
Abstract

Head injuries incurred during sports activities account for 5% to 10% of all head injuries treated in hospitals. 24 Statistics compiled by the U.S. National Center for Catastrophic Sports Injury Research indicate that the highest rates of severe head and neck injuries occur in football, gymnastics, ice hockey, and wrestling. 8 Soccer players have been regarded as having a low risk of severe nervous system injuries, although minor and mild head injuries are common.10,13 We report the case of a soccer player who developed a delayed epidural hematoma after a head injury during a soccer match. Such an occurrence is rare.
Case Report
A 19-year-old soccer player was heading a ball when he crashed into an opponent, hitting his right frontoparietal region against the opponent's left frontal scalp. He fell to the ground and was unconscious for 20 to 30 seconds. He was then immediately transported to the nearest hospital. Twenty minutes after the accident, he was alert and conscious without neurologic deficit, but he had amnesia of the traumatic event.
The general examination revealed a superficial contusion to the right frontal scalp. Forty-five minutes after the trauma the patient developed generalized seizures. Intravenous therapy was promptly established with anticonvulsion agents (lorazepam 4 mg), which stopped the seizures. A CT scan, performed 80 minutes after the trauma, revealed no intracranial lesions (Fig. 1A). Because the hospital had no neurosurgical department, the patient was transferred to our regional trauma center. On admission, neurologic examination showed a slight psychomotor slowing and slurred speech, which was thought to have been caused by lorazepam administration, in the absence of other neurologic deficits. The Glasgow Coma Scale score was 15 of 15. Routine laboratory investigations and electrocardiography were in the normal range. Eight hours after the trauma, he had nausea, vomiting, and a headache. An immediate repeat CT scan showed a bulky right frontal delayed epidural hematoma (Fig. 1B). Emergency craniotomy with removal of the clot was performed. His postoperative course was uneventful, and on the 10th postoperative day the patient was discharged in satisfactory clinical condition and was prescribed phenytoin (300 mg/day) as a prophylactic measure. Postoperative CT scans demonstrated that the hematoma had been evacuated. At the 9-month follow-up the patient was well; no epileptic seizures had occurred. Quantitative electroencephalography and neuropsychological examination findings were within the normal range. He currently engages in jogging, swimming, and cycling.
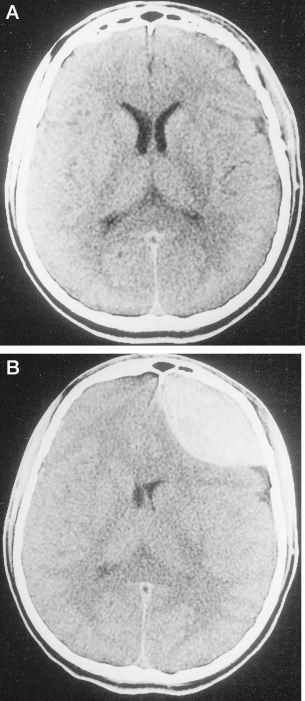
A, normal noncontrast CT scan taken 80 minutes after the head trauma. B, a CT scan was performed again after 8 hours; a right frontal delayed epidural hematoma is evident.
Discussion
Since the codification of soccer rules in Great Britain in 1863, soccer has become the most popular sport worldwide, with an estimated 120 million amateur participants. In Europe, soccer is responsible for about 50% of all sports-related injuries. 24 Soccer players have a high risk of soft tissue contusions, ligament sprains, and muscle strains of their lower limbs. The ankle and knee joints and the thigh and calf muscles are the most commonly involved sites.2,13 Mild head injuries, including lacerations of the scalp, and dental, ophthalmologic, and closed-head trauma, also represent a significant cause of morbidity,2,13,14,20 accounting for 3% to 5% of all soccer injuries. 20 Repeated head microtraumas (heading the ball included) may cause chronic, permanent organic brain damage in soccer players, leading to attention, concentration, and memory deficits.14,15,25 Severe head injuries, however, are rarely reported, which is at variance with other contact-collision sports where the occurrence of cerebral hemorrhagic contusion, subarachnoid hemorrhage, and intracerebral, subdural, or epidural hematomas has frequently been described.5,7,8,17–19,26
Our patient sustained an apparently mild head injury, with brief loss of consciousness, and had no radiologic signs of fracture or intracranial lesion on admission. Eight hours later, however, a cranial CT scan revealed a large epidural hematoma, whose time course fits the criteria for diagnosis of delayed epidural hematoma.11,21,22 Delayed epidural hematomas account for about 10% of all epidural hematomas3,4,12 and, although rare, may occur after minor head trauma, 1 even in the absence of precipitating factors such as medically or surgically induced drop of intracranial pressure, rapid correction of shock, 4 and coagulopathy. As far as we are aware, this is the first documented case of delayed epidural hematoma that occurred as the result of a soccer injury.
Although unusual, this case report suggests that the risk of head trauma in soccer players is probably underestimated, and it raises a few specific issues related to the features and the rules of soccer. For instance, the use of protective helmets, which has undoubtedly decreased the severity of head injuries in other sports, 9 is hardly applicable to soccer, since it would change the characteristics of the game. 10 In soccer, unlike in other sports, a substitution for a player during the game is definitive, and therefore the decision to remove an injured player from the match may be made with some reluctance.§
In collegiate soccer in the United States, players may be substituted for and reenter the game.—Editor.