
Abstract
Minority stress, which includes discrimination as well as internalized negative attitudes, is an important factor associated with maladaptive health behaviors such as binge eating among sexual minority individuals. In addition, body shame and social anxiety are robust predictors of binge eating. We examined social anxiety and body shame as sequential mediators of the association between minority stress and binge eating among young adult lesbian women. We hypothesized that social anxiety would be a key factor linking minority stress to body shame and binge eating. Self-identified lesbian women (N = 496) completed online measures of minority stress, social anxiety, body shame, and binge eating. Structural equation modeling supported the hypothesized model. Discrimination and proximal sexual minority stress were associated with increased social anxiety. In turn, social anxiety was associated with more body shame, and body shame was related to binge eating. Results suggest the oppressive social environments created by the experience of minority stress may have adverse consequences for lesbian women’s body satisfaction and eating behaviors. Interventions that bolster coping with sexual minority stress and focus on reducing social anxiety, in addition to targeting eating behavior directly, may be particularly useful for lesbian women with eating disorders or binge eating. Online slides for instructors who want to use this article for teaching are available on PWQ's website at http://pwq.sagepub.com/supplemental
Binge eating is defined as consuming a large quantity of food in a short period of time with an associated loss of control (American Psychiatric Association, 2013). Binge eating occurs across the spectrum of eating disorders as well as in women without eating disorders and is associated with negative mental and physical health (Hudson, Hiripi, Pope, & Kessler, 2007). Numerous researchers report that sexual minority women engage in more disordered eating, including binge eating, compared to heterosexual women (Austin et al., 2009; Frisell, Lichtenstein, Rahman, & Lanstrom, 2010; Hadland, Austin, Goodenow, & Calzo, 2014; Polimeni, Austin, & Kavanagh, 2009). An explanation for this disparity, consistent with minority stress theory, is that societal discrimination, stigmatization, and subsequent internalization of these attitudes are important etiological contributors to negative mental health and maladaptive health behaviors among sexual minority individuals (Hatzenbuehler, 2009; Meyer, 2003). Along these lines, in a recent empirical examination, sexual minority stress was associated with binge eating among lesbian and bisexual women (Mason & Lewis, 2015a).
An integrative framework of social anxiety among lesbian, gay, bisexual, and transgender (LGBT) youth posits that sexual minority stress may lead to social anxiety and social anxiety may lead to maladaptive behaviors among LGBT individuals (Roberts, Schwartz, & Hart, 2011). Accordingly, empirical research has shown strong relations between sexual minority stress and social anxiety (Feinstein, Goldfried, & Davila, 2012). Also, although not yet investigated among sexual minority women, social anxiety is associated with both body shame and disordered eating among heterosexuals (Dakanalis et al., 2014; Ostrovsky, Swencionis, Wylie-Rosett, & Isasi, 2013). Drawing from these theoretical and empirical findings, we developed and tested a conceptual model of contributors to binge eating among lesbian women including social anxiety and body shame as sequential mediators of the association between sexual minority stress and binge eating. We hypothesized that social anxiety would be a key variable linking sexual minority stress to body shame and binge eating.
Discrimination, Sexual Minority Stress, Body Shame, and Binge Eating
Sexual minority stress includes unique stress that sexual minority individuals experience due to their minority sexual identity. Two broad types of sexual minority stress are (a) distal sexual minority stress which includes actual experiences of discrimination, harassment, and victimization and (b) proximal sexual minority stress such as internalized homonegativity (i.e., shame regarding sexual orientation), stigma consciousness (i.e., expectations of rejection due to sexual orientation), and concealment of sexual identity (Meyer, 2003). Meyer (2003) contends that both distal and proximal sexual minority stress increase risk for a variety of negative mental health outcomes. For example, both distal and proximal sexual minority stress have been linked to depression and emotional distress (Kelleher, 2009; Lewis, Derlega, Griffin, & Krowinski, 2003; Newcomb & Mustanski, 2010), substance abuse problems (Lehavot & Simoni, 2011; Lewis, Mason, Winstead, & Kelley, 2016), and domestic violence (Balsam & Szymanski, 2005; Lewis et al., 2016).
In addition to discrimination due to sexual orientation, lesbian women may experience discrimination due to other reasons, such as being a woman or being a racial minority. This is often referred to as being a “double minority” or “triple minority” for racial minority lesbian women (Bowleg, Huang, Brooks, Black, & Burkholder, 2003). In a recent study, Black sexual minority women reported more discrimination and more forms of discrimination compared to White sexual minority women (Calabrese, Meyer, Overstreet, Haile, & Hansen, 2015). Similar to sexual orientation discrimination, gender and racial discrimination can involve overt, and sometimes violent acts, as well as more subtle acts of prejudice. Experiencing multiple forms of discrimination is related to poorer health outcomes compared to experiencing a single form of discrimination (Grollman, 2012). Consistently, both sexual orientation discrimination and gender discrimination are uniquely associated with increased psychological distress among lesbian women (Szymanski & Henrichs-Beck, 2014; Szymanski & Owens, 2009).
Sexual Minority Stress and Binge Eating
Given the paucity of research examining binge eating specifically among lesbian women, we review the literature on minority stress and disordered eating more broadly to include all sexual minority women. Mounting evidence suggests that both distal and proximal sexual minority stress are associated with increased disordered eating. Studies have demonstrated positive relations between distal sexual minority stress (e.g., heterosexist and antibisexual discrimination), proximal sexual minority stress (e.g., internalized homonegativity, stigma consciousness, and concealment), and low connectedness to the lesbian community and disordered eating among lesbian and bisexual women (Bayer, 2014; Brewster et al., 2014; Joshua, 2002; Mason & Lewis, 2015a; Watson, Grotewiel, Farrell, Marshik, & Schneider, 2015). Yet, we know little about the underlying mechanisms of these associations. Increasing our understanding of how sexual minority stress and binge eating (one particular type of disordered eating) are associated among lesbian women may offer useful suggestions for potential clinical interventions as well as advance the research literature. Body image concerns such as body shame represent a particular mechanism of interest.
Discrimination, Sexual Minority Stress, and Body Image Concerns
Sexual minority stress is related to body image concerns in sexual minority women. For instance, internalized heterosexism was positively associated with body shame among sexual minority women (Watson et al., 2015), and perceived antibisexual discrimination and internalized biphobia were positively related to body shame among bisexual women (Brewster et al., 2014). Some have suggested that the association between sexual minority stress and body shame results from sexual minority women’s motivation to pass as heterosexual and adhere to the same physical appearance norms as heterosexual women, which could reduce future discrimination or allow them to “fit in” better in society (Haines et al., 2008). Szymanski and Chung (2001) found that higher levels of proximal minority stress were associated with greater frequency of “passing for straight” in lesbian women.
Also in support of this view, among lesbian women, higher connectedness and involvement in the lesbian community were associated with lower body dissatisfaction (Heffernan, 1996; Joshua, 2002). Similarly, lesbian women who were more out to coworkers reported significantly less body surveillance, body shame, and weight concerns (Polsky, 2006). Hanley and McLaren (2014) showed that a sense of belonging––in the lesbian community, in lesbian groups and organizations, and with lesbian friends––was associated with lower body dissatisfaction. Given the strong association between body dissatisfaction and body shame (Mustapic, Marcinko, & Vargek, 2015), a lesbian-specific sense of belonging and community connectedness may protect against body shame as well. Because sexual minority stress may affect lesbian women’s decision to seek out support from the lesbian community (Puckett, Levitt, Horne, & Hayes-Skelton, 2015; Zimmerman, Darnell, Rhew, Lee, & Kaysen, 2015), lesbian women may instead try to modify or change their appearance in order to fit into the broader heterosexual society.
Body Shame as a Mediator
Body shame is an important risk factor for disordered eating (see Tiggemann, 2011, for a review). One tenet of objectification theory suggests that body shame leads to disordered eating behaviors in order to achieve a more ideal body (Fredrickson & Roberts, 1997). Among general samples of women and adolescent girls, feelings of body shame were associated with more body dissatisfaction (Mustapic et al., 2015) and with dieting (Mason & Lewis, 2015b). In addition, if the cultural body ideal is not reached, body shame may be associated with increased depressive symptoms, as has been found among heterosexual and lesbian women (Haines et al., 2008; Mason & Lewis, 2015b), which then may lead to binge eating for the purpose of affect regulation (Polivy & Herman, 1993). Consistent with objectification theory (Fredrickson & Roberts, 1997) and empirical research, there is an enduring relation between body shame and disordered eating among sexual minority women.
A number of studies have replicated the positive association between disordered eating and body shame among lesbian and bisexual women (Brewster et al., 2014; Haines et al., 2008; Kozee & Tylka, 2006; Watson et al., 2015; Yean et al., 2013). In addition, several studies have investigated body shame as a mediator between sexual minority stress and disordered eating. For example, among bisexual women, body shame mediated the relation between perceived antibisexual discrimination and eating disorder symptoms (Brewster et al., 2014). Body surveillance and body shame also mediated the relation between internalized heterosexism and disordered eating in samples of lesbian and bisexual women (Haines et al., 2008; Watson et al., 2015). Further, in a mediated model of disordered eating among lesbian women, positive sexual identity development (i.e., comfort with sexual identity, connectedness to the lesbian community, and being “out” longer) was associated with better psychological health, which in turn was associated with lower body shame, and less disordered eating (Joshua, 2002).
The studies reviewed here demonstrate that body shame may be an important mediator between minority stress and disordered eating—women who experience minority stress feel more shame about their body, which in turn leads to more disordered eating. Based on Joshua’s (2002) finding that a positive sexual identity is important in the connection between sexual minority stress and disordered eating, perhaps lesbian women experiencing minority stress become more ashamed about their body by attempting to pass as heterosexual and thus engage in more appearance monitoring and surveillance. In turn, these attempts to pass as heterosexual could lead to disordered eating in order to obtain the appearance that society presents as ideal for women. However, Watson et al. (2015) recently tested a theoretical model with lesbian women and found no relation between heterosexism and body surveillance or body shame and weak relations between internalized homonegativity and body surveillance or body shame. We hypothesized that it may be fear of negative social evaluations from others that drives the desire to pass as a heterosexual woman, and not simply experiences of discrimination and other minority stress.
Social Anxiety as a Linking Factor Between Minority Stress, Body Shame, and Disordered Eating
Social anxiety is “anxiety resulting from the prospect or presence of interpersonal evaluation in real or imagined social settings” (Schlenker & Leary, 1982, p. 642). Roberts and colleagues’ (2011) integrative framework suggests that experiences of minority stress may lead sexual minority individuals to become more anxious about evaluations from others. In support of this theoretical framework, empirical research with lesbian women and gay men has demonstrated positive relations between both discrimination and internalized homonegativity and social anxiety symptoms (Burns, Kamen, Lehman, & Beach, 2012; Cathey, Norwood, & Short, 2014; Feinstein et al., 2012). Also, internalized homonegativity mediated the relation between discrimination and social anxiety symptoms in a sample of lesbian women and gay men (Feinstein et al., 2012). Because social anxiety involves worries about how one is perceived by others, individuals who have been the target of discrimination expect to be rejected by others, and feel shame toward themselves, and they may report higher social anxiety.
One consequence of social anxiety includes elevated self-preoccupation and attention to self-presentation (Schlenker & Leary, 1982). This increased attention to oneself could lead to body image concerns if individuals are not satisfied with their appearance or if they feel others are harshly judging their appearance. Social anxiety was associated with greater body image concerns and disordered eating among presumably mostly heterosexual samples (i.e., samples in which sexual orientation was not assessed and/or reported; Cash, Thériault, & Annis, 2004; Dakanalis et al., 2014; Ostrovsky et al., 2013). People who experience social anxiety typically have difficulty developing social relationships (Alden & Taylor, 2004). As a result, social anxiety may prevent lesbian women from becoming involved in the lesbian community and from developing healthy social relationships, both of which serve as protective factors reducing body image concerns (e.g., Hanley & Mclaren, 2014). Although social anxiety, body shame, and disordered eating have not been examined collectively in a sample of lesbian women, relations between social variables and body image and disordered eating among sexual minority women have been investigated. For example, more social support and reduced social isolation were protective against disordered eating among lesbian and bisexual women (Joshua, 2002; Mason & Lewis, 2015a; Swearingen, 2006). In addition, perceived favorable social comparison and higher social rank were associated with lower body image dissatisfaction in a sample of lesbian and bisexual women (Davids & Green, 2011).
Conceptual Model
Empirical findings of relations among social anxiety, body shame, and disordered eating among heterosexuals and among other social variables, body image, and disordered eating among sexual minority women provide support for the potential association between social anxiety, body shame, and binge eating among lesbian women. We theorized that impaired social functioning (social anxiety), created by the experience of minority stress, may have adverse consequences for lesbian women’s body shame and binge eating. Our conceptual model of binge eating among lesbian women (Figure 1) is grounded in minority stress theory (Meyer, 2003) and Roberts and colleagues’ (2011) integrative model of social anxiety. We hypothesized that discrimination would be directly associated with proximal sexual minority stress and social anxiety, and proximal sexual minority stress would be directly associated with social anxiety. Also, we predicted that proximal sexual minority stress would partially mediate the relation between discrimination and social anxiety symptoms. Next, we hypothesized that social anxiety symptoms would be directly associated with body shame and binge eating and that body shame would partially mediate the relation between social anxiety symptoms and binge eating. Finally, the full model posited that minority stress would be indirectly associated with binge eating via social anxiety and body shame. In our model, we hypothesized that social anxiety and body shame would fully mediate the association between discrimination and proximal sexual minority stress and binge eating. Because body mass index (BMI) has been positively related to body dissatisfaction (Beren, Hayden, Wilfley, & Grilo, 1996; Koff, Lucas, Migliorini, & Grossmith, 2010; Strong, Williamson, Netemeyer, & Geer, 2000) and binge eating (Heffernan, 1997; Wagenbach, 2003) among lesbian women, we included BMI as a covariate of body shame and binge eating.
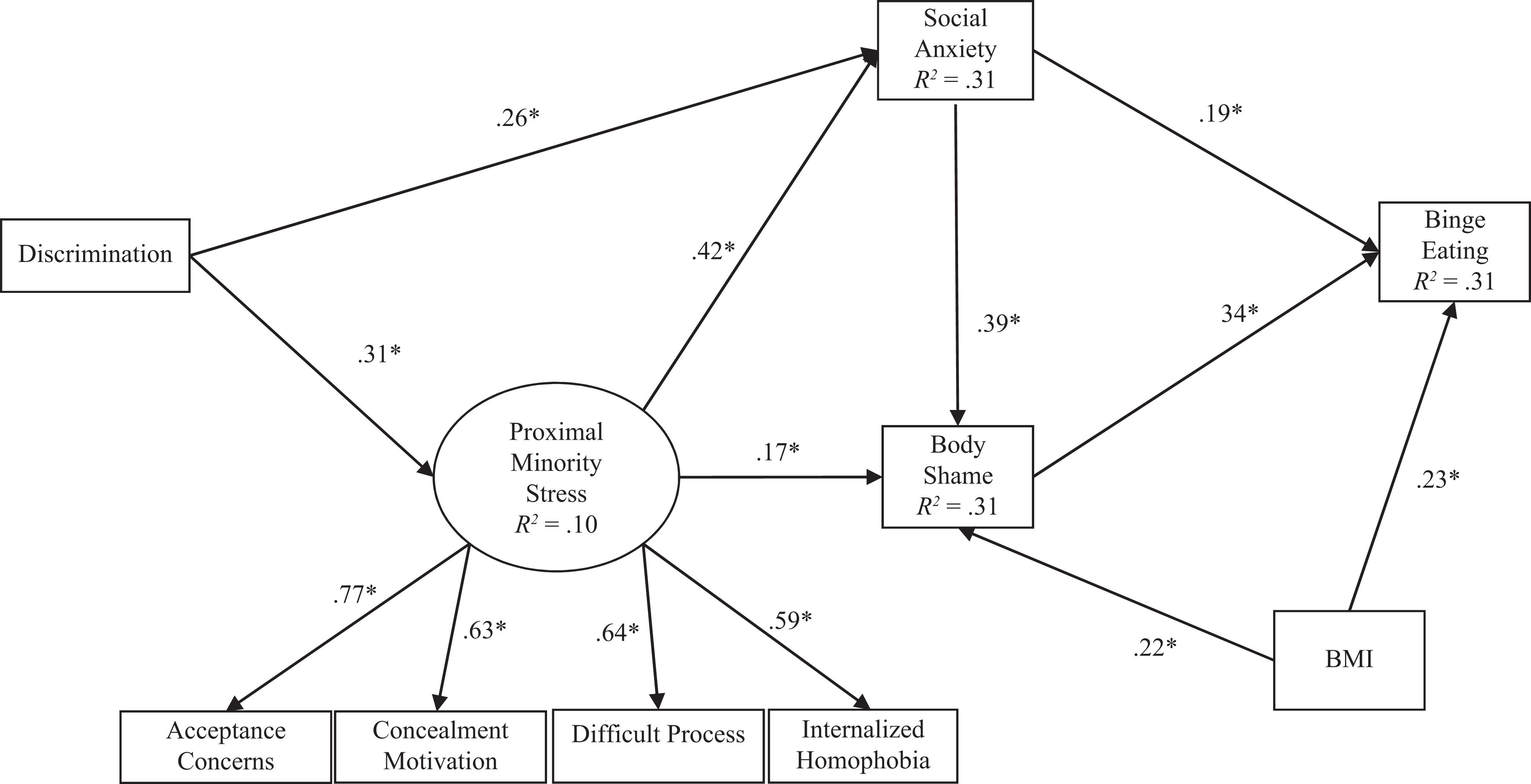
Mediated model of minority stress and binge eating among lesbians. *Bootstrapped confidence interval does not include 0. A correlated path exists between discrimination and BMI in the model but is not depicted.
Method
Participants
A sample of 496 lesbian women between the ages of 18 and 30 were recruited to participate in an online survey. Women from 49 states, the District of Columbia, and Puerto Rico participated in the study. Participation was restricted to lesbian-identified women, based on the recommendation that studying sexual minority groups separately provides important information that may be obfuscated by combining all sexual minority subgroups together (Institute of Medicine, 2011). Thus, women who indicated sexual identity other than “lesbian” were not eligible to participate in the current study. Participants were recruited through purchased Facebook advertising and LGBT websites and organizations (e.g., college LGBT organizations, city LGBT centers). The Facebook advertisements were directed to 18- to 30-year-old women living in the United States who indicated being interested in women only. Recruitment letters to LGBT websites and organizations included the same criteria. The majority of participants who completed the questionnaire indicated being recruited via Facebook. After an Internet protocol (IP) address was recorded as having completed the survey, the survey could not be completed from that IP address again. The study was reviewed and approved by an institutional review board.
The racial breakdown of the sample was 77.2% White, 3.3% Black, 0.5% American Indian or Alaskan Native, 1.9% Asian, 0.2% Native Hawaiian or other Pacific Islander, 3.1% other race, and 13.8% two or more races. About 12.3% of the sample endorsed Hispanic, Latin, or Spanish ethnicity. Most participants reported some postsecondary education: some college (44.6%), associate’s degree (9.0%), bachelor’s degree (17.0%), master’s degree (11.3%), or doctoral/professional degree (2.1%). In terms of relationship status, most women were single, not dating (35.8%), and partnered or in a committed relationship (32.0%). Women were fairly open about their sexual orientation, with 85.2% of women reporting that relative to other lesbian/gay individuals, they were “out of the closet most of the time” or “completely out of the closet.” The mean age of the sample was 21.92 years (SD = 2.85). The mean BMI was 26.30 kg/m2 (SD = 7.59). Divided into weight categories using BMI (World Health Organization, 1995) and listwise deletion, 7.4% of participants were underweight (BMI ≤ 18.5), 46.8% were normal weight (18.5 ≤ BMI ≤ 24.9), 20.8% were overweight (25 ≤ BMI ≤ 29.9), and 25.0% were obese (BMI ≥ 30).
Measures
Demographic survey
Participants completed a demographic questionnaire assessing sexual orientation, age, race, height, weight, income, state of residence, previous eating disorders, and educational level. We assessed level of outness (i.e., disclosure of sexual orientation). We calculated BMI using self-reported height and weight.
Everyday Discrimination Scale (EDS)
The EDS measures nine types of discrimination on a day-to-day basis including “people acted as if they are better than you,” “people acted as if they think you are not smart,” “people acted as if they are afraid of you,” “treated with less courtesy than other people,” “treated with less respect than others,” “received poorer service than other people at restaurants or stores,” “people acted as if they think you are dishonest,” “called names or insulted,” and “threatened or harassed” (Williams, Yu, Jackson, & Anderson, 1997). This general discrimination measure allowed us to capture in one measure, discrimination that lesbian women experience due to their sexual identity as well as gender and potentially other reasons (e.g., race and weight). Respondents indicated on a 6-point Likert scale ranging from 1 (never) to 6 (almost every day) the degree with which each discriminatory act occurred on each day. A sample item is, “I was treated with less courtesy than others.” Responses to each item were summed to create a total discrimination score. Validity of the EDS is demonstrated by positive associations with perceived stigma and externally rated prejudice events among lesbian, gay, and bisexual (LGB) adults (Frost, Lehavot, & Meyer, 2013). The EDS demonstrated adequate reliability in a sample of LGB individuals with a Cronbach’s α of .85 (Gordon & Meyer, 2008). The Cronbach’s α for the current study was .91.
Lesbian, Gay, and Bisexual Identity Scale (LGBIS)
The LGBIS is a 27-item measure that assesses eight dimensions of LGB identity (Mohr & Kendra, 2011). The current study used four of the eight subscales. We specifically chose the subscales that measured aspects of proximal sexual minority stress (other subscales measure positive aspects of lesbian identity). The Acceptance Concerns subscale measures concern and worry about others’ views of one’s sexual identity (e.g., “I often wonder whether others judge me for my sexual orientation”). The Concealment Motivation subscale assesses the desire to carefully control what others know about one’s sexual identity (e.g., “My sexual orientation is a very personal and private matter”). The Internalized Homonegativity subscale measures negative feelings or shame about one’s sexual identity (e.g., “If it were possible, I would choose to be straight”). The Difficult Process subscale assesses one’s perception of a difficult sexual identity development process (e.g., “Admitting to myself that I’m an LGB person has been a very painful process”). Participants rated each item on a Likert scale ranging from 1 (disagree strongly) to 6 (agree strongly). A validation study of the LGBIS showed that each of the subscales demonstrated adequate construct and convergent validity and reliabilities >.70 (Mohr & Kendra, 2011). The Cronbach’s αs for the current study were .80 for Acceptance Concerns, .83 for Concealment Motivation, .84 for Internalized Homonegativity, and .84 for Difficult Process.
State Social Anxiety Questionnaire
The State Social Anxiety Questionnaire is a 7-item measure that assesses social anxiety (Kashdan & Steger, 2006). Participants indicated how often they felt each social anxiety symptom over the past week on a 5-point scale ranging from 1 (very slightly/not at all) to 5 (extremely). A sample item is, “I was afraid that others did not approve of me.” Higher scores indicated more social anxiety. Kashdan and Steger (2006) reported reliability (α = .91) and concurrent validity with correlations between the State Social Anxiety Questionnaire and measures of emotion suppression, negative affect, and depressive symptoms. The Cronbach’s α for the current study was .93.
Objectified Body Consciousness Scale—Body Shame (OBCS-BS)
Due to an error in the online survey construction, participants responded to only 3 of the 8 items from the OBCS-BS Subscale (McKinley & Hyde, 1996). The 3 items from the OBCS-BS subscale to measure body shame were “When I can’t control my weight, I feel like something must be wrong with me”; “I feel ashamed of myself when I haven’t made the effort to look my best”; and “I feel like I must be a bad person when I don’t look as good as I could.” Based on previous data the authors collected on the OBCS from 540 college women of varying sexual orientations (though mostly “heterosexual”), we found that the summed score of these three correlated with the total BS subscale at r = .86. The 3-item BS summed score also correlated with binge eating (r = .46), dietary restraint (r = .46), and depressive symptoms (r = .35). Correlations between the original 8-item BS subscale and binge eating, dietary restraint, and depressive symptoms were similar to the 3-item summed score. In addition, a factor analysis of data from our sample revealed that the 3 items represented one unidimensional construct accounting for 73% of the variance. Participants used a Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree) to respond to items. The Cronbach’s α for these 3 items was .74 in a sample of over 500 college women (Mason & Lewis, 2013). The concurrent validity of the 8-item BS Subscale was demonstrated by a negative correlation with body esteem, r = −.51, and a positive correlation with body surveillance, r = .66 (McKinley & Hyde, 1996). The inter-item correlations for the 3 items in this study were all ≥.55. The Cronbach’s α for the current study was .81.
Eating Disorder Inventory—Bulimia Scale (EDIB) and Eating Disorder Diagnostic Scale (EDDS)
Based on Sherry and Hall (2009) and similar to Mason and Lewis (2015b), we constructed a binge eating measure that isolated the behavioral components of binge eating (e.g., consumption of food) from the affective components associated with binge eating (e.g., guilt), body shame, and compensatory aspects (e.g., purging). Participants responded to 5 items from the EDIB (Garner, Olmstead, & Polivy, 1983; e.g., “I stuffed myself with food”) and 7 items from the EDDS (Stice, Telch, & Rizvi, 2000; e.g., “There were times when I ate an unusually large amount of food and experienced a loss of control”). Participants responded to items from these measures using a Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). Validity of this combined scale of binge eating is evidenced by positive associations with dietary restraint, negative affect, and body shame among a large sample of college women (Mason & Lewis, 2015b). Given that the two scales were highly correlated (r = .89) and a factor analysis revealed that the items represented one unidimensional construct (accounting for 62% of variance), the items were summed to create one binge eating score with higher scores indicating more binge eating, similar to Mason and Lewis (2015b). The Cronbach’s α for the current study was .94 for the combined scale.
Procedure
We advertised the study on Facebook as a “study for lesbian women aged 18–30.” In messages to LGBT centers and websites, we included a longer message describing the survey as a study to learn more about lesbian health. Participants accessed the survey through an online link created with a survey management system and completed the questionnaires from a web-enabled device at the location and time of their own choice. No identifiable information was requested and all questionnaires were anonymous. Respondents were permitted to skip any question they did not wish to answer. The order of the items within the measures was randomized. Contact information for LGBT support and mental health resources were provided at the end of the survey. Participants were directed to a separate link to provide their e-mail address to enter a raffle for the opportunity to win either a US$50 or one of the five US$10 gift cards. Their e-mail information could not be associated with their responses in any way.
Results
Data Analysis Plan
Structural equation modeling with Mplus 7.31 was used to analyze the hypothesized model (Muthén & Muthén, 2015). With maximum likelihood estimation, we used a two-step procedure to test the hypothesized model. We first tested a measurement model to demonstrate appropriate fit of the latent variable. To appropriately identify the latent variable, at least three indicators were included and the factor loading of one of the indicators was fixed to 1. Variables were allowed to freely correlate in the model. After fitting the measurement model, we tested the structural model. In this model, we added the hypothesized directional paths. The following indices were used as guidelines in evaluating model fit: comparative fit index (CFI) ≥ .95, Tucker–Lewis index (TLI) ≥ .95, root mean square error of approximation (RMSEA) ≤ .06, and standardized root mean square residual (SRMR) ≤ .08 (Hu & Bentler, 1999). Bootstrapping with 5,000 bootstrap samples was used to test the indirect effect. The bootstrap approach generally produces preferable standard errors for the indirect effect test (Preacher & Hayes, 2008). Significance testing was done using 95% bias-corrected (BC) confidence intervals (CIs) generated from 5,000 bootstrap samples for both direct and indirect effects. If the CI did not include 0, then it was significant. BMI as a continuous score was used as a covariate of body shame and binge eating. Data are available from the corresponding author on request by e-mail.
Descriptive Statistics
The data were analyzed for missing data patterns. The analysis showed that .61% of data points were missing. Three quarters of respondents had complete data for all items (i.e., were missing no items) and 98% of the total data were complete. Because participants were often missing only several items from scales rather than missing full scales, the expectation-maximization algorithm was used to replace missing values for items (Dempster, Laird, & Rubin, 1977). Each scale was imputed separately; we used the answered items for each scale to impute items that were missing. For example, when item(s) were missing, responses to other items for the scale were used to impute the missing values. There was a high percentage of missing data for BMI (17.7%). We used full information maximum likelihood to account for missing data for BMI (see Enders & Bandalos, 2001). Descriptive statistics and bivariate correlations of study variables calculated via SPSS v. 22.0 are presented in Table 1. All study variables were significantly correlated with body shame and binge eating.
Descriptive Statistics Among Study Variables.
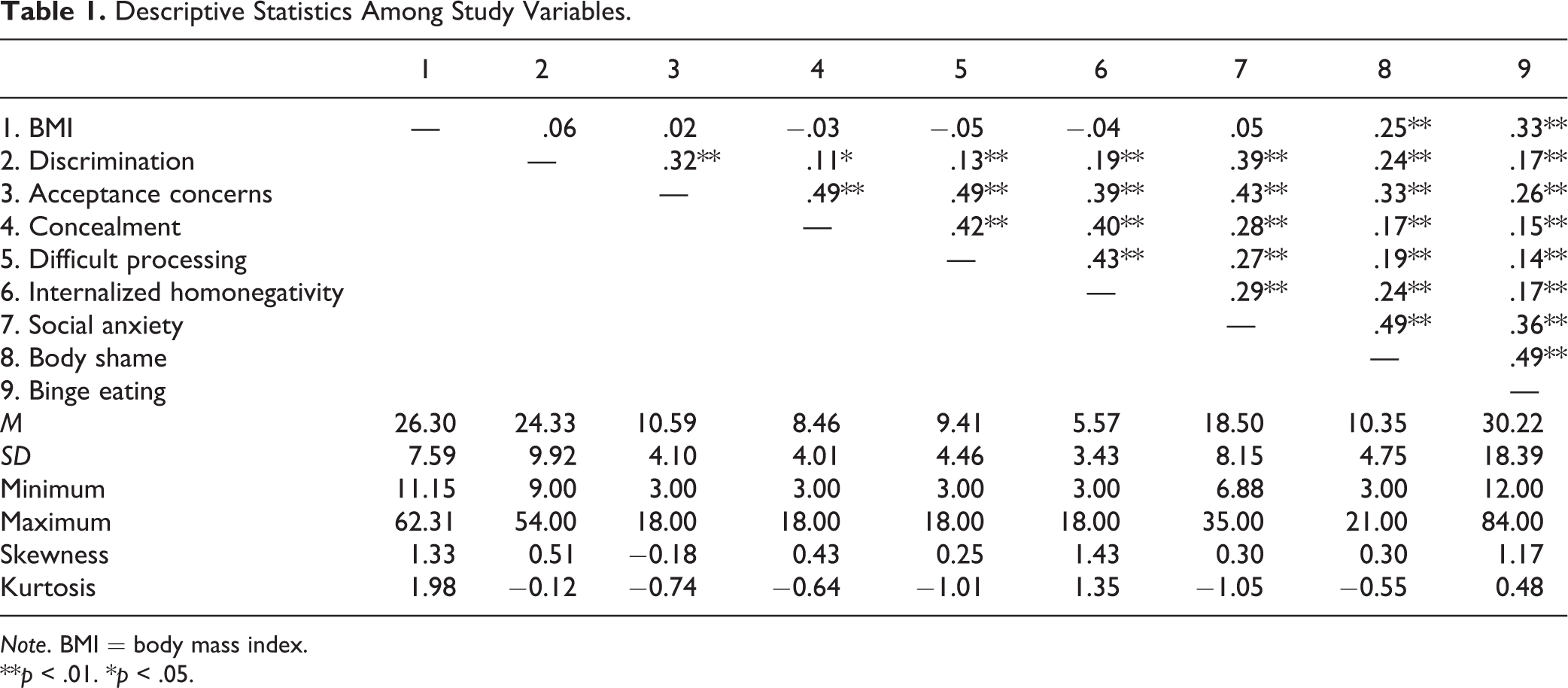
Note. BMI = body mass index.
**p < .01. *p < .05.
Main Analyses
A latent variable was created for proximal sexual minority stress comprised of acceptance concerns, concealment, difficult processing, and internalized homonegativity. All other constructs in the model were observed variables. A measurement model was calculated to define the latent factor. The model demonstrated acceptable fit, χ2(18) = 49.61, p < .001, CFI = .97, TLI = .93, RMSEA = .06, and SRMR = .03. All factor loadings were greater than .59. After fitting the measurement model, the hypothesized structural model estimated with maximum likelihood estimation demonstrated good model fit, χ2(21) = 47.35, p = .001, CFI = .97, TLI = .95, RMSEA = .05, and SRMR = .03. The model was deemed adequate, as all fit indices met the recommended stringent cutoffs (Hu & Bentler, 1999). BC CIs are presented in Table 2. The model explained 10% of the variance in proximal sexual minority stress, 31% of the variance in social anxiety, 31% of the variance in body shame, and 31% of the variance in binge eating.
Path Estimates With Bootstrapped SEs and CIs.
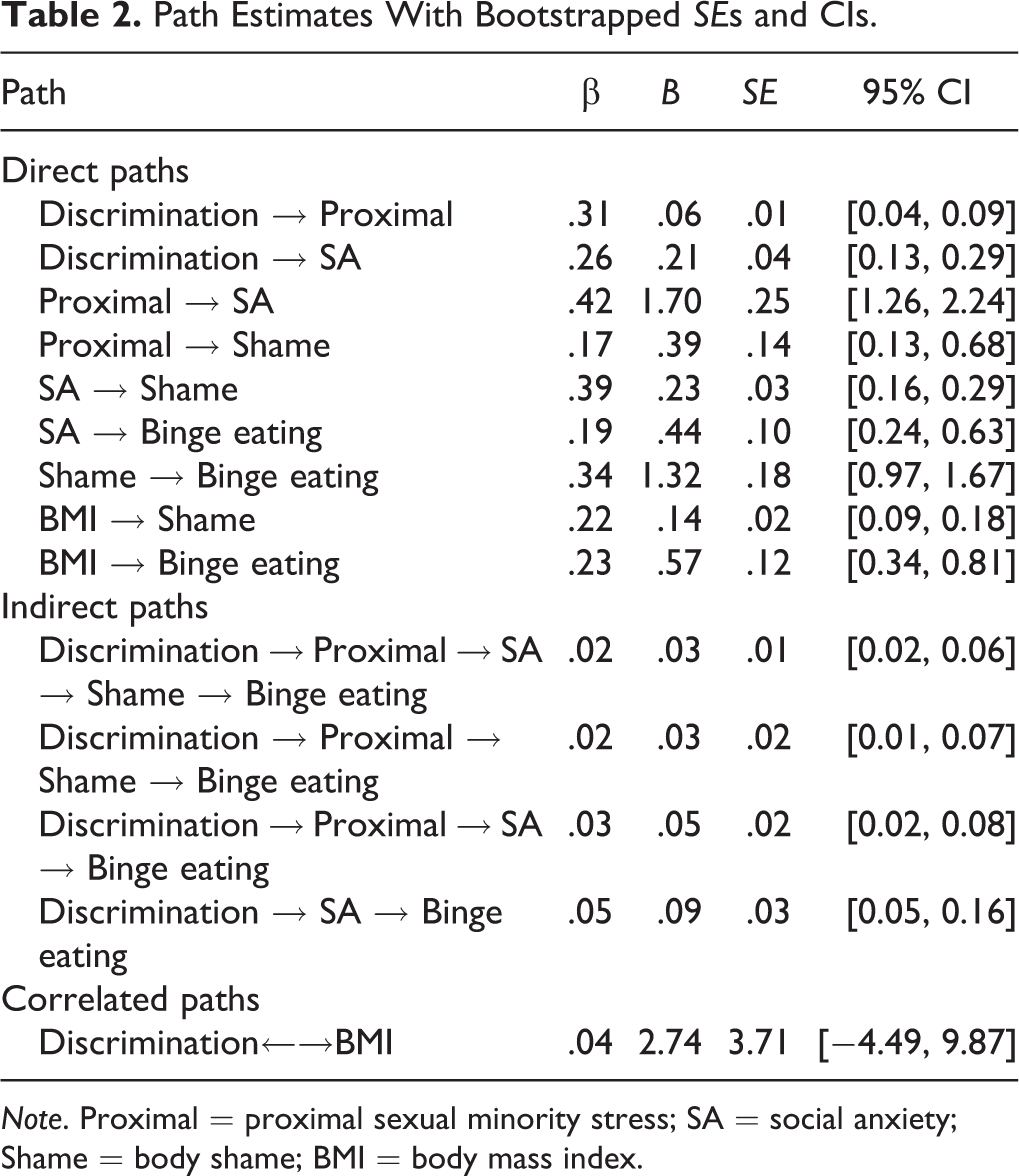
Note. Proximal = proximal sexual minority stress; SA = social anxiety; Shame = body shame; BMI = body mass index.
Experiencing discrimination was directly associated with more proximal sexual minority stress and social anxiety. Proximal sexual minority stress was positively associated with social anxiety and body shame. Social anxiety was related to increased body shame and binge eating. Body shame was positively associated with binge eating. BMI was positively related to body shame and binge eating. Tests of indirect effects revealed four pathways to binge eating (see Table 2). Discrimination was associated with binge eating via proximal sexual minority stress, social anxiety, and body shame; discrimination was associated with binge eating via proximal sexual minority stress and social anxiety; discrimination was associated with binge eating via proximal sexual minority stress and body shame; finally, discrimination was associated with binge eating via social anxiety only.
Discussion
Although prior research documents that lesbian women engage in more binge eating than heterosexual women (e.g., Austin et al., 2009), investigators have seldom examined the underlying reasons for this disparity. Based on minority stress theory, lesbian women’s experiences as members of a stigmatized and marginalized group may contribute to the disparity in binge eating (Meyer, 2003). To address this gap, we tested a model of minority stress and binge eating based on minority stress theory (Meyer, 2003) and Roberts and colleagues’ (2011) integrative framework of social anxiety. The results confirmed the main hypotheses of the study and explained a medium proportion of variance in binge eating.
Social anxiety mediated the relation between minority stress and negative outcomes (i.e., body shame and binge eating) in that lesbian women who experienced discrimination also reported more proximal sexual minority stress (i.e., internalized concerns about sexual identity such as shame and sensitivity to other’s reactions) and social anxiety. In turn, proximal sexual minority stress was associated with feelings of social anxiety and body shame. Social anxiety was related to more body shame and binge eating. Last, body shame was directly associated with binge eating. The indirect effects in the model demonstrated small effects (standardized coefficients all ≤ .05). It appears that variables in the model exert a greater effect on variables closer in the model, especially variables they directly predict. The association between social anxiety and body shame and binge eating extends the literature in two important ways. First, we extend previous research among heterosexuals on social anxiety, body shame, and binge eating (e.g., Dakanalis et al., 2014; Ostrovsky et al., 2013) to a sample of lesbian women. Second, with current results connecting social anxiety with body shame/binge eating, we offer preliminary evidence of social anxiety as an underlying mechanism of the minority stress–body shame/binge eating association among lesbian women.
In his integrative mediation framework of group-specific and general psychological processes, Hatzenbuehler (2009) predicts that experiences of discrimination are related to proximal sexual minority stress, which he termed group-specific processes, such as internalized homonegativity and expectations of rejection. In our study, experiences of general discrimination were positively related to increased proximal sexual minority stress. This finding suggests that prior experiences of discrimination may increase one’s negative feelings toward oneself as a sexual minority, difficulty accepting one’s sexual identity, or privatization of sexual identity. General experiences of discrimination were measured, as opposed to heterosexist discrimination specifically. Thus, we were able to capture the full range of discrimination, which may have included experiences related to gender or race. The association between general discrimination and proximal stress is consistent with other studies that have found positive associations between heterosexist experiences and proximal sexual minority stress (Lehavot & Simoni, 2011; Lewis et al., 2016). Because the particular reason for being discriminated against often may be unknown, lesbian women may perceive acts of discrimination as being sexual identity related, which in turn is associated with internalized sexual minority stress. In addition, discrimination in domains other than sexual identity may make women feel worse about themselves as a sexual minority even when not specifically discriminated against as a lesbian woman. For instance, sexist discrimination was positively correlated with internalized homonegativity (Szymanski, Dunn, & Ikizler, 2014).
Also, as predicted by the integrative theory of social anxiety (Roberts et al., 2011) and empirical research (Feinstein et al., 2012), we found that minority stress, both discrimination and proximal sexual minority stress, were associated with increased social anxiety. Consistent with previous research in a presumably mostly heterosexual female population (Cash et al., 2004), social anxiety was directly associated with body shame. Social anxiety may increase women’s preoccupation with their appearance in the hopes of reducing others’ negative evaluations. Levinson et al. (2013) found a strong association between social anxiety and social appearance anxiety among two samples of college students (samples were 74% and 100% women). Also, among a separate sample of college women, fear of negative evaluations was related to increased pressure to be thin and thin ideal internalization, which in turn were associated with increased body dissatisfaction (Utschig, Presnell, Madeley, & Smits, 2010). Specifically pertaining to lesbian women, preoccupation with appearance may include attempts to appear or “pass” as heterosexual, which may help lesbian women avoid negative evaluations due to their sexual identity and reduce the possibility of future discrimination. This preoccupation with appearance may lead to more attention and surveillance of their body resulting in increased body shame. In addition, increased social anxiety may prohibit lesbian women from seeking social support from the broader lesbian community. Therefore, lesbian women experiencing body dissatisfaction may not receive the protective benefits of the lesbian community (Hanley & McLaren, 2014).
We also found that proximal sexual minority stress was directly related to increased body shame, after controlling for social anxiety. Thus, the relation between minority stress and body shame cannot be attributed to social anxiety, or fear of negative evaluation, alone. Feelings of shame in one aspect of lesbian women’s lives may affect feelings of shame in other areas, possibly through reduced self-esteem. For example, women who experience minority stress and discrimination may begin to feel negatively about themselves in a global fashion with feelings of low self-worth, which may carry over to other aspects of their lives. Additionally, women high in minority stress may become more self-critical (Puckett et al., 2015). This self-criticism may be associated with a tendency to criticize and feel shame about one’s own appearance and body.
Finally, consistent with previous research on disordered eating in lesbian and bisexual women (Haines et al., 2008; Watson et al., 2015), body shame was strongly related to binge eating among lesbian women. Women experiencing body shame may engage in more dieting and restrictive behaviors which are strong risk factors for binge eating. In addition, they may experience more depressive symptoms if they are not able to reach their ideal body, which in turn may lead to binge eating. In addition, there was still a significant path between social anxiety and binge eating, after controlling for body shame. Congruent with the affect regulation model of binge eating (Polivy & Herman, 1993), it is possible that women experiencing social anxiety symptoms may engage in binge eating to cope with these negative feelings. The affect regulation explanation for binge eating has received much support. A meta-analysis of ecological momentary assessment studies showed that binge eating was commonly preceded by negative affect (Haedt-Matt & Keel, 2011).
Practice Implications
Given that binge eating symptoms are associated with a number of psychiatric disorders (Hudson et al., 2007) and poor psychosocial functioning (Wilfley, Wilson, & Agras, 2003), it is important that prevention and intervention efforts are directed toward reducing binge eating among lesbian women. Our conceptual model suggests several options for reducing binge eating among lesbian women. First, bolstering coping strategies for dealing with sexual minority stress may decrease social anxiety, body shame, and binge eating. Interventions specifically focused on coping with minority stress such as expressive writing (Lewis et al., 2005) have been described in the literature. Other, more comprehensive programs have also been described (e.g., cognitive behavioral therapy; Ross, Doctor, Dimito, Kuehl, & Armstrong, 2008).
Although not specific to sexual minority women, given social anxiety’s central role in our model, group (Gaston, Abbott, Rapee, & Neary, 2006; McEvoy, 2007; McEvoy, Nathan, Rapee, & Campbell, 2012) and individual (Lincoln et al., 2003) cognitive–behavioral therapy interventions that reduce social anxiety may be beneficial by reducing lesbian women’s body shame and associated binge eating. In addition, given research findings that social support and adaptive coping weaken the association between social anxiety and disordered eating (Wonderlich-Tierney & Vander Wal, 2010), interventions that enhance social support and bolster coping may reduce disordered eating among lesbian women.
Self-compassion is another avenue that may be useful in treating binge eating in lesbian women. Therapies including self-compassion have been effective at improving eating disorder outcomes (Kelly, Carter, & Borairi, 2014) and reducing body image concerns (Albertson, Neff, & Dill-Shackleford, 2014). While self-compassion interventions for sexual minority stress have not received much attention, a recent study found that self-compassion mediated the association between expectations of rejection and psychological distress among LGB individuals (Liao, Kashubeck-West, Weng, & Deitz, 2015). Integrating self-compassion elements in therapy may help lesbian women cope with sexual minority stress, thereby reducing psychological distress, and perhaps indirectly reducing social anxiety, body shame, and binge eating. Self-compassion therapies represent a promising area of future investigation.
Regardless of which particular intervention strategy is chosen, it is essential to increase health-care providers’ cultural competence in working with lesbian clients with disordered eating. Creating an inclusive environment in which lesbian women feel comfortable discussing issues related to their sexual identity may be vital in reducing binge eating. Moreover, it may be necessary to culturally tailor existing interventions to increase their appeal and effectiveness for lesbian clients (see Mason & Lewis, 2014). Finally, as lesbian-specific social support and community connectedness appear to be protective against body image concerns (Hanley & McLaren, 2014; Joshua, 2002), clinicians may want to incorporate these recommendations into their treatment plans.
Limitations and Future Directions
Although the findings from this study make an important contribution to the existing literature by highlighting social anxiety as an important mediational factor linking minority stress, body shame, and binge eating, we recognize the limitations of the current study. The directional predictions in our model were driven by theory, offering support for the conceptual model. However, because of the cross-sectional design, we cannot rule out the possibility that the relations between variables are in the opposite direction or may be bidirectional. Although the methodology enacted in this study was useful for exploring the relations among these variables, future studies should examine longitudinal associations between the study variables to make a stronger case for causality. Also, the indirect effects in the model had small effect sizes. Our model was evaluated among lesbian women between the ages of 18 and 30, so more research is needed to determine how our model may translate to older lesbian women. Predictors of body image concerns and disordered eating are similar for young women and middle-aged women (see Slevec & Tiggemann, 2011, for a review). However, we know little about older lesbian women and no study to date has examined body shame and binge eating specifically among older lesbian women. Future research should examine prevalence and correlates of body shame and binge eating among older lesbian women.
Our study participants were generally open about their sexual identity. It is difficult to recruit lesbian women who are less open about their identity, but greater efforts should be made to recruit these individuals. We also used a self-report measure that assessed binge eating using a number of conceptually related items. Future research should examine the relation between objective binge eating episodes and minority stress. Our measure of general discrimination limits our ability to draw conclusions about the specific effect of heterosexist discrimination. Future research should also examine the role of specific forms of discrimination (e.g., heterosexism, sexism, and racism) and binge eating individually in order to tease out the contribution of each type of discrimination. Our model of binge eating may not be generalizable to other sexual minority individuals. Thus, it is important for researchers to test this model among other sexual minority women (e.g., bisexual women) as well as sexual minority men. Another future direction is to look at how appearance anxiety specifically acts as a mediator between minority stress, body shame, and binge eating. A final limitation is that we used 3 items from the OBCS-BS subscale rather than the full 8-item subscale, which limits the reliability and validity of our measure of body shame.
Conclusion
The results of this study offer support for minority stress theory (Meyer, 2003) and Roberts and colleagues’ (2011) integrative framework of social anxiety regarding the relation of sexual minority stress and negative mental health among lesbian women. The results also extend these models by suggesting that social anxiety symptoms and stigma-related stress are positively related to body shame and binge eating. Collectively, we offer evidence that unique stress that lesbian women experience (i.e., minority stress) may be associated with binge eating through a network of mediators. As researchers and clinicians strive to reduce health disparities between lesbian and heterosexual women, it is essential to consider the role of sexual minority stress. Sexual minority stress is likely integral in explaining health disparities, including binge eating, among lesbian women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.