
Abstract

Subacromial impingement syndrome, or rotator cuff disease, is a common cause of shoulder pain. A less frequently recognized cause is coracoid or subcoracoid impingement. 1 There have been only a few reports of this condition in the literature,3–6,9,10 and although there are definitely cases that go unrecognized, coracoid impingement is probably a relatively uncommon cause of shoulder pain. Patients with this disorder usually have localized pain anteriorly, especially with forward elevation, internal rotation, and cross arm adduction. 1 Symptoms are presumed to be the result of impingement of the subscapularis tendon between the coracoid process and the lesser tuberosity. 5 Initial treatment is nonoperative and based on activity modification and physical therapy, but operative decompression may be required if conservative measures fail. The following is a case report of coracoid impingement treated by operative decompression.
Case Report
A right-handed 39-year-old male active-duty soldier came to our orthopaedic service complaining of a 4-year history of activity-related pain in his anterior left shoulder. His pain was aggravated by doing pushups and by performing activities with the arm in a forward-elevated position. He also had pain while sleeping on the affected side. Multiple courses of nonsteroidal antiinflammatory medication, activity modification, and physical therapy were unsuccessful in relieving his symptoms.
The patient was a muscular, well-developed man without any sign of muscle atrophy or deformity. He had full active range of motion of the left shoulder with the exception of decreased internal rotation compared with the right, unaffected side. The measurement difference was three vertebral spinous processes. His shoulder was tender in the region of the coracoid and just lateral to it. His motor strength measured 5/5 in all muscle groups about the shoulder, including all rotator cuff muscles. Yergason's and Speed's tests for biceps disease were negative. He had increased pain with cross arm adduction, forward elevation, and internal rotation of the shoulder. A diagnostic dose of lidocaine injected into the soft tissue between the coracoid process and the humeral head provided 100% relief of his pain, even in the provocative position of adduction, forward elevation, and internal rotation.
Roentgenograms were normal except for the presence of a very prominent, laterally projecting coracoid (Fig. 1, A and B). Magnetic resonance imaging scans (Fig. 2) revealed a 28-mm long coracoid process measured from its base at the scapula, with a coracoid index of 18 mm. 3 The coracoid index is a measurement of the lateral projection of the coracoid beyond a line tangential to the articular surface of the glenoid on an axial imaging study.
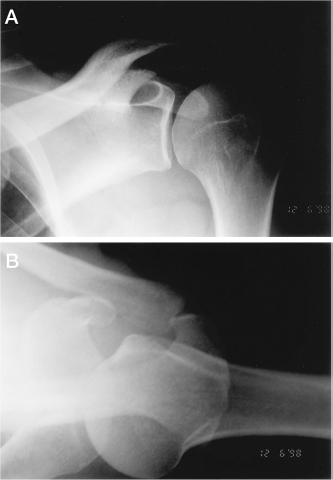
Roentgenograms revealing a prominent coracoid process. A, AP view. B, axillary lateral view.
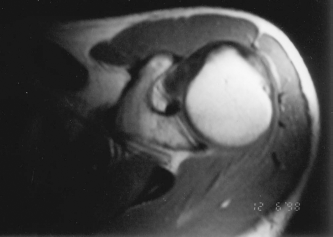
Axial MRI scan of the same shoulder seen in Figure 1. The coracoid index measures 18 mm (see text for details).
The patient underwent surgical excision of the lateral 15 mm of the coracoid process and reattachment of the conjoined tendon to the remaining coracoid base. Dines et al. 3 recommend removing 10 to 15 mm of the coracoid process. In this patient's case, 15 mm of resection was required to completely decompress the coracohumeral space with the shoulder in full internal rotation and adduction; this still left enough of the base of the coracoid process for reattachment of the conjoined tendon. During surgery it was noted that the coracoid process projected so far laterally that a standard anterior approach to the glenohumeral joint would have been impossible without either osteotomy of the coracoid or release of the conjoined tendon. Postoperative roentgenograms confirmed adequate resection of the coracoid process (Fig. 3). Six months after surgery the patient had complete relief of his pain, both during the day and at night while sleeping on the affected shoulder. His internal rotation was increased from the preoperative measurement, and he had 5/5 muscle strength about the shoulder. He had no pain with activities.

Postoperative AP roentgenogram verifies the amount of coracoid resected.
Discussion
Coracoid, subcoracoid, or coracohumeral impingement is an uncommonly recognized cause of anterior shoulder pain, but it should be considered in any patient being evaluated for impingement syndrome or anterior shoulder pain. 1 It must also be kept in mind while treating a patient for presumed bicipital tendinitis. Failure to recognize coracoid impingement may be one of the causes of a failed subacromial decompression.
The subcoracoid space is defined as the area between the coracoid process and the humeral head. 4 Coracoid impingement is characterized by impingement of the subscapularis tendon between the coracoid process and the lesser tuberosity of the humerus, resulting in tendinosis and pain in these soft tissues. The causes of coracoid impingement can be idiopathic, traumatic, or iatrogenic. 5 The syndrome is most common after a history of chronic overuse with multiple episodes of microtrauma, especially when the shoulder is overworked in a forward-elevated, adducted, internally rotated position. 10 Malunion of a coracoid process or glenoid fracture can lead to altered anatomic relationships, resulting in subcoracoid impingement. 10 Iatrogenic impingement from anterior shoulder surgery such as a Bristow or Trillat procedure or glenoid osteotomy has also been implicated. 5 These procedures produce a change in the anatomic relationships between the coracoid process and the humeral head. There has also been a case report of subcoracoid impingement caused by a ganglion arising from the subscapularis tendon. 7 Patte 9 emphasized the possibility that anterior instability of the humeral head may be causing secondary impingement.
Patients with this condition typically complain of a dull pain in the anterior aspect of the shoulder. Such pain is exacerbated by activities performed with the shoulder in a forward-flexed, internally rotated position.5,6 It is important to ask about prior shoulder surgery or trauma. Physical examination will often elicit tenderness of the soft tissues around the coracoid process and between the coracoid process and the lesser tuberosity. 10 The coracoid impingement test, which consists of placing the patient's shoulder in a position of cross arm adduction, forward elevation, and internal rotation, is a good provocative maneuver for detecting this impingement. 3 Pain is elicited more consistently in the midrange of forward elevation than in the full elevation that is used to detect subacromial impingement. 5 This test should be differentiated from the superior labrum test of O'Brien et al., 8 which requires the patient to resist downward pressure on the arm. Although the two tests are similar, the coracoid impingement test is passive on the part of the patient. The arm is placed in the provocative position without any particular effort by the patient to resist. Diagnostic lidocaine injection into the area of presumed impingement will distinguish it from subacromial impingement. 3 Roentgenograms, particularly an axillary view and an AP view perpendicular to the plane of the scapula, can detect anatomic aberrations that may be contributing to the impingement. Magnetic resonance imaging or CT scans are useful for further delineating coracoid and subcoracoid anatomy. Kinematic, or cine, MRI may be used to evaluate the dynamic aspects of subcoracoid impingement.2,4
Dines et al. 3 introduced the coracoid index, which is a measurement of the lateral projection of the coracoid process beyond a line tangential to the articular surface of the glenoid on an axial CT view. They found that the average index in 67 normal shoulders was 8.2 mm (range, −2.5 to 25 mm). The measurement of the coracohumeral interval is another way to quantify anatomic variation in this region. 4 The coracohumeral interval or distance is defined as the minimal distance between the coracoid process and lesser tuberosity, as measured on an axial MRI scan with the humerus in maximum internal rotation. Friedman et al. 4 found that in asymptomatic subjects the average coracohumeral interval measured 11 mm in maximum internal rotation, with none measuring less than 4 mm. Symptomatic patients had an average interval of 5.5 mm in maximum internal rotation; some measured 0 mm. Friedman et al. 4 also noted that there is no redundancy of the subscapularis tendon in asymptomatic subjects with the arm in full internal rotation. Patients with subcoracoid impingement often demonstrate increased soft tissue in the subcoracoid space because of redundancy or folding of the subscapularis tendon and capsular tissues when the shoulder is in this provocative position of maximum internal rotation.
The first line of treatment for coracoid impingement should be a program of activity modification, with avoidance of provocative positions, and physical therapy to strengthen the rotator cuff muscles and stabilize the scapula.5,10 Nonsteroidal antiinflammatory medications and nonnarcotic analgesics are also helpful.
Surgical decompression of the subcoracoid space may be undertaken if nonoperative measures fail. Dines et al. 3 described a coracoplasty. Earlier in their series, 3 they performed an osteotomy of the neck of the coracoid process and bent the tip medially. They found that they could not guarantee the final healed position of the tip with this method, and in their more recent patients they completed the resection of the offending portion of the tip of the coracoid and reattached the conjoined tendon to the remaining base of the coracoid. Gerber et al. 5 usually included a resection of the coracoacromial ligament and acromioplasty with the coracoid resection because of their belief that isolated coracoid impingement is rare. They performed an isolated coracoid resection in one patient who had an excellent result, but they emphasized the need to make sure that there is no element of subacromial impingement before doing this. Patte 9 recognized that some cases of coracoid impingement caused by anterior glenohumeral instability would be treated best by anterior shoulder stabilization.
Coracoid impingement should be included in the differential diagnosis when evaluating a patient with activity-related anterior shoulder pain. It is not thought to be as common as subacromial impingement, and the possibility of the coexistence of the two conditions must be taken into consideration before treatment of either as an isolated process. If nonoperative treatment fails to relieve symptoms, surgical decompression can be offered as an option.