
Abstract
Osteochondritis dissecans of the patellofemoral joint is an uncommon condition that may be the cause of anterior knee pain or crepitus. We present the clinical features of 37 patients with osteochondritis dissecans lesions of the patellofemoral joint (24 on the patella, 13 on the trochlear groove), including two patients with medial trochlear groove lesions, which have not, to our knowledge, been previously reported. The osteochondral lesions involved the convex articular surfaces. The median age of patients when first examined was 15 years, and 54% of patients had open epiphyses. These lesions were more common in male patients than in female patients (four-to-one ratio). Osteochondritis dissecans of the patellofemoral joint can be overlooked unless quality radiographs are viewed with care and, at arthroscopy, both the patella and trochlear groove are assessed. Treatment depends on the symptoms, site, and nature of the lesion and the patient's age. Nonoperative management includes patellar taping and vastus medialis obliquus muscle exercises. Operative intervention is indicated for patients with mechanical symptoms and includes arthroscopy, consisting of chondroplasty and removal of loose bodies, and lateral retinacular release. In this study treatment generally improved the symptoms, but patients with articular cartilage loss had persistent patellofemoral crepitus and discomfort.
Osteochondritis dissecans is the separation of a segment of articular cartilage, and its underlying avascular subchondral bone, from the surrounding cancellous bone.2,25 This separation can be either partial or complete.
Osteochondritis dissecans was first described by Sir James Paget 18 in 1870 as “quiet necrosis” of an injured portion of cartilage and subchondral bone. The condition was named osteochondritis dissecans by Konig in 1887. 10 Konig initially believed that trauma led to articular bone surface necrosis, with the fragments gradually detaching as a result of inflammation.10,16
The cause of osteochondritis dissecans of the knee remains unknown. Axhausen (1922), 3 Ribbing (1955), 20 and Tobin (1957) 27 contributed to the early literature. Further significant contributions to the modern literature have come from Smillie,24–26 O'Donoghue, 17 Roberts, 21 and Kennedy. 9 Aichroth1,2 has made contributions related to the cause of osteochondritis dissecans, and Linden 12 to the description of the prognosis relative to epiphyseal closure. The most widely accepted theory of the cause of osteochondritis dissecans is a combination of repeated trauma and ischemia at susceptible sites on the convex articular surfaces.2,4–7,9,23,24
This condition most commonly affects the knee joint, with approximately 85% of lesions occurring in the medial femoral condyle (69% classic, 6% extended classic, and 10% inferocentral) and 15% in the lateral femoral condyle (13% inferocentral and 2% anterior).2,9 Review of the literature reveals few reported cases of osteochondritis dissecans of the lateral femoral trochlear groove.2,11 Aichroth 2 described these as anterior lesions of the lateral femoral condyle. He found these lesions in 2% of 100 patients with osteochondritis dissecans of the knee.
Osteochondritis dissecans of the patella was first reported by Rombold in 1936 22 and has been described as uncommon.9,13,23,24 There are, however, some excellent reports of these lesions, particularly by Edwards and Bentley 6 (6 cases) and Schwartz et al. 23 (31 cases).
Case Series
Between January 1981 and January 1996, the senior author (IDM) diagnosed and treated 37 cases of osteochondritis dissecans lesions of the patellofemoral joint (24 patellar lesions and 13 trochlear groove lesions). All patients had plain radiographs of the knee including AP, lateral, intercondylar, and skyline views. The lesions were best seen on the skyline patella and lateral knee views, with additional information often being gained from oblique femoral and Hughston patellar views. Most patients then underwent CT scans to define the lesions more clearly. Of the 37 patients, 30 were male (18 patellar lesions, 12 trochlear groove lesions) and 7 were female (6 patellar lesions and 1 trochlear groove lesion). This represented a male-to-female ratio of four-to-one.
Patient Age
The mean age at presentation of the patients with osteochondritis dissecans of the patella was 21.5 years (range, 12 to 33; median 15). Patients with osteochondritis dissecans of the trochlear groove had a mean age of 24.5 years (range, 13 to 40; median, 17). The majority of patients were 12 to 20 years old. At the initial examination, the epiphyses were open in 15 of 24 patients with patellar lesions and in 5 of 13 patients with trochlear groove lesions. Thus, approximately half of all patients had open physes.
Duration of Symptoms
The duration of symptoms before initial examination varied from 10 days to 15 years; most patients were seen within 6 weeks to 12 months of the onset of symptoms. In one patient, osteochondritis dissecans of the patella was an incidental finding when the patient was being examined for an ACL disruption. Another patient had bilateral trochlear groove lesions, but symptoms were present in only one knee.
The onset of symptoms was gradual in 15 patients (7 with patellar lesions and 8 with trochlear groove lesions). Repeated minor stresses related to running, cycling, kneeling, or karate occurred in 7 patients (4 with patellar lesions and 3 with trochlear groove lesions). Fifteen patients developed symptoms after a specific injury to the knee, either a direct blow or a twisting injury (13 with patellar lesions and 2 with trochlear groove lesions).
Patient Activity Level
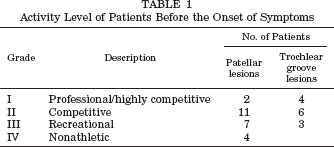
The majority of patients were competitive athletes before injury (Table 1). Six performed at grade I level (professional or highly competitive), 17 at grade II (competitive), 10 at grade III (recreational), and 4 at grade IV (played no sports).
Activity Level of Patients Before the Onset of Symptoms
Clinical Features
Symptoms
Most patients reported retropatellar pain that often radiated medially or laterally from the patella (Table 2). This pain was usually precipitated or exacerbated by running, squatting, climbing stairs, or arising from a sitting position. Catching and clicking were prominent features in those patients with unstable articular cartilage lesions. Patients with loose bodies often experienced locking.
Clinical Symptoms in Patients with Osteochondritis Dissecans of the Patellofemoral Joint
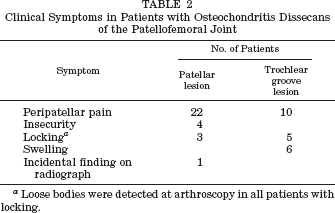
Loose bodies were detected at arthroscopy in all patients with locking.
Examination Findings
Examination revealed peripatellar tenderness and crepitus in the majority of patients. Significant functional patellar and lower limb malalignment or lateral patellar retinacular tightness were present in the majority of patients (20 of 24 with patellar lesions and 11 of 13 with trochlear groove lesions).
Imaging Investigations
Adequate radiographs, and careful examination of these radiographs, were essential. Many cases of osteochondritis dissecans were missed by the primary physician. The lesions were best identified on lateral or skyline views. Computed tomography scanning was generally undertaken to confirm and clarify the lesion, along with defining its site and size. Magnetic resonance imaging was not used in this series because the technique was not widely available in this country before 1997. Other authors have used MRI to assess bone activity, vascularity, fragment loosening, and displacement.15,19
Lesion Location
Lesions were usually craters with or without a separate fragment, but occasionally the lesion had a cystic or lytic appearance. Of the 24 patellar lesions, there were 5 inferior, 11 central (2 cystic), 6 superolateral (2 cystic), and 2 inferomedial (Fig. 1). Of the 13 trochlear groove lesions, there were 11 on the lateral femoral condyle side and 2 on the medial femoral condyle side. To our knowledge, there have been no previous reports of medial-side trochlear groove lesions. Examples of the described conditions are illustrated in Figures 2 through 4.
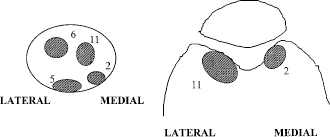
Locations of osteochonditis dissecans lesions seen in this study.
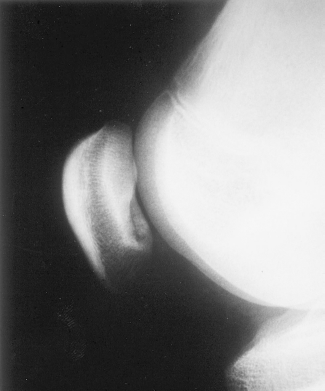
An inferior patella osteochondral crater as seen on a plain radiograph.
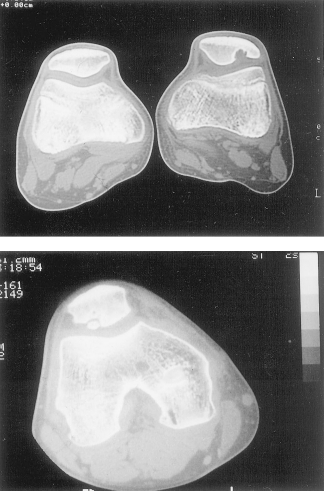
A CT scan of the knee joint showing a lateral patellar crater (top) and a crater containing an osteochondral fragment (bottom).
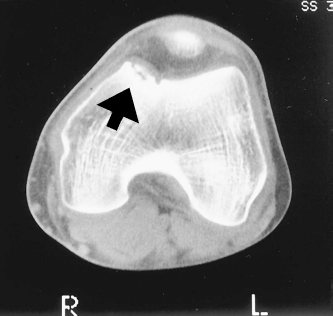
A CT scan of a medial trochlear groove osteochondral crater containing an osteochondral fragment (arrow).
Treatment
The treatment depended on the state of the epiphyses (open or closed) and the symptoms. We wanted to avoid operative intervention in patients with open epiphyses unless symptoms suggested a loose fragment.
Nonoperative treatment consisted of a modified McConnell program of lateral retinacular stretching, patellar taping, and eccentric vastus medialis obliquus muscle exercises.8,14 This program was combined with modification of activity, particularly in running, jumping, and twisting sports. Patients were encouraged to wear soft well-cushioned shoes and to convert to nonimpact or low-impact activities such as swimming and cycling. A nonoperative program was undertaken in 13 patients with patellar lesions and in 3 patients with lateral trochlear groove lesions.
Surgical treatment was indicated when there were mechanical symptoms (locking, catching, or giving way), effusion with activity, significant limitation of activity with pain, and when nonoperative management failed. Eleven of 24 patients with patellar lesions were treated surgically. Procedures performed included 10 arthroscopic chondroplasties, 4 removals of loose bodies, 1 removal of an unstable osteochondral fragment, 1 drilling procedure, and 4 lateral patellar retinacular releases. Eight of 11 patients with lateral trochlear groove lesions were treated surgically, including 6 chondroplasties, 6 removals of loose bodies, 1 removal of a loose osteochondral fragment, and 6 lateral patellar retinacular releases.
The two patients with medial trochlear groove lesions were examined arthroscopically. One was found to have a stable osteochondral fragment with an intact articular surface. This patient was treated nonoperatively and the lesion healed with no symptoms or radiographic abnormalities. The other patient required chondroplasty and removal of loose bodies.
Discussion
Thirty-seven patients with osteochondritis dissecans lesions of the patellofemoral joint were studied. This included two patients with medial trochlear groove lesions. We are not aware of previous reports of lesions in this area.
The osteochondral lesions we observed involved the convex articular surfaces and were generally seen in young active persons (median age was 16 years at initial examination). These lesions were more commonly seen in male patients than in female patients (four-to-one ratio).
The cause of osteochondritis dissecans is most likely related to “stress” to the immature convex articular surface, either as 1) repetitive microtrauma during athletic or recreational activities, 2) a single indirect trauma during a twist or jump, or 3) a direct shearing blow. These injuries may produce an undisplaced osteochondral fracture, or stress fracture, in adolescents, and these fractures may progress to nonunion and later, possibly, separation. This shearing-type stress occurs both in the longitudinal and transverse axes on the convex surfaces of the trochlear groove and patella. The lesions are more common in the lateral patellofemoral compartment, particularly in association with lateral patellar tightness and compression or functional malalignment.
Osteochondritis dissecans lesions of the patellofemoral joint can be easily overlooked unless adequate radiographs are viewed with care and, at arthroscopy, attention is paid to both the patella and femoral trochlear groove. Joint distension, and often retraction of the fat pad and synovium, is needed to adequately visualize the trochlear groove and to allow appropriate probing.
Treatment of osteochondritis dissecans lesions depends on the site and nature of the lesion and the symptoms. If there is evidence of a loose body or unstable articular surface (that is, sharp pain, crepitus, catching, effusion) then arthroscopy is recommended. Generally, the lesion can be adequately treated by arthroscopic techniques alone. If the lesions occur in the lateral facet or central ridge of the patella, or to the lateral trochlear groove, and adequate arthroscopic visualization is not obtained because of a tight lateral retinaculum, then lateral retinacular release may be indicated.
After surgery, patients begin a McConnell program of lateral retinacular stretching, patellar taping, and vastus medialis obliquus muscle exercises. The patients are encouraged to swim and cycle to reduce impact loading.
The treatments we described generally resolved the patients’ symptoms. However, some patients with articular cartilage damage had persistent patellofemoral crepitus and discomfort associated with increased athletic activities or activities involving loads on the bent knee.
In summary, the purpose of this paper was to emphasize that not all anterior knee pain is simply chondromalacia of the patella. One should be aware of the possibility of osteochondritis dissecans lesions in these patients. Careful viewing of adequate radiographs and CT scans or MRI studies can be used to make the diagnosis. When arthroscopy is indicated for any knee problem, the surgeon should carefully visualize the whole joint, including the trochlear groove and patella. With these considerations kept in mind, we may well find that these lesions are not as uncommon as previously thought.