
Abstract
Our goal was to compare the results after anterior cruciate ligament reconstruction using either the traditional one-incision or the subcutaneous two-incision technique to harvest the central third of the patellar tendon, particularly concerning disturbances in anterior knee sensitivity and the patient's ability to walk on his or her knees. One surgeon performed anterior cruciate ligament reconstruction on 124 patients with unilateral ruptures and no history of previous incisions in the anterior knee region. The traditional one-incision graft harvesting technique was used in 58 patients and the subcutaneous two-incision technique was used in 66 patients. At 2 years, the International Knee Documentation Committee classification, Lysholm score, arthrometry side-to-side difference, and single-legged hop test showed no significant differences between groups. The area of insensitivity was a median of 24 cm2 in the traditional harvest group and 0 cm2 in the subcutaneous harvest group. The patients with subcutaneous harvest had a tendency toward fewer problems during walking on their knees than did the patients with traditional harvest. Our conclusion is that the subcutaneous two-incision graft harvesting technique caused less disturbance in anterior knee sensitivity and a tendency of less discomfort during walking on one's knees than the traditional one-incision technique.
At least 50,000 arthroscopic ACL reconstructions are performed annually in the United States, 43 and around 3000 are performed annually in Sweden. 28 The results, in terms of restored knee stability and a return to sports activities, have been satisfactory after arthroscopic ACL reconstruction using patellar tendon autografts.4,5,8 However, persistent donor-site complications such as tenderness, disturbance in anterior knee sensitivity, and the inability to kneel and walk on one's knees are still a problem; 40% to 60% of the patients who have undergone either open or arthroscopic ACL reconstruction using patellar tendon autografts have some type of donor-site complication.7,16,30,32,35,36,39,41
There are several reports in the literature that support the theory that anterior knee pain after ACL reconstruction is correlated with the loss of motion.2,17,28,39,41 Shelbourne and Trumper 41 even state that the return of full hyperextension equal to the contralateral side is essential to avoid postoperative anterior knee pain.
There are few reports in the literature on discomfort after injury to the infrapatellar nerve or its branches in conjunction with ACL surgery. Slocum and Larson 42 have discussed the possibility of injury to the nerves in the anterior knee region during a pes anserinus transplantation. Berg and Mjöberg 6 have reported that difficulty in kneeling is correlated with the loss of sensitivity in the anterior knee region after open knee ligament surgery, and they therefore recommended a lateral parapatellar skin incision. In one study involving 90 patients, Kartus et al. 30 reported that the inability to kneel and walk on the knees after arthroscopic ACL reconstruction using patellar tendon autografts harvested through a 7- to 8-cm vertical incision correlated with the area of disturbed anterior knee sensitivity. This finding was subsequently confirmed by the same authors in a study involving 604 patients. 28 The same study also demonstrated a significant correlation between anterior knee problems and loss of motion.
The vertical incision used for tibial nailing is similar to that used for harvesting the central third of the patellar tendon, and Ebraheim and Mekhail 12 have mentioned the theoretical possibility of injuring the infrapatellar nerve during the insertion of an intramedullary tibial nail through the patellar tendon. Mishra et al. 34 stated in a technical note that two horizontal incisions made it possible to protect the infrapatellar nerve(s). No results in terms of nerve function were, however, presented.
Kartus et al. 26 have shown in a cadaver dissection study that it is possible to harvest the central third of the patellar tendon leaving the infrapatellar nerve undamaged in the majority of specimens. In a study involving 72 patients, Kartus et al. 27 reported that using the subcutaneous two-incision graft harvesting technique resulted in significantly more patients with no disturbance in anterior knee sensitivity than using the traditional one-incision technique. However, no significant difference was found in terms of ability to walk on one's knees.
The aim of this prospective study was to evaluate the disturbance in anterior knee sensitivity and the discomfort during walking on their knees in a large group of patients who underwent ACL reconstruction using either the traditional one-incision or the subcutaneous two-incision technique for harvesting the central third of the patellar tendon. Our hypothesis was that the subcutaneous two-incision graft harvesting technique would cause less disturbance in anterior knee sensitivity and fewer problems during walking on one's knees than the traditional one-incision technique.
Materials and Methods
Patients
A consecutive series of 124 patients was included in the study. To minimize confounding factors, only patients with unilateral ACL rupture and no history of previous incisions (except arthroscopic portals) in the anterior knee region were included. The study was approved by the Ethics Committee at Göteborg University.
Allocation Procedure
The patients were allocated to two consecutive series, depending on the graft harvesting technique that was used. The traditional graft harvesting technique was used in 58 patients (group T) and the subcutaneous technique in 66 patients (group S). In group T, the patients were operated on between November 1993 and March 1995; the patients in group S were operated on between February 1995 and October 1996. The demographics of the two study groups were comparable (Table 1).
Preoperative Demographics for Group T (Traditional Graft Harvest) and Group S (Subcutaneous Graft Harvest) a
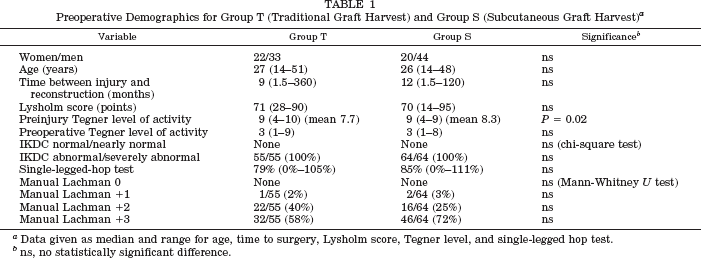
Data given as median and range for age, time to surgery, Lysholm score, Tegner level, and single-legged hop test.
ns, no statistically significant difference.
Surgical Procedure
All patients underwent ACL reconstruction by one experienced arthroscopic surgeon (J. Kartus) using the arthroscopic transtibial technique, 38 patellar tendon autograft, and interference screw fixation. 33 The femoral screw was consistently inserted through the patellar tendon defect. In group S this was done after retracting the skin incision over the tibial tubercle as much as possible in the proximal direction. All associated meniscus injuries were addressed between the time of the ACL injury and the reconstruction or at the time of the reconstruction.
Graft Harvesting Procedures
In group T, the traditional one-incision graft harvesting technique was used. This is the most common technique used by surgeons today and consists of a 70- to 80-mm vertical incision to obtain access to the central third of the patellar tendon under direct vision as described by Terry and Janssen. 47
In group S, the subcutaneous two-incision graft harvesting technique was used. This technique has previously been used by Kartus et al. 26 in a cadaver study and in a clinical situation. 27 The technique uses two vertical 25-mm skin incisions and the central third of the patellar tendon is harvested subcutaneously without dividing the paratenon.
A 25-mm vertical incision is made just above the tibial tubercle. Because the skin in this area is very mobile it is easy to identify the medial and lateral borders of the patellar tendon by retracting the skin in either direction. The paratenon is incised in the vertical direction and this incision is thereafter extended subcutaneously in the proximal direction to approximately 30 mm. A standard 20-mm long bone block is harvested from the tibial tubercle with chisels, and the bone block with the patellar tendon connected to it is pulled out through the skin incision. On each side of the proximal part of the 10-mm wide tibial bone block, a 5-mm long vertical incision through the patellar tendon is made. When the bone block is pulled out through the distal skin incision in the direction of the patella, the central part of the patellar tendon is separated from the rest of the tendon without using sharp instruments or graft harvesters. These two 5-mm incisions in the tendon are very important because they initiate the separation of the central third of the tendon from the remaining two-thirds. A second vertical skin incision is subsequently made from the apex of the patella, extending 25 mm in the proximal direction. The two folds of the prepatellar bursa and the paratenon are incised, and a sharp but closed towel clamp is pushed under the skin and the paratenon from the proximal incision and out through the distal incision. The distal bone block is captured and pulled in the proximal direction under the paratenon and out through the proximal incision. The proximal bone block is harvested using an oscillating saw and a chisel through the proximal incision in the standard manner (Fig. 1). The tendon defect is left open and no bone grafting of the defects in the tibial tubercle or the patella is performed.
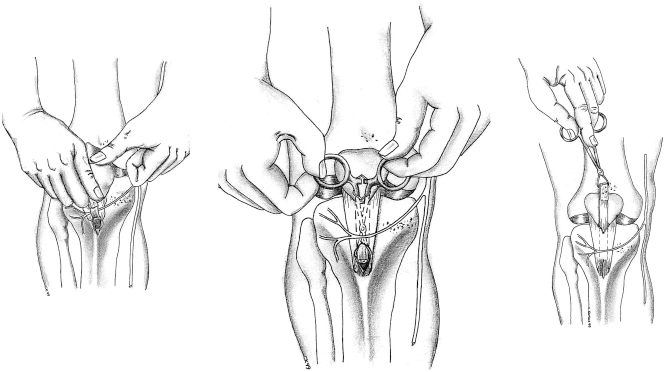
A, the bone block was pulled out through the distal skin incision in the direction of the patella, and the central part of the patellar tendon was separated from the rest of the tendon along the fibers up toward the apex of the patella, without using sharp instruments or graft harvesters. B, a sharp but closed towel clamp was pushed under the skin and the paratenon from the proximal incision. The distal bone block was captured under direct vision through the distal skin incision. C, the distal bone block was passed under the paratenon and out through the proximal incision.
Standard Clinical Assessments
The pre- and postoperative clinical assessments were performed by two independent physical therapists. The Lysholm score, 46 Tegner activity level, 46 International Knee Documentation Committee (IKDC) evaluation system, 18 single-legged hop test, 14 and manual Lachman test (graded as 0, +1, +2, +3) were used as standard clinical assessment tools. The Lysholm score was patient-administered, as described by Höher et al. 19 The total anterior-posterior laxity testing 10 was performed with a KT-1000 arthrometer (MEDmetric, San Diego, California) during only the postoperative assessment.
Specific Donor-Site and Anterior Knee Region Assessments
The anterior knee region was palpated and the area of disturbed sensitivity was measured in square centimeters (Fig. 2).
The anterior knee region was palpated and the area of disturbed sensitivity was measured in square centimeters. The dotted area shows the area of disturbed sensitivity.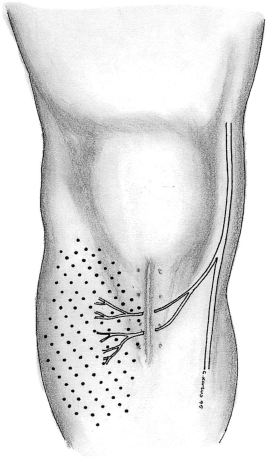
To determine donor-site discomfort, a four-grade knee-walking test was used.
30
The patients were asked to kneel on a hard floor without any clothing or protection on their knees and were then asked to walk slowly forward, on their knees, with their hands behind their back. The patients were then asked to grade the feeling of walking on the operated knee and the test as normal, unpleasant, difficult, or impossible to perform (Fig. 3).
The patients were asked to kneel on both knees on a hard floor without any clothing or protection on their knees and were then asked to walk slowly forward with their hands behind their back.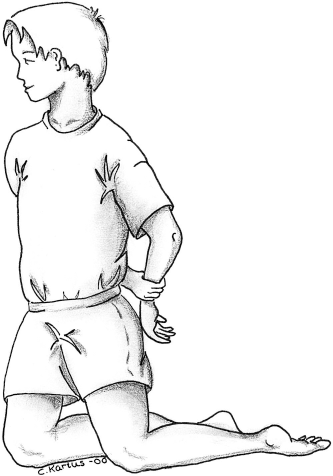
The patients were classified as having anterior knee pain (retropatellar pain) if they had all three of the following: pain while resting with the knee at more than 90° of flexion, pain while walking up and down stairs, and pain during or after activity.
Measurement of Range of Motion
The range of motion was measured with a goniometer to the nearest 5°. Any loss of motion as compared with the contralateral side was registered; for example, if full hyperextension equal to the contralateral side had not been regained, the patient was classified as having a loss of extension.
Rehabilitation
All the patients were rehabilitated according to a protocol permitting immediate full weightbearing and full range of motion. 40 No rehabilitation brace was used in the study.22,29 Closed-chain exercises were started immediately after surgery. Terminal extension with an external load was not permitted during the first 6 weeks postoperatively. Running was permitted at 3 months and contact sports at 6 months.
Statistics
Median (and range) values are presented. Wilcoxon's signed-rank test was used for comparisons of the preoperative and postoperative values of the variables in group T and group S. The Mann-Whitney U test was used to compare the variables between group T and group S. Spearman's rank-order correlation coefficient was used to test the correlations between variables. The chi-square test was used to compare categorical variables. A P value of less than 0.05 was considered statistically significant.
Results
Fifty-five of 58 (95%) patients in group T and 64 of 66 (97%) patients in group S returned for the follow-up evaluation. The follow-up period was a median of 24 months (range, 22 to 36; mean, 24.7) in group T and a median of 25 months (range, 23 to 30; mean, 25.4) in group S. Meniscus injuries were addressed between the time of ACL injury and reconstruction or at the ACL reconstruction and were registered in 39 of 55 (71%) patients in group T and in 47 of 64 (73%) in group S (no significant difference). At the ACL reconstruction, cartilage injuries were registered in 9 of 55 (16%) patients in group T and in 12 of 64 (19%) in group S (no significant difference).
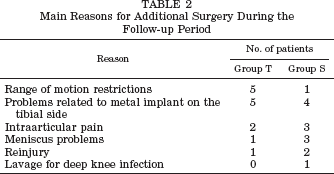
During the follow-up period, 14 of 55 (25%) patients in group T and 14 of 64 (22%) patients in group S underwent additional surgery for problems related to the metal implants on the tibial side, meniscus problems, restrictions in range of motion, or other problems (no significant difference) (Table 2). One patient in group S suffered a deep intraarticular knee infection during the 1st postoperative week. It was successfully treated with arthroscopic lavage and antibiotics. In both groups, the postoperative assessments revealed a significant improvement in terms of the Lysholm score, Tegner activity level, IKDC evaluation system, single-legged hop test, and the manual Lachman test, as compared with the preoperative values (Tables 3 and 4).
Main Reasons for Additional Surgery During the Follow-up Period
Pre- and Postoperative Assessments by the Standard Evaluation Tools in Group T a
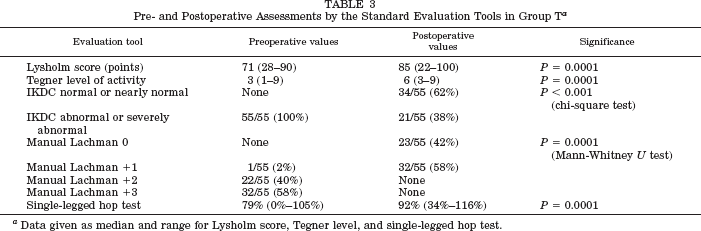
Data given as median and range for Lysholm score, Tegner level, and single-legged hop test.
Pre- and Postoperative Assessment by the Standard Evaluation Tools in Group S a
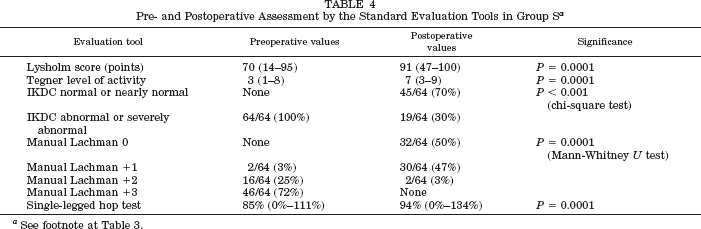
See footnote at Table 3.
The disturbance in anterior knee sensitivity was a median of 24 cm2 (range, 0 to 200) in group T and a median of 0 cm2 (range, 0 to 285) in group S (P = 0.02). Furthermore, the patients in group S had a tendency (P = 0.07) toward fewer problems during the knee-walking test than the patients in group T. A comparison between the two groups at follow-up is presented in Table 5.
Comparison of the Postoperative Values of Group S and Group T a
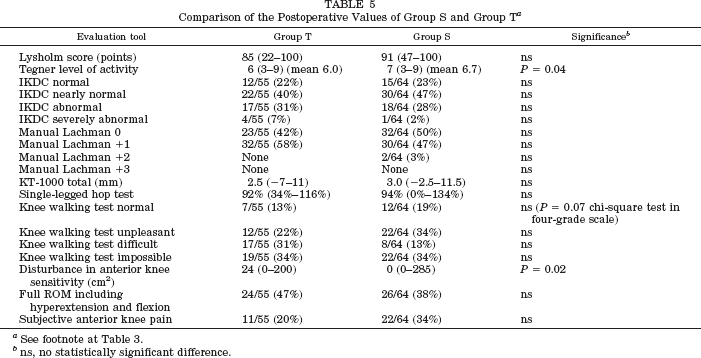
See footnote at Table 3.
ns, no statistically significant difference.
There was a significant correlation between the disturbance of anterior knee sensitivity and the discomfort on walking on their knees in group T (rho = 0.56, P = 0.0003) but not in group S (rho = 0.26, P = 0.06).
Discussion
The principal findings in the present study were that the subcutaneous two-incision graft harvesting technique produced less disturbance in anterior knee sensitivity and a tendency toward less discomfort during walking on one's knees than the traditional one-incision technique.
The strengths of the present study are that one experienced surgeon performed all the reconstructions in a standardized fashion and the only difference between the study groups was the graft-harvesting technique. Furthermore, there were few dropouts, the groups were comparable, efforts were made to minimize confounding factors, and the preoperative and postoperative evaluations were made by the same two unbiased observers.
The present study confirms and strengthens our previous observation 30 that the subcutaneous two-incision graft harvesting technique produces less disturbance in anterior knee sensitivity than the traditional one-incision technique. A technique using two horizontal incisions for patellar tendon harvest has previously been described by Mishra et al. 34 Theoretically, this technique would cause even less disturbance of anterior knee sensitivity than the technique presented in the present study. However, in our hands the horizontal incision technique caused problems during the subcutaneous tunneling procedure. This was because of the limited possibility of retracting and moving the edges of the horizontal skin incision over the proximal tibia. The use of vertical incisions solved this problem.
We must emphasize that the present study deals with only a limited part of a multifactor problem; however, we believe that the discomfort during walking on the knees, among other things, is caused by direct pressure on the injured subcutaneous nerves in the area of the skin incision. This theory could explain why the patients in group T had more discomfort during walking on their knees than the patients in group S. The theory is also supported by the fact that a traditional 70- to 80-mm vertical skin incision almost always sacrifices the infrapatellar nerve or one of its branches, as previously shown in a dissection study by Kartus et al. 26
There are several reports in the literature on injury to the infrapatellar nerve and surgery in the anterior knee region. Arthornthurasook and Gaew-Im, 3 Horner and Dellon, 20 and Hunter et al. 23 have all shown in dissection studies that the infrapatellar nerve is in danger when incisions are made close to the tibial tubercle and on the medial side of the knee joint. It is also obvious from anatomic descriptions of the prepatellar area that the infrapatellar nerve is in danger when incisions are made in the anterior knee region.1,31,48
Discomfort and paresthesia in the anterior region of the knee, along with problems kneeling, after surgery have previously been reported. Johnson et al., 25 Swanson, 44 and Tapper and Hoover 45 have described postoperative complications such as numbness and problems with kneeling after injury to the infrapatellar branch of the saphenous nerve after open medial meniscectomies. Chambers 9 explored the anterior knee area in three patients because of pain and numbness after open medial meniscectomies and found scarring or neuroma in the infrapatellar branch of the saphenous nerve. Ganzoni and Wieland 13 have shown a difference in postoperative sensory loss depending on whether the infrapatellar nerve was protected during medial knee arthrotomies. Poehling et al. 37 have described the development of reflex sympathetic dystrophy after sensory nerve injury in the knee region. The importance of the infrapatellar nerve is further stressed by the reports of Gordon 15 and Detenbeck 11 on prepatellar neuralgia after direct blows to the anterior knee region, the report by House and Ahmed 21 on entrapment of the infrapatellar nerve, and the report by Worth et al. 49 on entrapment of the saphenous nerve in the knee region. Even though there are few reports on ACL surgery and disturbance in sensitivity,6,28,30 the findings in the present study, previous findings by Kartus et al.,28,30 and reports in the literature stress the importance of protecting the infrapatellar nerve when incisions are made in the anterior knee region. One important reason is that kneeling and walking on one's knees are essential in many occupations, as well as in religious ceremonies.
There appears to be agreement in the literature that the restoration of full extension compared with the noninjured side after ACL reconstruction is essential to avoid postoperative discomfort in the anterior knee region. Irrgang and Harner, 24 Harner et al., 17 and Sachs et al. 39 have stated that the loss of extension contributes to anterior knee pain. Shelbourne and Trumper 41 have stated that the restoration of full hyperextension is of major importance when it comes to avoiding anterior knee pain.
The influence of loss of flexion on anterior knee pain is controversial. Stapleton 43 states that the loss of flexion causes significantly more anterior knee pain than the loss of extension, and Aglietti et al. 2 reported that loss of flexion exceeding 10° might be correlated with anterior knee pain. However, Irrgang and Harner 24 found that loss of flexion rarely creates difficulties, unless the knee flexion is less than 110°.
In a previous study involving 604 patients, we have shown that anterior knee problems and discomfort during the knee-walking test were correlated with the loss of motion, especially with the combined loss of both flexion and extension. 28 In the present study, there was no difference between the study groups in terms of the loss of motion and the frequency of subjective anterior knee pain. It is therefore probable that the difference in the ability to walk on the knees was caused by the graft harvesting technique and the difference in the disturbance in anterior knee sensitivity. However, it is also probable that the graft harvesting technique has no influence on the results after ACL reconstruction using central third patellar tendon autografts, as long as the knee-walking test is not taken into account. This view is supported by the fact that all the other variables, except the Tegner activity level, revealed no significant difference between the study groups.
One interesting finding was that the disturbance in sensitivity correlated significantly with the discomfort when walking on the knees in group T, but not in group S. One explanation for this difference could be that in a situation in which the majority of the patients have minimal or no disturbance in sensitivity, as seen in group S, other factors such as the loss of motion probably tend to have more effect on the results of the knee-walking test.
We were able to verify our hypothesis that the subcutaneous two-incision graft harvesting technique caused less disturbance in anterior knee sensitivity and a tendency toward fewer problems during walking on the knees than the traditional one-incision technique. Because of the findings in the present and previous studies, we have discontinued the use of the traditional one-incision technique.