relatives and non-relatives who care for the family. All of them offer their collective strength and support, thus creating a chain of support.
We go for a walk like this: I push a stroller with my son and my mum pushes a wheelchair with me. It’s like a pageant. The two of us now share my mothering. My mothering is a collective task.
Both mother and child are dependent on others to a greater or lesser extent, which is why motherhood, for women with disabilities, appears to be both individual and collective. Contrary to the public perception, support is not a one-way delivery system. Women with disabilities often provide care not only for their own children but also for parents, partners, and other families. They both receive support and provide it.
The realistic assessment of my condition made me cut a deal with my mum, who has just left her job and is now helping us. We divided the tasks: I am responsible for most aspects of domestic life, also on behalf of mother (for example, I do the bank transfers, pay her rent), and she represents and replaces me on the outside (for example, takes children to kindergarten).
The interviewees mentioned that the daily support network can sometimes lead to difficulties stemming from the clash of contradictory models of family. As a result, motherhood among women with disabilities deconstructs the normative definition of motherhood and creates its new meaning. The women I interviewed described the process of negotiating with people and finding supporting solutions that would allow them to take an active role in the care of their child.
Once you have sat your ass in a wheelchair, everything changes. The attitude of the people around you changes. It gets even worse, because it also applies to your family who decides your fate. You have as much freedom as you can get. That is why I agreed with my mother that she would fulfil my requests when it comes to my child. I remain this relationship’s manager.
The women made clear that independence does not mean the exercise of care without help. The inability or limited ability to perform physical tasks related to parenthood has little to do with the ability to be a competent parent. The women perceived those in supportive roles as helping in the background while they built a relationship between mother and child.
Women are embedded in dependent relationships as a result of their disability and the lack of responsiveness of the support system (Asch, Rousso, & Jefferies, 2001). The perspective of women with disabilities complicates the discussion of this dependent relationship while offering insights into the complexities of negotiating the support they need to fulfil all the duties of motherhood. The feminist perspective, irrespective of the disability discussion, clearly sees the dependence of women as problematic (Ells, 2001). Morton (2000) noted that a dependent relationship may cause economic, social, psychological, physical, or sexual abuse and lead to stigmatisation and supervision. The interviewed women mentioned the discomfort of being dependent on a partner, family, institution, or the state. However, many women also said that building a support network could be a source of strength and identity and that this network was their most important resource. The lives of all people, not just people with disabilities, are characterised by interdependent actions of others (Ells, 2001). The stories of women with disabilities clearly showed that a rooted relationship can become the basis for self-development.
Independence is the ability to lead an autonomous life and make important life choices. Also when it comes to support.
You must learn to ask for support in such a delicate and intimate sphere of being a mother. I’m still learning it and it develops me as a human being in general.
Being a part of a support network helps a woman with disabilities achieve a greater degree of independence in mothering, as it opens the public sphere to her.
Limiting motherhood to private spheres
The unavailability or limited availability of the public sphere often confines mothers with disabilities to the private sphere. The interviewees pointed out that motherhood covers a wide range of activities, many of which take place outside the home. The public perception of women with physical and sensory disabilities is that obstacles in the external environment limit their participation in the lives of their children, making it difficult for them to build a relationship with their child. This belief, as well as the fear that they will not be able to provide the child with adequate interaction and activity in the outside world, actively discourage women with physical disabilities from parenthood.
When I left the house with my daughter, the thing I was afraid of most was that someone would think I was drunk and it was awful for me. I walk slowly, prop up and falter. Rolling over a buggy happened to me a few times. One time people helped me, the other time there was no one there, but somehow I pulled myself together. I was more afraid that somebody would think that the mother was drunk, and I would get into trouble because of this. And this was my huge anxiety associated with motherhood. That’s why I only in extreme and rare cases left the house with my child.
For women with disabilities, motherhood is a socially supervised role, and activities with children are limited by a lack of availabile accessible spaces. Accessibility is important for all mothers, but in the case of disability, inaccessible spaces result in social isolation for women and their children. In addition, the inaccessibility of the public sphere makes it difficult for mothers with disabilities to provide independent care for children and reinforces their dependence on others.
The social concept of disability assumes that the disadvantages of disability stem from the relationship between a person and her social and physical environment. Social environments, which are more or less inclusive, are friendly and accessible to people with different physical and psychological needs, yet they may constitute an obstacle for people with disabilities. Public space planning should consider the needs of all users. But the interviews showed that inaccessible public space discourages women with disabilities from being active and underscores their parental inadequacies.
Another thing that rules me out from spending time actively with my son is architecture. That’s why I prefer to sit at home. When I go out, I feel more disabled. The entire space of playgrounds screams at me “get out of here!” because it exposes what I cannot do with my child.
Hostile space (Burchardt, 2004) requires precise planning of travel routes, such as searching for sidewalks without curbs, or for places where you can relax when you walk, or where you can drive and park the car. Most of the interviewees said that due to their disability and the hostile environment, they needed to invent and learn alternative, secure, and convenient ways to care for a child. They described various unconventional practices, adapting activities, equipment, and procedures that enabled them to deal with a child, regardless of external support.
I have developed a system for putting my little thing in the baby seat and then taking him out, so I was full of joy when we could have an ordinary proper breakfast. For someone it might be a task, which they would never contemplate. For me it was something which disturbed my peace, interlaced with the anger at the manufacturer, who in all its cheapness had never thought of the fact that the seat may be used by a mother with disability.
These women found creative methods of performing daily activities and improving their mothering by using unconventional methods of moving or lifting children while maintaining the safety and comfort of the child. They also sought technical improvements, often by modifying existing equipment (cribs, car seats, high chairs), or arranging space to facilitate daily activities related to childcare. Their children also learned to adapt to the mother’s disability, for example, by helping to lift themselves, strongly holding the mother’s neck, going for a chair, or leaning against the stronger side of the mother’s body.
It is important to emphasise that, due to the complexity of their situation, not all mothers with a disability can find alternative childcare and use it without additional support. These women, after identifying their limitations in meeting the requirements of independent care, organised a support system, formed with other people (family, friends, and volunteers), that could take care of their child.
New gender contract
As described in the introduction, in Polish society the concept of the “maternal figure” imposes on the mother incomparably more responsibilities than on fathers (Hryciuk & Korolczuk, 2012). Strong idealization of the role of the mother diverts attention from understanding that care and educational roles should be determined by various factors, including one’s level of efficiency. Mothers with disabilities challenge the existing allocation of roles and diversification of parenting practices. Their experience of motherhood could become a catalyst for change. The making of a new gender contract begins in situations where the divisions of male and female realms are challenged and traditional relationships are no longer possible. Disability prevents the implementation of women’s managerial model of motherhood and fosters a redefinition of normative social roles.
For my family the situation of the deterioration of my ability was not so natural. My parents automatically took the role; they probably just never came out of the role of parents. My daughter was growing up with my disability. The person who dealt with the whole situation the worst was my husband, because it was very difficult for him to accept that I was losing my ability and that he had to take on most of the household chores—including taking care of a small child.
The results of the current study provide support for the thesis that slow change is the basic pattern of internal family life. Beliefs and cultural norms that bind people to gender-specific expectations of the duties and requirements in a relationship between a woman and a man are, from the point of view of women with disabilities, the main factors that hinder any change in the balance of power and the more favourable shaping of family relations.
There were a whole lot of fears and anxieties, because there was a husband, a tiny child—I was coping quite well then in fulfiling my role, even if it meant extreme challenges such as washing windows. The role of a woman in Poland is “a woman for everything.” My husband comes from a traditional family where he was raised only by his mother and did very little at home. He was not trained to do anything at home. When it turned out that there was a growing area where I needed help, it was very difficult for him. He did not seize anything automatically, I had to fight for some things; it was not without friction.
The Polish stereotypical division of roles in the family frees men from many household activities. What is more, it is often up to the man whether he will or will not support the woman in completing home tasks. In that sense, disability can be seen as a special circumstance that leads to the transfer of most of the household duties to the man. Her disability is important not only for establishing new patterns in a woman’s life but also for her partner’s adoption of a new role. The study participants observed a mismatch between the culture in which they were raised, in which women fulfiled all the obligations associated with childcare and the family, and a culture in which their partners took over some of these tasks. Disability—in the opinion of the women—helped them achieve the desired equality in the relationship.
Children as independent and resilient
When the mother is a person with a disability, the reorganisation of family roles often involves the the issue of children’s role as guardians of their parent. The reversal of roles occurs when a child acquires parental responsibility that surpasses the development standards recognized for the child’s age. The current study shows that the tensions associated with being dependent on their children are particularly strong among single mothers. The absence of childcare programs and social policies, combined with the lack of sensitivity in the social environment (teachers, neighbours), deepens social isolation and can lead to a reversal of roles in the mother–child relationship.
Mothers may receive support and services from health and social service groups in the voluntary and private sectors, which work with families as providers of community care or as a part of the welfare infrastructure protecting children and supporting families. However, some researchers writing from the disability perspective have argued that parental impairment is a feature of any family’s life (Ells, 2001). Parental ill health or temporary disability will always necessitate that children undertake caregiving–caretaking roles in the family, especially when parents and children are not adequately supported by other family members or professionals. Mothers with disabilities may receive care, but they also provide care to their children and to others. Both sides gain from the support of the family structure and relationships enhanced by the exchange of caregiving. Both parents and children lose when children are taken away from parents or when parents are hospitalized. The reciprocal and interdependent nature of the caring relationship enables the family to survive as a unit. In most narratives, there was a theme of children’s natural adaptation to their mother’s disability.
I do not know how much my disability changed my child’s life. She tells me, that now my disability is inside her, accepted, and loved. Composed into her life.
The women usually indicated that their children provided instrumental support, such as cleaning. Katarzyna said, “When my daughter was two she was saying, ‘I will put down this thing here so you won’t trip over it.’” Iwona said, “My child is three years old and flawlessly walks me between the cars on the street, saying: ‘Trust me, I will guide you.’” Małgorzata said, “My child at the age of five knew how to save me, for example, in a fall.” The women also received emotional support—advice, consolation, and support of parents. The interviewees acknowledged that their disability “threw” their children into adulthood, encouraged their independence and resourcefulness, and developed unexpected skills that have enabled the mother with disabilities to function in the family.
My son is amazing. His commitment to getting me out of bed, when he helps himself and me, leaning his feet on my hip, is charming.
When we go to the playground it is in fact my daughter who leads me there and not the other way round. As we are already there, I’m sitting in the sandbox until my daughter takes me by the hand and leads me to the swing, then I’m pushing her in the swing, then again she leads me to a place where she wants to be.
As the interviewees correctly assessed situations, developed realistic expectations for their child, and took into account the specific circumstances caused by their disability, they could develop mindfulness of others and prevent their child from difficulties in obtaining autonomy.
My child was growing up with my disability. My daughter always remembered that her mother has a problem, and she lived with that. It was not a problem for her. When I was bringing her up, I tried to protect those areas that I found difficult to master, I knew for example, that I would not run after my child if she ran away. My child knew, therefore, that she should not run when she was with her mum and that she had to stay close. I tried to do some forward thinking so that nothing that I could not handle would happen. My child was growing up in the situation of my disability and supported me very much. When she was little, we used to go for a walk and I was holding her hand. When we reached the bench, I would sit down and she was then more relaxed. I suspect that my disability gave a rhythm, marked certain areas and limits to my child’s freedom.
In summary, disability in the context of inadequate social services requires different social contracts, in which, despite prescribed cultural roles, relationships between family members can blossom as the mother’s role in the family is defined differently. The assumption of new roles is not an easy or peaceful task. It means that well-known models of family relationships are violated. Disability is, therefore, a factor in the disintegration of known types of social relationships; it creates the need to continuously negotiate the rules of a new order, a daily struggle for all members of the family. By continuing to build a new family structure better adapted to the prevailing circumstances, women with disabilities identify new possibilities for all families. The motherhood experiences of women with disabilities are a challenge to the deeply rooted sociocultural norms of the sexual reproduction system in relation to broad-based parenting. The experience of women with disabilities can begin the process of redefining notions of femininity and motherhood.
Disability as a Source of Self-Fullfilment
One additional theme emerged everywhere and cut across all categories. In each of the categories, the interviewees pointed out the need and possibility to overcome barriers posed by the social perception of the motherhood of women with disabilities. The interviewees often emphasised that their motherhood was a source of self-confidence, self-fulfilment, satisfaction, and happiness. Most of the women acted to overcome complications and reach their life goals. Their creative ways of looking after a child, inventive problem-solving, and persistent overcoming of barriers show that resourcefulness is a prominent feature of motherhood among women with physical disabilities. The everyday life of all mothers, regardless of their level of ability, consists of the same type of activities. And the core of motherhood—providing care—is the same for all. Motherhood, as described in the narratives of interviewees, is not defined by efficiency and physical availability. It is a relationship based on emotions and responsibility, in which the quality of relationships counts most.
Love deals with everything. Thanks to motherhood my disability does not determine my life and this is my victory.
Mothers also develop various coping strategies.
Since I became a mother I’ve became more resourceful. When my daughter was born, I asked my mum to teach me how to nurse a child on a doll. It was heartening and thanks to it I felt more certain in the new role.
Motherhood, as traditionally understood, regulates and limits women’s behaviour. These women’s narratives show that disability, by blocking the fulfilment of socially ascribed roles, may open up a broader repertoire of behaviour (Prilleltensky, 2003).
I am not able to live up to the standard of motherhood in our culture. I had no other way but to create my own. I had to come up with a new concept of me as a mother and implement this concept to the life of my family. It was a long difficult process because the ideal of the Polish Mother is deeply rooted in all of us.
Disability makes the experience of motherhood more flexible because it forces women to search for a wider context of that experience. Disability promotes the development of alternative discourses of motherhood.
General Conclusion
Practice Implications
The experiences of women with disabilities confound traditional concepts of gender and disability, and, in consequence, they demythologise and delegitimise the traditional Polish image of a mother. Since the current discourse on motherhood only concerns women who meet certain health, economic, and social conditions (Stenhouse & Letherby, 2011), there is a need to create a new model that would include women with disabilities. The responsibility for making significant changes in social support lies with the state. The system should establish guidelines concerning the type of support needed for women with disabilities, providing mothers with a sense of efficiency, accountability, and competence. Current personal assistance helps people with disabilities to perform daily living activities (e.g., eating, bathing, dressing, and toileting) and with instrumental activities of daily living (e.g., grocery shopping, cooking, and cleaning). This kind of support does not provide assistance in caring for children to women without a disability nor does it meet the needs of women with disabilities who are mothers.
For women with disabilities, motherhood can be a source of strength and personal fulfilment. However, as described in the interviews, mothers with disabilities face significant systemic barriers in wanting to create and maintain families. The mothers’ potential could be developed by raising awareness of problems that result from the combination of gender and disability. There is a need to start a dialogue on the creation of a social system in Poland that would support women with disabilities in the implementation of their maternal duties. It seems advisable to do this with the involvement of women with disabilities as advisors and partners at every level of state policy.
Today, the situation of the family might be less troublesome if the child, rather than the mother, is disabled. The child’s disability triggers the public support system. We need to expand the support system to include families where parents are persons with disabilities. The flow of information between departments should include the presence of children in the families of women (and men) with disabilities. The welfare system should provide support for children whose parents have a disability and ensure that these children benefit from the same life opportunities as all other children.
In addition, no mother with a disability should be forced to rely on any member of the family when levels of available assistance or help with tasks are inappropriate (Wates, 2002). Instead, the state should create a support system that is respectful of personal relationships and should nurture those relationships through policies, services, and procedures while maintaining care for children in a broad social context. The goal is to keep the family whole. Providing appropriate support to assist adults with disabilities in fulfiling their parental responsibilities is the best way to safeguard the welfare of children.
Study Limitations and Directions for Future Research
The analysis of the current study has a number of limitations stemming from the diversity of the group. Additional research on the experience of motherhood among women with different types of disability should also be conducted. There is also a need to examine mothers’ disabilities in different cultures and countries. That could provide insights into various strategies to support mothers with disabilities. Another valuable task would be to identify the experiences of grown-up children and to determine how this mediated disability becomes a factor that influences their biographies.
A weakness of qualitative methodology is the possible effect of the researchers’ presence on the people they are studying. Other study limitations are the status of qualitative data and the small size of the representative group, which does not allow for generalization of results. Moreover, research quality is heavily dependent on the skills of the individual researcher and more easily influenced by the researcher’s personal biases.
Conclusions
The current study examined the individual and social context in which women with physical and sensory disabilities experience motherhood. It also tried to highlight the ways in which motherhood among women with disabilities is organised and implemented, treating the disability primarily in terms of a sociocultural context. My results complement feminist research combating prejudices that hinder implementation of the right to be a mother. The narrative analysis revealed that being a mother with a disability is more of a burden than a privilege—privilege being the attribute generally associated with a maternal role. Disability can also add to the negative consequences commonly faced by women with problems such as insufficient health care or lack of support during pregnancy.
The study of motherhood among women with disabilities draws attention to the complexity and variability of mother figures. And it underscores the intensity of their entanglements in social contexts, which can lead to specific abuses (Titkow, 2012). This study demonstrates that stereotypes of disabled women include not only repressive sexuality but maternal inadequacy. For women with a disability, regardless of its type, motherhood is often treated as a “luxury.” A disabled woman who is a mother, or who may be or is about to be a mother, is treated in the social, medical, and obstetric environment with surprise, condemnation, embarrassment, and insecurity.
One important theme of the interviews is a widespread prejudice about women with disabilities functioning as mothers (Banks, 2010). The findings showed that women with disabilities are discouraged from having childen or even denied their right to have and raise a child. Women with disabilities are seen as children themselves, dependent and asexual, and are assumed to be incapable of fulfiling the traditional roles of Polish women (Nosek, Howland, Rintala, Young, & Chanpong, 2001a; Prilleltensky, 2003). It seems that pregnancy and disability are still seen as a rare combination and that the status of women as disabled overshadows their status as pregnant (Nosek, 2010). Disability situates women as people “in need of care,” ignoring them and excluding them from being people “giving care” (Morris, 1995; Prilleltensky, 2003). Women who cannot give care cannot fulfil the Polish social image of the mother.
Analysis of the interviews revealed that disability appears to offer an alternative concept of maternity, which diversifies parental practice and modifies normative social roles. Women with disabilities are forced to construct their gender identity from scratch within the experience of motherhood because they are excluded from the possibility of identifying themselves within the existing monolithic model. Thus, it appears that women with disabilities are outsiders in the system, having to renegotiate again and again their sexual identity.
This study also found that answering the question “who is mothering?” becomes increasingly difficult in light of the diversity of maternity practices. Today the family is ceasing to be monolithic; mothering becomes something that we define as we shape it ourselves, constantly (re)negotiating the terms and rules of the role. This begins to create a new model of motherhood, generated by women with disabilities.
The interviewees pointed to the complicated relationship between gender and disability, in which disability reveals itself as all-encompassing (Garland-Thomson, 2005; Lamp, 2006). The analysis of narratives of women with disabilities supplements existing feminist research on the issue of the right to be a parent. Motherhood, as experienced by women with disabilities, challenges sociocultural norms of sexual reproduction systems in the field of parenting. In the modern feminist movement, the dominant issues in the field of women’s reproductive rights are ensuring independence in making decisions regarding procreation and the social acceptance of childlessness. In light of this study, the scope of current feminist research should widen to include further study of women with disabilities, to ensure their right to motherhood.
Footnotes
Acknowledgment
The author thanks Professor Anna Titkow for inspiring comments on earlier drafts of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Academy of Special Education (Poland) under the grant: BSTM 3/13-I and was approved by the Ethics Committee of the Academy of Special Education (63-2013/2014).