
Abstract
Reconstruction of the anterior cruciate ligament using a hamstring tendon autograft has often been recommended for female athletes. We compared the results of acute, isolated, intraarticular anterior cruciate ligament reconstructions using quadruple-looped hamstring autografts in 39 female and 26 male patients. All reconstructions were performed by the same surgeon using a similar surgical technique and the same postoperative management. In each case, patients had Endobutton femoral fixation and either post or button fixation for the tibial side. The average follow-up was 40.9 months for women and 39.0 months for men. Objective analysis of results included examination for the presence of effusion and crepitus, Lachman and pivot shift testing, and KT-1000 arthrometer testing for side-to-side differences. Subjective analysis consisted of a 15-item visual analog scale completed by patients postoperatively, and pre- and postoperative Tegner and Lysholm scores. The clinical failure rate was 23% (9 of 39) for the female patients and 4% (1 of 26) for the male patients, which was statistically significant. There was also a trend toward increased laxity in female patients. Subjectively, the women also reported a higher frequency and intensity of pain. Based on Tegner activity levels, more of the men returned to their preinjury level of activity than did the women. When compared with the male patients, female patients had a significantly higher failure rate after reconstruction.
There has recently been a vast increase in the number of women participating in competitive and recreational sports.15,26 Along with this rise in participation, there has been an increase in the number of ACL injuries in female athletes when compared with their male counterparts.3,5,8–11,13–16,19,23,29,30,38 Although it has been suggested that women may be more cruciate-dependent than men, 6 the precise reason for their increased risk of ACL injury is unknown and probably multifactoral. 3 Some proposed explanations for this sex variation in the incidence of ACL injury have centered around differences in muscular strength, hormonal influence, physiologic laxity, and anatomic and structural differences.3,8,38
The proposed advantages of using hamstring tendons for ACL reconstruction in female athletes include ease of graft harvesting, low morbidity, avoidance of cosmetic defects, avoidance of patellofemoral problems, and easier rehabilitation. 24 The purpose of this prospective study was to determine whether the results of ACL reconstruction using quadruple-looped semitendinosus and gracilis tendons are equivalent in men and women at short-to-medium range follow-up.
Materials and Methods
Patient Characteristics and Inclusion Criteria
From October 1991 through October 1996, 690 patients underwent ACL reconstruction with autogenous grafts. All procedures were performed arthroscopically by a single surgeon (GRB). Of the 690 ACL reconstructions, 130 patients underwent quadruple-looped hamstring tendon autograft ACL reconstruction using the semitendinosus and gracilis tendons. All cases of bilateral or chronic ACL reconstruction, workers’ compensation cases, and litigation cases were excluded from this study. All patients with fixation other than Endobutton (Acufex Microsurgical Inc., Mansfield, Massachusetts) proximally and button or post distally were also excluded. Sixty-five patients satisfied the inclusion criteria and were available for the minimum 2-year follow-up. Thirty-nine of these patients were women and 26 were men. Only patients with acute ACL injuries (less than 3 months old) without other pathologic ligament disorders were included to avoid associated-injury bias. The average age of the patients was 29 years (range, 13 to 48) for men and 23.2 years (range, 14 to 47) for women. Injuries were sustained in 13 right knees and 13 left knees for the men and in 18 right knees and 21 left knees for the women.
Data Collection
The results of each patient's initial examination, surgical findings, and follow-up examinations were prospectively entered into a computerized relational database (FoxPro 2.6; Microsoft Corporation, Redmond, Washington). Patients were prospectively evaluated using objective and subjective criteria both preoperatively and postoperatively. All patients were examined by the senior author (GRB) at each follow-up visit. Postoperative data were collected at 3, 6, and 12 months after surgery and annually thereafter.
Objective Analysis
Objective parameters used for evaluation included examination for the presence of effusion or crepitus, Lachman and pivot shift testing, KT-1000 arthrometer testing (MEDmetric Corp., San Diego, California) for side-to-side differences, modified Lysholm knee function scores, 20 and Tegner activity scores. 34 The Lachman examination was performed with the knee in approximately 30° of flexion and was compared with examination of the contralateral extremity. Grading was defined as 0 (normal compared with uninjured knee), 1+ (increased excursion with an end point), or 2+ (increased excursion without an end point). Pivot shift testing was graded as normal, 1+ (glide), 2+ (clunk), or 3+ (gross subluxation). Manual maximum KT-1000 arthrometer side-to-side differences in anterior tibial translation were recorded with the knee in 25° of flexion. Results were defined as clinical failures by either a 2+ Lachman test (no end point), a 1+ or greater pivot shift test, greater than 5-mm side-to-side difference on KT-1000 arthrometer testing, or requirement of revision ACL reconstruction for repeat injury. Lysholm knee function scores were determined both preoperatively and postoperatively. 20 Patients’ activity levels were quantitated using the Tegner activity scale 34 ; preinjury scores were compared with those at final follow-up. Postoperatively, all patients were evaluated radiographically for accurate tunnel placement.
Subjective Analysis
Postoperative subjective analysis consisted of a 15-item visual analog scale questionnaire (Fig. 1). Patients rated their symptoms on a scale of 0 (no problems) to 10 (severe problems). These questions addressed subjective symptoms of pain, swelling, instability, locking, limitations of motion, grinding, and difficulties with various sports maneuvers. Statistical analyses were performed using chi-square and two-sample t-tests.
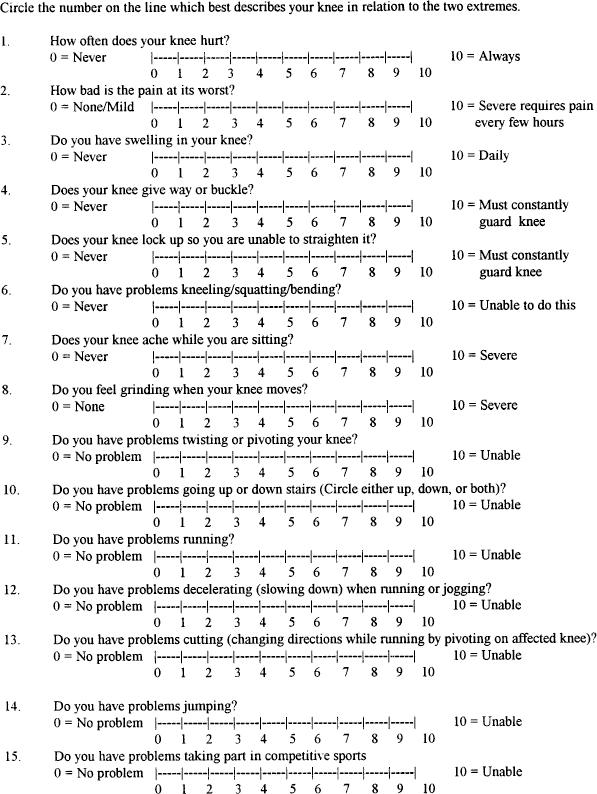
Subjective visual analog scale answered by all patients.
Associated Injuries
Female Patients
Among the 39 female patients, 35 (90%) injuries occurred during sports participation; 10 (26%) were considered contact injuries. There were associated injuries in 14 patients (36%). None of these injuries involved other knee ligaments. All associated lesions involved either the meniscus or the articular cartilage. There were three medial meniscal tears: two were repaired using an inside-out technique and one required with partial meniscectomy. There were seven lateral meniscal tears: two of these tears were repaired using an inside-out technique and five required partial meniscectomy. There were five osteochondral lesions, three of which required debridement and one that required drilling.
Male Patients
Among the 26 male patients, 19 (73%) injuries occurred during sports participation; 5 (19%) were sustained by a contact mechanism. There were associated injuries in 13 of the 26 male patients (50%). One patient had a loose body removed arthroscopically. All associated lesions involved either the meniscus or the articular cartilage. There were nine associated medial meniscal lesions: five were repaired using an inside-out technique and four required partial meniscectomy. Six patients had lateral meniscal tears: three were repaired using an inside-out technique and three required partial meniscectomy. There was one associated osteochondral lesion that was lightly debrided and lavaged arthroscopically.
Preoperative Evaluation
All reconstructions were performed within 3 months of the original injury. Initially, patients were prescribed a physical therapy program to regain motion and decrease swelling preoperatively. Surgery was generally delayed until at least 2 weeks after the injury and until full range of motion had been restored to the injured extremity.
Operative Technique
A single-incision endoscopic technique for ACL reconstruction using quadruple-looped hamstring tendons was employed in all cases. All patients underwent examination under anesthesia and diagnostic arthroscopy with treatment of meniscal lesions before graft harvest. Semi-tendinosus and gracilis tendons were then harvested through a 3-cm vertical incision on the anteromedial aspect of the proximal tibia 3 to 4 cm distal to the joint line. The distal insertion of the tendons was released and prepared using a whipstitch with nonabsorbable suture. Commercially available tendon strippers were used to harvest the grafts. The proximal ends were prepared similarly with a nonabsorbable whipstitch. After preparation, all grafts were preconditioned using the Graftmaster board (Dyonics, Smith & Nephew, Memphis, Tennessee) at 15 pounds of tension for 10 to 20 minutes. Notchplasties were performed arthroscopically to allow for adequate graft placement and to avoid impingement.
The tibial guide pin was placed using a tibial guide through the footprint of the ACL adjacent to the anterior horn of the lateral meniscus and the tibial tunnel was reamed. All tunnels were reamed to graft size as determined by graft sizers. The femoral guide pin was placed 5 mm anterior to the posterior cortex to allow for a 1- to 2-mm posterior cortical rim after reaming at the 11 o'clock (right knee) or 1 o'clock (left knee) position. Intraoperative radiographs were obtained to ensure proper femoral guide pin placement. The femoral tunnel was reamed just until the anterolateral femoral cortex was reached but no further (approximately 30 to 40 mm).
Graft fixation was performed with an Endobutton on the femoral side and either a button or post (suture tied over a screw with spiked washer) on the tibial side. The tibia was loaded with a maximal posterior force during fixation on the tibial side to minimize graft laxity present at the time of surgery. An intraoperative radiograph was again obtained to verify correct tunnel position and suction drains were placed. The knee was placed in an immobilizer until physical therapy was initiated on the 1st postoperative day.
Postoperative Rehabilitation
The rehabilitation protocol was identical for both groups. Patients immediately started a passive range of motion exercise program and maintained a nonweightbearing status for 3 weeks in a hinged brace. At 6 weeks after surgery the brace was removed and active exercises were initiated. No running was allowed until 3 months after surgery. Return to full sports activity was generally permitted at 6 months.
Complications
One male patient had a failed repair of a lateral meniscal tear and subsequently underwent partial meniscectomy. One female patient had a failed lateral meniscal repair and also underwent partial meniscectomy. There were no infections, nerve injuries, or thrombophlebitic or anesthesia-related complications.
Results
Female Patients
The average preoperative Lysholm score for female patients was 46.6 (range, 28 to 90), and the average preinjury Tegner activity level was 6.54 (range, 0 to 7). The average follow-up was 40.9 months (range, 24 to 81). In 11 knees (31%) the Lachman test was graded as 1+ and in 4 knees (8%) it was graded as 2+. The remaining 24 knees were graded as normal by Lachman examination. In eight knees (18%) there was a 1+ pivot shift result and in one (3%) there was a 2+ pivot shift result. The remaining 31 knees were graded normal on pivot shift testing. The average manual maximum KT-1000 arthrometer side-to-side difference within this group was 1.88 mm (range, 0 to 6.5). Thirty-one patients (79%) had a side-to-side difference of 3 mm or less, six patients (13%) had a difference of between 3 and 5 mm, and three patients (8%) had a difference of greater than 5 mm. The average postoperative Lysholm score at final follow-up was 89.7 (range, 55 to 100), and the average postoperative Tegner activity level was 5.17 (range, 2 to 7), which was significantly decreased from the preinjury value of 6.54 (P = 0.001).
Male Patients
The average preoperative Lysholm score for the male patients was 45.25 (range, 14 to 68), and the average preinjury Tegner activity level was 5.11 (range, 0 to 7). The average follow-up was 39.0 months (range, 24 to 60). In 2 patients (8%) the Lachman test was graded as 1+, and in the remaining 24 patients the knee was graded normal by Lachman examination. In all 26 patients the pivot shift examination was normal. Manual maximum KT-1000 arthrometer side-to-side differences among the male patients averaged 1.25 mm (range, 0 to 7). There were 23 knees (88%) with a difference of 3 mm or less, 2 knees (8%) with a difference of 3 to 5 mm, and 1 knee (4%) with a difference of greater than 5 mm. The average postoperative Lysholm score for the male patients was 90.9 (range, 81 to 100), and the average Tegner activity level was 5.26 (range, 3 to 7). Compared with the preinjury value of 5.11, this increase was not statistically significant.
Failures
Female Patients
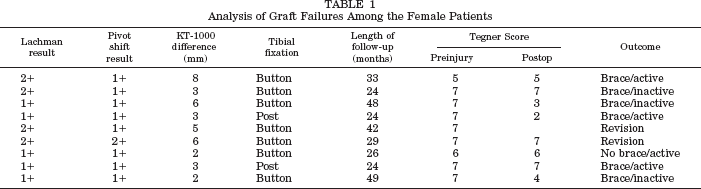
Failure of the reconstruction had occurred in nine cases (23%) at final follow-up. The examination results of the female patients with failed reconstructions are detailed in Table 1. Two of these patients have undergone revision ACL reconstruction with patellar tendon allografts and are doing well. The other two patients declined revision surgery and are currently using braces and modifying their activities to minimize symptomatic instability.
Analysis of Graft Failures Among the Female Patients
Male Patients
There was one patient (4%) with a failed result; he had a 7-mm side-to-side difference on KT-1000 arthrometer testing. However, this patient had a normal Lachman test result, a negative pivot shift result, and was doing well clinically at the latest follow-up. No male patients developed a positive pivot shift test, a 2+ Lachman result, or underwent revision surgery.
Subsequent Surgery
Three female patients underwent repeat arthroscopic surgery for meniscal tears. One of these patients had a partial lateral meniscectomy at 34 months postoperatively. Another patient underwent a medial meniscal repair with Bionix arrows (Smith & Nephew, Memphis, Tennessee) at 48 months postoperatively; she did not have a medial meniscal tear at the time of her ACL reconstruction. The third patient had a partial lateral meniscectomy at 18 months after her ACL reconstruction. Two of these meniscal tears were considered to result from a failed meniscal repair that never healed. None of the female patients with failed grafts had failed meniscal repairs clinically. One male patient with a stable reconstruction had a partial lateral meniscectomy at 18 months after his primary ACL reconstruction.
Comparison of Male Patients versus Female Patients
The male and female patients were comparable at the time of initial evaluation based on our objective criteria. Comparison of objective results between the male and female populations revealed no significant differences with regard to effusion or crepitus, KT-1000 arthrometer measurements, or Lysholm scores. However, at the follow-up examination, a higher number of female patients than male patients were graded as having a 1+ Lachman result, which was statistically significant (P < 0.05). Twelve female patients (31%) had a 1+ Lachman result on final follow-up examination, compared with only two male patients (7%). Seven female patients were graded as having a 1+ pivot shift test result, compared with none of the male patients (P < 0.05).
When comparing the extension difference between the operated leg and the opposite extremity, we found that female patients had a greater difference than did male patients (P = 0.031). The average extension loss was 2° for the male patients (range, 0° to 6°) and 2.75° for the female patients (range, 0° to 15°). Thirty-three female patients (85%) had an extension difference of less than 5°, 3 (8%) had a difference of 6° to 10°, and 3 (8%) had a difference of greater than 10°. In contrast, 24 of 26 male patients (92%) had an extension difference of less than 5°, 2 had a difference of 6° to 10°, and none had a greater than 10° difference. However, at the latest follow-up examination the lowest Lysholm score for the three female patients with a difference greater than 10° was 91, and the lowest Tegner activity level was 4, indicating that the objective knee scores were not significantly affected by the loss of extension. The effect of extension loss on final outcome was not otherwise evaluated.
A subjective comparison between the two groups was performed by comparing the postoperative visual analog scale scores from the 15-item questionnaire. Female patients had a significantly higher frequency (P = 0.024) and intensity (P = 0.010) of pain postoperatively than did male patients. No other differences were noted.
The patients’ ability to return to their preinjury activity levels was graded using the Tegner activity scale. Female patients had a significant decrease in their Tegner levels; from 6.54 before injury to 5.17 at the final follow-up (P < 0.05). Female patients, on average, therefore, did not return to their preinjury activity level. The increased postoperative Tegner level in the male population implies that male patients not only returned to their preinjury level of activity but also surpassed it in some cases. Comparison of their preinjury mean Tegner level (5.11) with their mean Tegner level at final follow-up (5.26) revealed no statistically significant difference.
There was a statistically significant difference in the rate of graft failure between the female and male patients. Nine female patients (23%) and one male patient (4%) sustained a failure of their reconstructed ACL graft. Success rates for maintenance of integrity of the graft by our objective criteria (a negative pivot shift result, a 0 or 1+ Lachman test result, and less than 5-mm side-to-side arthrometer difference) were 77% in female patients and 96% in male patients. No patients had any evidence of tunnel malposition on postoperative films.
Discussion
Success rates for ACL reconstruction using autogenous hamstring tendons have ranged from 82% to 90%.1,4,12,17,36,37 The results of this study are comparable with these success rates for the male patients but not for the female patients. The success rate for male patients was 96% compared to 77% for the female patients. Most previous reports have not demonstrated any statistically significant differences when comparing male and female patients using either hamstring or patellar tendon grafts.1,2,21,28,31,32 Siegel and Barber-Westin 32 evaluated results in 82 patients with quadruple-looped hamstring ACL reconstructions using femoral button fixation and tibial button or staple fixation. Thirty-four of these patients were women; no significant sex differences were reported with regard to anterior-to-posterior displacements, symptoms, functional limitations, outcomes, or rating scores. In similar studies, Aglietti et al. 1 and Maeda et al. 21 fixed quadrupled hamstring tendon autografts outside the bone tunnel with posts or staples and found no significant differences between the sexes. Corry et al. 7 compared 82 patellar tendon ACL reconstructions with 85 hamstring tendon ACL reconstructions and did note a statistically significant increase in KT-1000 arthrometer differences for female patients in the hamstring tendon group. The average difference was 2.5 mm, which was significantly different from the male patients with hamstring tendon grafts (P < 0.0001), the male patients with patellar tendon grafts (P < 0.0003), and the female patients with patellar tendon grafts (P < 0.001). In their study, metal interference screws were used for aperture fixation in all groups.
In our study, female patients had increased graft laxity compared with male patients, as demonstrated by KT-1000 arthrometer testing, Lachman tests, and pivot shift tests. Our criteria for failure included a 2+ Lachman result, a 1+ or greater pivot shift test result, a greater than 5-mm side-to-side difference with KT-1000 arthrometer testing, or revision surgery. The one male patient with a failed result had a normal Lachman test, a negative pivot shift test, and a 7-mm difference on KT-1000 arthrometer testing, which brings into question the reliability of KT-1000 arthrometer data in classifying this patient as having a failed result. Aglietti et al., 1 in evaluating 69 ACL reconstructions, also used arthrometer differences of greater than 5 mm and a positive pivot shift test as criteria for determining graft failure. Likewise, Siegel and Barber-Westin 32 defined graft failure with KT-1000 arthrometer differences of greater than 5.5 mm or a 2+ pivot shift result. Our definition of 1+ pivot shift result (glide) as a criterion for failure did increase the failure rate for female patients and may be criticized as a limitation of this study. However, using the same criteria, no male patients had a positive pivot shift result with the same fixation and no associated ligamentous instability.
Postoperative radiographic evaluation for both groups did not reveal any cases of aberrant tunnel placement that may have contributed to increased graft laxity, which has been demonstrated as a cause for failure in other studies. 18 Patients in this study did not undergo an aggressive postoperative rehabilitation program, which also has been associated with increased graft laxity as shown by KT-1000 arthrometer examination. 25 An analysis of the failures in the female patient group (Table 1) demonstrates a poor correlation of KT-1000 arthrometer side-to-side arthrometer differences with Lachman test results, pivot shift test results, and clinical failure in this study.
Although it is difficult to determine if the increased instability seen in our female patients was truly symptomatic, the female patients did complain more than the male patients of increased pain frequency and intensity postoperatively as judged by the results of the visual analog scale. The increased visual analog scores noted in the female patients may reflect their greater loss of extension compared with the male patients. Because the men had more meniscal tears (58%) than the women (26%), it is unlikely that associated meniscal or osteochondral lesions accounted for the higher visual analog and Tegner scores reported for the female patients. In addition, caution should be used in attributing the lower Tegner levels and Lysholm scores to the increased laxity seen in female patients, because other studies have demonstrated that KT-1000 arthrometer side-to-side differences are not directly correlated with knee outcome scores.33,35
Tegner activity levels revealed that the female patients were more active than the male patients before their initial injury. This may reveal some selection bias on the part of the surgeon. There was an apparent tendency toward use of hamstring tendon grafts in female athletes and bone-patellar tendon-bone in male athletes. However, regardless of the selection bias, return to activity levels have traditionally been used as a means of judging the success of ACL surgery. Even though the average age of the female patients was lower than that of the male patients, the female patients did not achieve their preinjury activity levels after surgery, whereas the male patients did. The female patients also did not demonstrate a statistically significant difference from the male patients regarding the number of meniscal injuries or osteochondral injuries that could have accounted for their higher visual analog and lower Tegner levels.
This study has several limitations that warrant review before definitive conclusions can be made. The current fixation techniques used for soft tissue grafts are superior to those used during the time of this study; this older technique likely contributed to the increased laxity noted in the female patients. Post fixation combined with interference screws has been shown to be superior to post fixation alone in cadaver studies. 27 Also, the use of sutures with post fixation has also been shown to have decreased failure strength. 22 The tibial fixation techniques we used varied between posts with spiked washers and buttons and could be an additional confounding variable. Another factor to consider is the generalized ligamentous laxity that is more frequently present in women. This factor was not evaluated and could have contributed to the increased graft laxity noted in some of the female patients. Also, the female patients had higher preoperative Tegner activity levels than the male group, which may reflect a difference in activity level between the groups that could bias the results. The reasons for the lower postoperative Tegner scores in the female patients were not evaluated and could be secondary to factors other than knee stability.
Despite the limitations, the value of this study lies in the fact that the female patients had a higher failure rate than the male patients and greater laxity than male patients at 2 years’ minimum follow-up in a study that involved the same surgeon, the same postoperative protocol, similar activity levels and ages of patients, and similar graft fixation methods. Although it would be interesting to determine why the female patients had poorer results, causes for graft failure such as neuromuscular differences, bone density, quality and size of the hamstring tendons, and hormonal factors were not evaluated. It is the opinion of the senior author that the women in this study generally had smaller tendons than their male counterparts, which potentially contributed to the increased failure rate and laxity observed at final follow-up. However, the size of the tendons was not specifically evaluated in this study.
In conclusion, the findings of this study show a tendency toward increased graft laxity in women with acute, isolated ACL ruptures reconstructed with quadruple-looped hamstring tendon autograft with fixation outside of the bone tunnels. The female patients had more pain than the male patients and a significantly increased number of 1+ Lachman and 1+ pivot shift results on follow-up examination. They also did not reach their preinjury activity level as judged by Tegner activity levels. The success rate for the female population (77%) was lower than the success rates shown in previous studies, whereas the success rate for the male patients (96%) was comparable with those of earlier studies. The quadruple-looped hamstring tendon autograft may be an inferior graft construct for ACL reconstruction in women when implementing fixation outside of the bone tunnels on the femoral and tibial sides. Further research is necessary to determine whether sex affects final graft laxity and consequently graft selection when using current fixation techniques.