
Abstract

Acquired anomalies of the upper extremities are relatively rare in young athletes and, as such, are sometimes overlooked as a cause of pain in this patient population. Nevertheless, there are specific conditions that cause arterial insufficiency in athletes. Both axillary artery thrombosis secondary to compression by the humeral head and axillary artery aneurysm formation with distal embolization have been reported as causes of arm and hand ischemia in athletes. We describe a case of symptomatic dissection of the axillary artery in a tennis player. The dissection resulted in a nearly complete occlusion of the axillary artery just distal to the origin of the circumflex humeral vessels. The anatomic location of the dissection suggests a tethering effect of the circumflex vessels, which assumes importance in athletic activities characterized by forceful abduction and forward motion of the upper extremity. Although this newly recognized condition is probably uncommon, it should be considered when evaluating tennis players who are experiencing arm pain.
Case Report
A 52-year-old, right-handed woman who was an avid tennis player was seen with a 9-month history of pain in the right arm and forearm brought on by repetitive activities. Her medical history was unremarkable. Specifically, there was no history of diabetes, hypercholesterolemia, cigarette smoking, or manifestations of atherosclerotic cardiovascular disease. Physical examination revealed barely palpable brachial and radial pulses in the right upper extremity. All other pulses were palpable and normal. There were no manifestations of cutaneous ischemia. Arterial noninvasive flow studies of the upper extremities demonstrated marked dampening of the arterial flow curves on the right extremity, and her forearm blood pressure was 70 mm Hg lower on the right than on the left side. Arteriography was performed and demonstrated near complete occlusion of the right axillary artery beginning at the origin of the circumflex humeral vessels (Fig. 1).
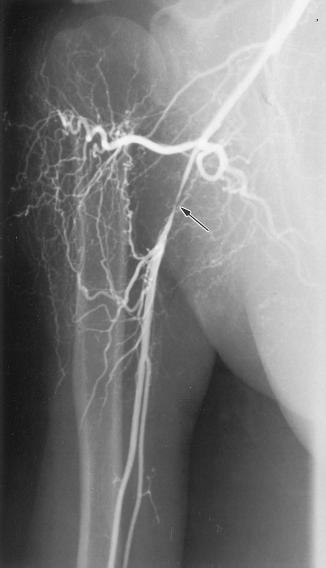
Arteriogram demonstrating near complete occlusion of the right axillary artery (arrow) beginning at the origin of the circumflex humeral vessels.
Surgical repair was performed. The right arm was positioned in 90° of abduction. An incision was begun in the right axilla and extended to the border of the pectoralis major muscle. The right axillary artery was approached by careful sharp dissection, and no neural or venous structures were divided. The axillary artery was found to be thickened over a distance of 4.0 cm and there was a chronic inflammatory reaction surrounding the artery. The vessel was completely normal both proximal and distal to the thickened, nearly occluded segment. There was no evidence of extrinsic compression of the artery by tendinous or muscular tissue. The anterior and posterior circumflex humeral arteries arose individually from the axillary artery. These vessels were involved in the dissected segment and were ligated and disconnected from the axillary artery. The diseased segment was excised and reconstruction was accomplished using a reversed vein harvested from the saphenofemoral junction. Her postoperative course was uncomplicated and there was immediate return of palpable radial and ulnar pulses in the extremity. The patient resumed all activities, including tennis, and has remained asymptomatic during 8 months of follow-up. Postoperative noninvasive flow studies revealed normal blood flow in the right upper extremity.
Discussion
Although most upper extremity pain in athletes has a musculoskeletal origin, vascular anomalies will occasionally be found and must be considered in the differential diagnosis. Reports exist of baseball pitchers with complete axillary artery occlusion due to thrombosis,4,6 with intimal tearing as a presumed cause of the arterial thrombus formation. Subclavian artery thrombosis with retrograde propagation to the brachiocephalic artery and subsequent embolic stroke has been reported in a major league baseball pitcher. 1 Digital ischemia secondary to embolization from aneurysms of the posterior circumflex humeral arteries have been reported in three volleyball players, 3 and another report described embolization to the hand in two baseball pitchers with aneurysms of the posterior circumflex humeral artery and subscapular artery, respectively. 2
Our group recently described the successful treatment of two major league baseball pitchers with digital ischemia in the pitching hand. 5 The ischemic changes were secondary to embolization from thrombus within axillary artery aneurysms that had developed at the junction of the axillary artery and the circumflex humeral arteries in their pitching arms.
It now appears clear that aneurysms of the axillary artery and its branches can occur in any athletic activity that is associated with repetitive, forceful extension of the upper extremity. The case reported here suggests that the same forces exerted on the axillary artery that lead to aneurysm formation at the junction of the axillary and circumflex humeral arteries can cause dissection of the artery at that point. Atherosclerotic occlusion of the axillary artery distal to the origin of the circumflex humeral vessels is rare. The occurrence of axillary arterial occlusion in our patient, who had no other manifestations of occlusive disease, suggests that her arterial dissection and occlusion were caused by mechanical stresses on the artery. It is likely that the mechanism of injury was repeated abduction and external rotation of the upper extremity with downward displacement of the humeral head. The circumflex humeral arteries arise from the third portion of the axillary artery, either separately or as a common trunk, encircle the surgical neck of the humerus, and provide the main arterial supply to the head of the humerus. This anatomic configuration creates a tethering effect on the axillary artery and maintains the artery in a fixed position relative to the humerus. A repetitive stretching motion at the point of fixation, such as occurs in tennis, baseball pitching, or volleyball, for example, can lead to dissection or aneurysm formation of the axillary artery. These lesions should be considered in an athletic patient with upper extremity pain.