
Abstract
Surgical management of the anterior cruciate ligament-deficient knee has evolved from primary repair to extracapsular augmentation to anterior cruciate ligament reconstruction using biologic tissue grafts. The technique of anterior cruciate ligament reconstruction has improved over the last few decades with the aid of knowledge gained from basic science and clinical research. The biology and biomechanics of anterior cruciate ligament reconstruction were analyzed in the previously published first part of this article. In this second part, current operative concepts of anterior cruciate ligament reconstruction as well as clinical correlations are discussed. The latest information regarding anterior cruciate ligament reconstruction is presented with a goal of demonstrating the correlation between the application of basic science knowledge and the improvement of clinical outcomes.
Surgical options for treatment of the ACL-deficient knee include primary repair, augmented primary repair, prosthetic replacement, and ACL reconstruction using various types of graft material. Anterior cruciate ligament-deficient knees are currently treated with reconstruction procedures that use biologic tissue grafts, as other types of surgical procedures have been performed with less success. A brief review of previously performed surgical procedures will be presented, followed by a focus on the current concepts of ACL tissue graft reconstructions. Pertinent clinical studies that review the results of various components of the operative procedure will be discussed, as well as a few key basic science principles.
ACL Surgery—Treatment Perspectives
Primary suturing of the ruptured ACL is no longer recommended as a treatment option, as both retrospective and prospective data suggest that isolated primary repairs become functionally inadequate in a high proportion of patients. 28 Although primary repair can be augmented with lateral extraarticular procedures, these procedures consist of placing a tissue weaker than the ACL in a nonanatomic position. 44 Most extraarticular procedures have failed to restore satisfactory stability to the knee.3,68 An additional means of augmenting a primarily sutured ACL is with an artificial strut. This technique uses an artificial ligament-augmentation device placed in the over-the-top position on the lateral femoral condyle to provide some additional stability. However, a recent prospective, randomized study did not find that such augmentation improved the results achieved with primary repair alone. 28
Prosthetic ligaments are not currently recommended for the reconstruction of the ACL. A recent review found that between 40% and 78% of 855 prosthetic ACL ligaments failed when assessed over a 15-year period. 24 Another report found that 83% (46) of 55 knees that had been reconstructed with a Dacron prosthesis had significant osteoarthritic changes at 9-year follow-up. 48 Synthetic grafts appear to cause more complications than biologic grafts. This may partly be the result of increased wear debris. The solution may come from tissue-engineered collagen scaffolds, enriched with growth factors. These materials may be sufficiently strong to allow the achievement of a solid fixation and early rehabilitation. Such scaffolds are not presently available, but studies are being undertaken in this area. 38
Because of the unfavorable results of primary ACL repair and of prosthetic ligament replacements, the most popular treatment of the ACL-deficient knee has become biologic tissue graft reconstruction. Current research supports the concept that a properly performed ACL reconstruction done with a biologic tissue graft improves the stability and function of the knee in most patients.
ACL Reconstruction—Graft Options
As discussed in Part I of this article (November/December 1999, pages 821–830), currently recommended graft choices for ACL reconstruction include biologic autograft and allograft materials. Autograft choices include bone-patellar tendon-bone, quadrupled semitendinosus/gracilis tendon, or bone-quadriceps tendon autografts. Allograft options include Achilles tendon, bone-patellar tendon-bone, and hamstring tendons. Although many surgeons prefer to use one particular graft choice, the modern knee surgeon must be adept at using more than one type of graft, and should choose the graft most suitable for a given patient. The biomechanical and biologic specifications of the aforementioned grafts have been discussed in Part I of this review article. It is clear that with appropriate surgical technique and rehabilitation, all of these grafts are suitable for ACL reconstruction. At present, the most commonly used grafts for ACL reconstructions are autograft bone-patellar tendon-bone and hamstring tendon grafts. Clinical studies have demonstrated that these two graft choices have similar rates of effectiveness in adults, with minor differences in postreconstruction knee stability, and muscle strength and activity levels at 2,2,47 3,31,40,63 and 5 years4,21,23 after implantation.
The bone-patellar tendon-bone graft is often selected for young, high-demand athletes because of this graft's load to failure, stiffness, quality of fixation, durability and success at long-term follow-up. This graft allows for the earliest return to high-demand activities. The advantages of the hamstring tendon graft include a smaller incision, theoretically less anterior knee pain, and a thicker tendinous portion within the knee joint and the bone tunnels. Fixation site healing of the hamstring tendon graft within the osseous tunnel is still under investigation. Also, recent studies have reported tunnel widening with the use of the hamstring tendon graft.19,47 The advantages of the quadriceps tendon autograft include a potentially wide tendinous portion along with a bone plug fixation at one end. Potential disadvantages include the size and location of the donor-site scar.
Recent literature supports the use of allograft tissue as an alternative for ACL reconstruction, 25 provided that the graft material is carefully screened for viral disease and that appropriate harvesting, sterilization, and preservation techniques that do not weaken the graft are used. Both animal and clinical data suggest that, as with autograft tissue, allograft tissue revascularizes and becomes viable after implantation.7,36,75,76 There are a few studies demonstrating that the rate of graft incorporation and remodeling are slower for allograft than for autograft reconstructions.25,36 Clinical studies with 5-year5,75,77 and 7-year 60 follow-up demonstrate that the outcomes of early ACL allograft reconstructions are similar to those of autograft reconstructions. The incidence of chronic knee effusion after allograft reconstruction appears to be diminishing, perhaps because of improved allograft procurement and avoidance of ethylene oxide sterilization.
Surgical Approaches
Over the last 25 years, there have been developments toward less-invasive techniques for the reconstruction of the ACL that are aimed at limiting extensor mechanism trauma, decreasing scarring in the knee, and avoiding exposure of the articular cartilage. Despite theoretical advantages, endoscopic and arthroscopically assisted procedures have shown minor improvement of early symptoms when compared with miniarthrotomy,15,17,67,74 and no significant difference at 2-year follow-up.29,62,72
When comparing the use of a single-incision versus a two-incision approach, clinical studies reported in the 1990s have revealed only minor short-term differences in subjective and objective outcomes.6,29,62 Potential benefits of the single-incision technique include improved cosmesis, less postoperative pain, and potentially faster rehabilitation. While there were some initial concerns regarding difficulty obtaining proper femoral tunnel placement through a single incision, this has not been a problem. When using a single-incision technique, a partial notchplasty can be performed to assist with visualization of the posterior femur. In addition, placement of the arthroscope into the anteromedial portal can assist with femoral visualization.
Tunnel Placement
Placement of the femoral and tibial tunnels aims to best restore the original anatomy, and thus limit permanent graft stretching, 9 graft impingement, 34 and overconstraint of the knee, resulting in loss of motion and graft failure. The most common technical mistake is excessively anterior placement of either the tibial or femoral tunnel. Anterior tibial tunnel placement results in graft impingement against the intercondylar roof 37 and limits knee extension. 52 Three recent studies have described a landmark for more posterior tibial tunnel placement.35,55,56 Drilling the tibial tunnel in the posterior aspect of the ACL footprint prevents graft impingement against the intercondylar roof 55 and allows satisfactory clinical outcomes. 29
On the femoral side, the femoral tunnel should be drilled near the 10 or 11 o'clock position for a right knee and the 1 or 2 o'clock position for the left knee, and immediately anterior to the over-the-top position, leaving a 1- to 2-mm posterior cortical wall. Mueller 57 has shown that an anterior femoral tunnel places the graft under high tissue strains with knee flexion, resulting in decreased knee flexion or increased graft stretching. Inversely, the over-the-top position may cause the graft to tighten in the last degrees of extension26,30,57,70 and results in an increased anteroposterior laxity when the knee is in flexion. Clinical results of over-the-top ACL reconstructions have, however, been very good with surgeons who are adept at this technique.
The tibial tunnel is initiated at or slightly anterior to the midpoint between the anterior tibial tubercle and posteromedial border of the tibia. This tunnel is directed at between a 45° to 55° angle toward the posterior aspect of the ACL tibial footprint. Care must be taken to ensure that the ACL tibial guide is perpendicular to the long axis of the tibia during drilling. Attention to this detail prevents excessively superior or inferior tunnel placement. An intraoperative lateral radiograph can be obtained to assess the quality of placement of the guide pin. With the knee in full extension, the tibial guide pin should be parallel to and lay posterior to an extension of Blumensaat's line (Fig. 1). In cases of a long bone-patellar tendon-bone graft, the angle of the tibial tunnel can be increased to prevent bone plug extrusion from the tibial tunnel.42,54,61 If the bone plug does extrude, tibial fixation can be achieved with bone staples as opposed to an interference screw.
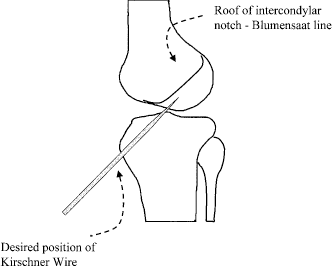
Proper positioning of the tibial guide pin for tunnel placement.
Notchplasty and Roofplasty
A notchplasty or roofplasty serves to increase the view of the posterior part of the notch and to create clearance for the graft when the knee is in extension.32,33,58 However, a large lateral notchplasty may displace the femoral insertion to an abnormally lateral position, which may lead to abnormal knee kinematics. Furthermore, a recent study has shown that aggressive intercondylar notchplasty can cause articular cartilage histopathologic changes at 6 months, consistent with those found in knees with early degenerative arthrosis. 45 A prospective, randomized study involving 100 patients found no beneficial short-term effect of performing a notchplasty (M. Cohen et al., unpublished data, 1998). Minimizing the notchplasty reduced the postoperative bleeding, pain, swelling, and potential notch regrowth (M. Cohen et al., unpublished data, 1998). Therefore, extensive notchplasty or roofplasty should be performed only if deemed necessary after having tested the graft clearance intraoperatively. Some surgeons choose to place the tibial tunnel in the central aspect of the tibial footprint of the ACL, as opposed to the posterior aspect. In these instances, a more aggressive notchplasty or roofplasty will be necessary to prevent graft impingement in extension.
Graft Preconditioning and Tensioning
The purpose of ACL reconstruction is to reestablish normal joint stability and the ability to maintain this stability with activity. While inadequate tension of the graft will result in continued instability, excessive graft tension can restrict knee motion and accelerate arthrosis within the knee. Studies have demonstrated that application of tension to the graft can influence graft performance. 26 In addition, the forces within the graft may decrease by as much as 30% soon after fixation of the graft unless the graft has been cyclically preconditioned. 27 In a prospective, randomized study of ACL reconstructions using hamstring tendon grafts with a minimum follow-up of 2 years, patients whose grafts were tensioned at 80 N had significantly less knee laxity than did those with an initial graft tension of 20 N. There were, however, no reported differences in clinical symptoms. 81 At present, the precise amount of tension that should be applied to the graft has yet to be defined.59,79
Graft Fixation
Fixation of the graft should ideally restore the original anatomy. Therefore, fixation should be as close to the joint line as possible. When using bone-patellar tendon-bone graft and a metal interference screw to reconstruct an injured ACL, a single-incision technique allows for femoral fixation at the joint line and tibial fixation distant to the joint line (Fig. 2A). A two-incision technique places the tibial bone plug at the joint line, while the femoral bone plug is fixed away from the joint line (Fig. 2B). In an effort to achieve bone-patellar tendon-bone graft fixation at both femoral and tibial joint lines, some surgeons now supplement the tibial fixation with a bone graft or bioabsorbable screw, or both, at the joint line (single-incision technique) in addition to placing an interference screw adjacent to the more distal bone plug. This will theoretically decrease tibial-sided sagittal graft tunnel motion.
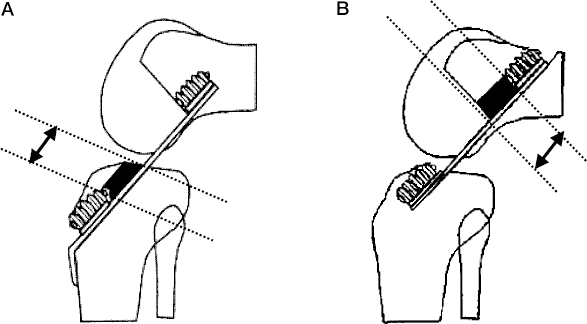
Fixation with interference screws. A, tibial fixation is away from the joint line with a single-incision technique. B, femoral fixation is away from the joint line with a two-incision technique.
Recent studies have reported no difference in the clinical outcome of reconstruction with the bone-patellar tendon-bone graft when metallic, titanium, or biodegradable interference screws are used for fixation (Ref. 50; K. P. Benedetto et al., unpublished data, 1998). On the femoral side, with the endoscopic single-incision technique, screw divergence of more than 15° from the orientation of the bone plug dramatically decreases the fixation strength of the construct.13,16,39,65 To prevent divergence, one may initiate the screw insertion by notching the anterior edge of the femoral tunnel with a small curette. Inserting the femoral screw with the knee flexed 100° to 120° better approximates the axis of the femoral tunnel. 29 Another method to prevent divergence includes inserting the screw into the notch and placing the screwdriver through the tibial tunnel.
When fixating the hamstring tendon graft, many surgeons take advantage of the recently designed bioabsorbable soft tissue screws. Use of these screws allows for graft fixation at the femoral and tibial joint lines. Whip-stitching of the quadrupled-tendon construct before its insertion into the osseous tunnels allows for easier screw placement and prevents twisting of the graft construct during screw insertion. The diameter of the screw should approximate that of the osseous tunnel to ensure adequate pullout strength. There are no long-term clinical studies on this construct, but short-term results have been good in our experience. The incidence and ramifications of cyst formation after screw absorption is unknown; however, there have been case reports, documented by MRI findings, of cyst formation after the use of bioabsorbable screws. 51
Femoral-sided hamstring tendon graft fixation can also be achieved by using a bicortical screw that crosses perpendicular to the axis of the femoral tunnel. This technique, known as cross-pin fixation, has been shown to produce good results at 2-year follow-up. 18
Hamstring tendon graft fixation can also be achieved with techniques that secure the graft near the tibial and femoral cortices. The femoral-sided Endobutton (Smith & Nephew Endoscopy, Andover, Massachusetts) and tibial-sided screw and washer have traditionally been used to achieve hamstring tendon graft fixation. This construct fixes the graft distant to the joint line and may allow for increased graft-tunnel motion. Therefore, when using this technique, it is important to assure that the quadrupled graft construct fits snugly within the osseous tunnels. It is recommended that the tunnels are underdrilled by a few millimeters and then sequential hand dilation is performed until the desired diameter is achieved. This will allow for a tighter graft-tunnel fit.
There is some debate regarding the recommended knee position at the time of tibial-sided graft fixation after femoral-sided fixation (single-incision, endoscopic technique). Although graft fixation with the knee in a small degree of flexion will result in the least amount of laxity and motion on the Lachman test, the normal knee does have some anterior-to-posterior laxity. Some surgeons fix the tibial side of the graft with the knee in full extension. This may limit the chance of developing a slight flexion contracture and will also allow for some mild anterior-to-posterior laxity. Other surgeons fix the tibial side with the knee slightly flexed, arguing that this allows for the tightest fixation. The best knee position in which to fix the graft has yet to be determined.
Donor-Site Morbidity
Bone-Patellar Tendon-Bone Autograft
The use of the central third of the patellar tendon as an autograft has been associated with donor-site symptoms. Whereas complications such as postoperative arthrofibrosis, patellar fracture, or patellar tendon rupture are rare, the incidence of patellar pain seems to be relatively high in some studies. Reports of patellar pain after harvest of this graft range from 4% to more than 40%.12,41,64,66,73 Although no study has demonstrated a definitive association, a possible reason for postharvest anterior knee pain is the development of patella baja. It has been demonstrated that, after complete closure of the tendon defect, the patellar tendon is shortened in 73% of the cases 12 by as much as 10%. 20 However, one study suggests that differences in patellar tendon length and width are identical after patellar tendon or hamstring tendon ACL reconstruction. 53 Because direct closure may lead to shortening of the patellar tendon, suturing of the patellar tendon paratenon has been proposed. Histologic data suggest that suturing the paratenon alone is sufficient to regenerate a firm tendinous scar after 6 to 12 months. 10 The properties of this scar tissue do not match the quality of the original tendon, although this scar is participating in the loadbearing of the extensor mechanism.14,45 Some surgeons leave the defect open, and MRI studies have suggested that the defect fills with hypertrophic scar, which remodels over a maximum of 2 years. 24 Some authors advocate bone grafting of the patellar bone defect. According to radiographic, MRI, and biopsy studies, bone grafting of the donor site does not show a difference in terms of histologic, clinical, or functional outcome.1,11 One study even reported a higher incidence of patellar pain due to painful bone spurring at the inferior pole of the patella after grafting. 43
An important factor for the limitation of donor-site problems in bone-patellar tendon-bone autografts seems to be the postoperative management. The incidence of donor-site problems, specifically patellar pain, has been reported to be very low in patients after an immediate and aggressive rehabilitation program after bone-patellar tendon-bone autograft harvest.69,73 Overall, it appears that the functional deficit associated with harvesting the central third of the patellar tendon is relatively low and, if present, usually resolves after 3 to 6 months. The control of patellar pain seems to depend more on the rehabilitation protocol and regaining free range of motion than on the technique of donor-site closure or bone grafting.41,73 In addition, the incidence of patellar tendon rupture is low with or without closure of the patellar tendon defect.
Hamstring Tendon Autograft
One advantage of the hamstring tendon graft is the avoidance of interference with the extensor mechanism of the knee. Despite removing two of the three medial muscular stabilizers of the knee, the functional deficit after semitendinosus and gracilis tendon harvest seems to be minimal. Three years after hamstring tendon graft ACL replacement, hamstring muscle strength is reported to be around 95% of preoperative values. 78 One study by Marder et al. 49 that compared autograft hamstring tendon and autograft bone-patellar tendon-bone patients, however, did find a statistically significant decrease in hamstring muscle peak torque at 60 deg/sec in the patients who were treated with hamstring tendon graft replacement; the subjective scores showed no statistical difference. There is no hypertrophy of the semimembranosus or biceps femoris muscle after hamstring tendon harvesting, as shown by MRI. 78 There is evidence of a postharvest firm scar formation, resembling a neotendon, in the semitendinosus and gracilis tendon region. The origin of this neotendon is slightly more proximal than on the control side. 78 In one study, soreness in the harvest area was noted for up to 3 months but was not a major patient complaint. 80 Overall, harvesting of the hamstring tendon does not cause major functional impairment for patients who have undergone ACL reconstruction.
Future Directions
Orthopaedic surgeons currently have a variety of well-established techniques and graft materials for use in replacing an injured ACL. Clinical follow-up studies with both objective and subjective evaluations have demonstrated favorable results in 80% to 90% of patients.8,22,71 However, a study with a mean follow-up of 64 months that included a comparison of bone scan and radiographic findings in ACL-reconstructed knees (91 patients) versus those in ACL-deficient knees (145 patients) found that patients who had undergone ACL reconstruction had a higher level of knee arthrosis. 21 This disturbing finding suggests that even though ACL reconstruction can prevent gross instability, there is still early degeneration in the injured knee. Long-term follow-up studies that stratify patient populations into appropriate subgroups are needed to critically evaluate current techniques in ACL reconstructions.
The field of orthopaedic surgery is currently in an exciting era with significant attention focused on the basic science of orthopaedic problems. We predict that advances in molecular biology, gene therapy, and tissue engineering in conjunction with robotic technology and computer assisted surgery may allow physicians to more successfully restore the ACL-injured knee preinjury state.