
Abstract
Over the last several decades there has been an improved understanding of the intricate anatomy that provides stability to the glenohumeral joint. In addition, significant advances in identifying the pathologic etiology of the unstable shoulder have occurred because of basic science glenohumeral ligament cutting studies, clinical evaluation, and the advent of arthroscopic evaluation and treatment of the unstable shoulder. This article will review the pertinent anatomy of the normal glenohumeral joint and will carefully review the pathoanatomy found in the unstable shoulder. Sports medicine specialists who treat athletes with unstable shoulders should have a firm understanding of both the normal and pathologic shoulder conditions to be able to provide the best care for these athletes.
History of Shoulder Instability
The pathophysiology of the unstable shoulder has generated interest for over 1000 years. Hippocrates is credited for one of the most detailed early descriptions of an anterior dislocation, including the anatomy and surgical treatment. 1 In the early 1900s, many surgeons postulated a variety of mechanisms for the unstable shoulder. Initial reports by Perthes, 50 Thomas, 62 and Bankart 5 suggested that the capsule and glenohumeral ligaments played a significant role in the stability of the shoulder. Disruption of the capsule and ligaments was believed to be responsible for recurrent shoulder instability.
A proliferation of nonanatomic operative procedures in the middle 1900s ventured away from the pathologic processes suggested by the previously mentioned reports. Bone grafting of the glenoid, tendon and bone transfers, and subscapularis muscle-shortening procedures became increasingly popular, partly because of the technical difficulties encountered with the Bankart procedure.24,36,42,45 Unfortunately, these nonanatomic procedures led to an unacceptable incidence of recurrence and a high number of complications.2,16,23,25,66,79,80
Biomechanical studies, beginning with the classic study of Turkel et al. 69 in 1981, returned the focus to the pathologic processes responsible for the unstable shoulder. The significant contribution of the glenohumeral ligaments was more clearly elucidated from this study. Arthroscopic intervention in the shoulder coincided with these studies and demonstrated that the glenohumeral ligaments were discrete, critical structures.
An intricate balance between the static and dynamic stabilizers confers the stability of the shoulder joint. 58 Static stabilizers include the glenoid labrum, glenohumeral ligaments and capsule, and rotator interval. The dynamic constraints include the rotator cuff musculature and the scapular rotator muscles. Any imbalance in this relationship can lead to shoulder instability. Furthermore, a thorough understanding of the normal anatomy and anatomic variations is critical to differentiate them from pathologic findings.
In addition to the previously mentioned topics, proprioceptive characteristics of the intact and the pathologic shoulder will be addressed in this study. Finally, it is crucial to remember that shoulder laxity does not imply a pathologic process and needs to be differentiated from instability. In fact, several studies have demonstrated significant glenohumeral translations in shoulders that are not clinically symptomatic.21,38
Static Stabilizers of the Glenohumeral Joint
Labrum: Normal and Variants
The labrum is a fibrocartilaginous bumper that is circumferentially attached to the glenoid rim (Fig. 1). It is loosely attached superiorly, and great anatomic variability in this region has led to the inappropriate treatment of normal variants. 57 A sublabral hole or sulcus is commonly found and should not be confused with a Bankart lesion. If the “lesion” is above the transverse glenoid equator, then it is rarely a pathologic lesion. Conversely, the anteroinferior labrum is intimately attached to the glenoid rim, with detachment indicating abnormalities. A recent vascular injection study has shown that the labrum is vascularized throughout the peripheral attachment of the joint capsule. 12 This may have clinical applicability in determining whether labral tears are repairable.
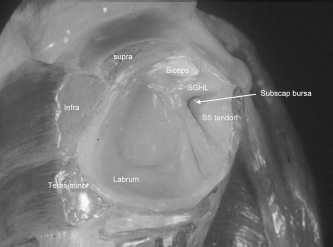
Cadaveric view of a normal glenoid labrum.
The superior part of the labrum inserts directly into the biceps tendon distal to the insertion of the tendon to the supraglenoid tubercle. Since the biceps tendon inserts on the supraglenoid tubercle (5 mm medial to the superior edge of the glenoid), there is a synovial recess beneath the biceps tendon and that part of the labrum. This can easily be mistaken for a SLAP (superior labrum, anterior to posterior) lesion, and careful inspection will reveal a firm attachment of the biceps anchor.
The labrum has three key roles in contributing to stability of the glenohumeral joint. First, it doubles the anteroposterior depth of the glenoid socket from 2.5 to 5 mm and deepens the concavity to 9 mm in the superior-inferior plane. 26 The labrum is analogous to a chock-block preventing an automobile's wheel from rolling downhill. 19 A recent biomechanical study showed that labral resection reduced resistance to translation by 20% in shoulders that were subjected to a compressive load. 34 Second, the labrum enhances stability of the joint by increasing the surface area of contact for the humeral head. 34 Finally, and perhaps most importantly, the labrum serves as a fibrocartilaginous ring to which the glenohumeral ligaments attach.
Labrum: Normal Variants
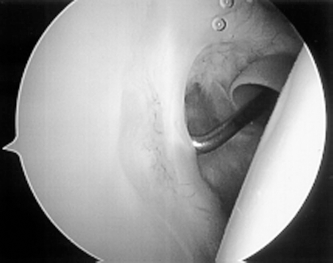
Normal variations of the capsulolabral complex are quite common (13.5% in one large series) and can be mistaken for pathologic lesions. 77 One such variant is the sublabral foramen in the anterosuperior quadrant of the shoulder. A cord-like middle glenohumeral ligament can also be easily confused for a traumatic disruption of the labral-ligamentous complex (Fig. 2). The Buford complex is a cord-like middle glenohumeral ligament found in conjunction with an absent anterosuperior labrum complex. 77
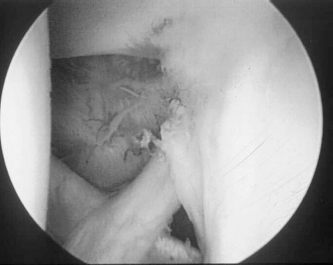
Cord-like middle glenohumeral ligament (MGHL).
Labrum: Pathologic
Anteroinferior Labral Lesions.
There have been several pathologic lesions described in relation to the anteroinferior labrum. The Bankart lesion is classically described as the detachment of the anteroinferior labrum with its attached inferior glenohumeral ligament complex (Fig. 3). Bankart initially identified detachment of the labrum in four patients with recurrent glenohumeral instability and dubbed it the “essential lesion.” 6 Bankart later reported the excellent results of labral reattachment (“Bankart procedure”) in 27 patients. 5 Emphasis was placed on anatomically repairing the torn labrum. Numerous reports have documented the success of this operation.20,33,52,53
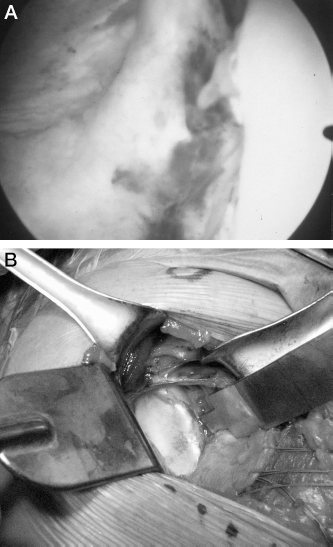
A, arthroscopic view of a Bankart lesion with acute detachment of the anteroinferior labrum/inferior glenohumeral ligament (IGHL). B, open view of a Bankart lesion.
Neviaser 41 described the ALPSA lesion (anterior labral periosteal sleeve avulsion) as a pathologic finding similar to the Bankart lesion, with one notable difference: the anterior scapular periosteum does not rupture and the inferior glenohumeral ligament, labrum, and periosteum are stripped and displaced in a sleeve-type fashion medially on the glenoid neck (Fig. 4). 41 Differentiation of an ALPSA lesion from the much more common Bankart lesion is essential in properly managing these lesions.

Axial MRI demonstrating an anterior labral periosteal sleeve avulsion.
Although the open treatment of unstable shoulders has led to a high percentage of successful results, arthroscopic Bankart repairs have not had consistently successful outcomes. The failure rates after arthroscopic Bankart repair have ranged from 5% to 60%.3,28,37,56,71
Several explanations may account for these varying results. First, labral detachment may not be solely responsible for the increased anterior glenohumeral translation necessary to produce a shoulder dislocation. This theory was tested in a recent biomechanical study by Speer et al. 60 A simulated Bankart lesion was created in nine fresh, intact cadavers and caused increases in anterior translation at all positions of elevation. However, these increases were small; the maximum mean increase was only 3.4 mm. The authors hypothesized that additional abnormalities are necessary to allow for glenohumeral dislocation. Simple reattachment of the torn labrum, therefore, may not properly retension the inferior glenohumeral ligament complex.
Indeed, Bankart later believed that he had placed too much emphasis on the labrum. He stated that “in every case the capsule is incised over the glenoid margin and any part internal to this (including the labrum) is excised.” 4 Critical review of Bankart's earlier papers may shed some light on this apparent contradiction. The “essential lesion” was actually a “detachment of the capsule from the fibro-cartilaginous glenoid ligament … .” Subsequently, general perception has been that labral detachment was the primary pathologic process when Bankart clearly was describing loss of tension in the inferior glenohumeral ligament.
General consensus today is that a Bankart lesion, in and of itself, is insufficient to allow the humeral head to dislocate. Therefore, surgical procedures that simply place the labrum back on the glenoid but do not properly restore tension in the inferior glenohumeral ligament complex are doomed to fail. We believe that this is one of the explanations for the unacceptably high failure rate of many of the previously reported arthroscopic studies for shoulder instability.
Superior Labral Lesions.
Lesions of the superior labrum (SLAP) were described clinically by Snyder et al., 57 but were not initially implicated in unstable shoulders. More recently, however, a small group of patients with recurrent shoulder instability was found to have anteroinferior labral and SLAP lesions. 74 All shoulders had a complex labral detachment from the 10 o'clock to 6 o'clock positions on the glenoid (right shoulder) corresponding to the entire posterosuperior, anterosuperior, and anteroinferior labrum (Fig 5). Five of the seven patients had successful treatment with absorbable tacks. One patient developed recurrent instability and underwent open reconstruction, and another patient developed stiffness that required arthroscopic release and manipulation.

Arthroscopic view of a SLAP lesion.
A recent biomechanical study by Pagnani et al. 48 confirmed the clinical findings of Warner et al. 74 Superior labral lesions were created in seven fresh-frozen cadavers and subjected to a series of mechanical tests in varying positions of glenohumeral elevation. There was no significant effect on anteroposterior or superoinferior translation with just an anterosuperior lesion (1 to 3 o'clock). However, there was a significant effect on anteroposterior and superoinferior translation with a complete lesion (10 to 3 o'clock). The relative increases in translation were small, although they may be related to the symptoms associated with an isolated lesion of the superior portion of the labrum.
Capsule/Glenohumeral Ligaments
Normal Anatomy.
Early investigators under-appreciated the importance of the glenohumeral ligaments. 35 Cadaveric studies helped to further elucidate the anatomy of these ligaments.17,46,55 Selective glenohumeral ligament cutting studies pioneered by Turkel and associates 69 led the way to fully appreciating the functional role of the glenohumeral ligaments. Criticism of selective cutting studies as being nondynamic led to subsequent investigations using strain gauge analyses. However, these dynamic studies confirmed the findings of Turkel et al. 69 and documented the contribution of the glenohumeral ligaments to shoulder stability.43,44,61
Arthroscopy has dramatically improved our understanding of the anatomy of the glenohumeral ligaments, normal variants, and pathoanatomic lesions.57,72,73 The glenohumeral ligaments are discrete thickenings in the capsule, with a number of anatomic variants having been described (Fig. 6). 15
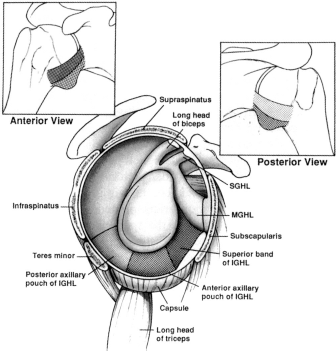
Anatomic drawings of the three regions of the inferior glenohumeral ligament (IGHL) from intracapsular and extracapsular views. MGHL, middle glenohumeral ligament; SGHL, superior glenohumeral ligament. (Reprinted with permission from Bigliani et al. 7 )
There is controversy concerning the relative roles of the coracohumeral ligament and the superior glenohumeral ligament. A recent study showed that the cross-sectional area of the coracohumeral ligament was significantly greater than that of the superior glenohumeral ligament. 9 In addition, the coracohumeral ligament had greater stiffness and ultimate load than did the superior glenohumeral ligament. These findings disputed earlier studies that showed minimal contribution of the coracohumeral ligament. 13
The coracohumeral ligament originates on the lateral surface of the coracoid process as an extraarticular structure and inserts into the greater and lesser tuberosities spanning the bicipital groove. The superior glenohumeral ligament courses from the anterosuperior labrum anterior to the biceps tendon and inserts superior to the lesser tuberosity near the bicipital groove. It is variable in size but is demonstrable in more than 90% of cases.13,15,43,73 These two structures in concert limit inferior translation and external rotation of the adducted shoulder and posterior translation of the flexed, adducted, internally rotated shoulder.
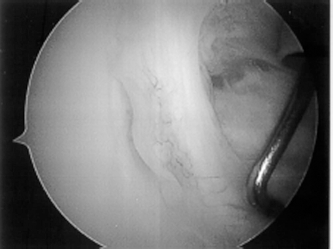
The middle glenohumeral ligament arises next to the superior glenohumeral ligament and extends laterally to attach on the lesser tuberosity in association with the subscapularis tendon (Fig. 7). The middle glenohumeral ligament is the most variable of the ligaments, and a number of anatomic variants have been described, as previously discussed. 77 The middle glenohumeral ligament limits anterior translation of the humeral head when the arm is abducted between 60° and 90°.44,69
The middle glenohumeral ligament (MGHL).
The inferior glenohumeral ligament complex extends from the anteroinferior labrum to insert just inferior to the middle glenohumeral ligament (Fig. 8). The inferior glenohumeral ligament complex has been shown to consist of three distinct parts: the anterior band, axillary pouch, and posterior band. 43 A recent study, however, showed that the posterior band was less consistent than the anterior band and the axillary pouch. 65 The inferior glenohumeral ligament functions like a hammock in preventing increased translation of the humeral head on the glenoid. With abduction, the entire complex moves beneath the humeral head and becomes taut. Conversely, with internal rotation, the complex moves posteriorly and limits posterior translation. Finally, with external rotation, the complex moves anteriorly and statically limits anterior translation.
The inferior glenohumeral ligament complex.
Pathologic Lesions.
Thomas 62 noted in 1909 that the “essential lesion” was a tear in the capsule that allowed glenohumeral dislocation. He found tearing of the anteroinferior capsule in cadavers after controlled dislocations. He concluded that recurrent dislocation of the shoulder is due to “an anterior hernial pouch of the capsule, and that the object of the operation should be to obliterate the hernial protrusion.” The recommended operation involved shortening the capsule and was successful in 33 of the initial 34 patients. 63
Likewise, Bost and Inman 10 found that redundant capsular pockets were present in shoulders surgically treated for recurrent instability. They also noted that there “must be initial tearing or stretching of the anterior capsular attachments.” Townley 67 introduced the concept of the “capsular mechanism” and suggested that loss of the anterior buffering mechanism of the capsule allows abnormal translation of the humeral head. He believed that the labrum added little more than a slight anterior barrier to dislocation. Operative repair in 19 patients with a technique similar to that of Bankart had no recurrences and allowed excellent return to vigorous activities. Numerous reports subsequently have described the clinical importance of the capsule in the anatomic and pathoanatomic situations.39,40,54
Curl and Warren, 14 Pagnani and Warren, 49 and Warren et al. 76 introduced the “circle concept” of capsular contribution to shoulder stability. Complete dislocation requires capsular deformation on the involved side as well as the opposite side of the joint. These authors found damage on both the anterior and posterior sides of the capsule in a cadaveric study of posterior instability. Other investigators have confirmed this concept using strain gauge analyses that show anterior and posterior capsular strain with anterior translation of the humeral head.11,17,61
As previously detailed, the literature was replete with reports about capsular redundancy, capsular stretch, capsular injury, and labral lesions. The unsolved question that remained was, what is the essential lesion of instability, or perhaps more importantly, is there an essential lesion of instability? A biomechanical study in 1992 greatly increased our understanding of the pathoanatomy in shoulder instability. 8 The inferior glenohumeral ligament was divided into three anatomic regions and tested to failure in uniaxial tension. Failure occurred at the glenoid insertion in 40% of specimens (Bankart lesion), in the intrasubstance in 35%, and at the humeral insertion in 25% of the specimens. Perhaps more important is that even in cases where the inferior glenohumeral ligament failed at its glenoid insertion, such failure occurred only after significant inferior glenohumeral ligament elongation. This concept of plastic deformation had not previously been described and was hypothesized to account for some of the more subtle glenohumeral joint instability observed clinically.
Assessing capsular stretch arthroscopically is difficult and continues to be a common etiologic factor leading to failure of arthroscopic stabilization techniques.28,37,56,71 The goal of the surgical procedure is to address all pertinent pathoanatomy. With increased awareness of this problem, newer techniques are being developed to attempt to address these issues. Laser capsulorrhaphy has been used to reduce the capsular stretch component of the injury. Early results are encouraging, although the long-term success is unknown and the cost and risk of avascular necrosis are drawbacks. A radiofrequency heat probe (Oratec, Menlo Park, California) has been introduced recently to deal with these concerns. Many surgeons have noted early clinical success but there remain no clinical data yet published to critically review this device.
Rotator Interval
The rotator interval is the triangular-shaped area marked by the anterior border of the supraspinatus tendon superiorly, the subscapularis tendon inferiorly, and the coracoid base laterally (Fig. 9). The capsule is structurally enhanced by the coracohumeral ligament and the superior glenohumeral ligament. Harryman et al. 22 have shown that the rotator interval has a significant role in glenohumeral stability. Significant increases in anterior, posterior, and inferior humeral head translation occurred after sectioning of the rotator interval.
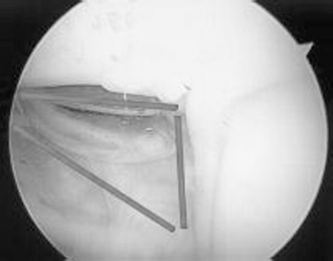
The rotator interval capsule.
Pathologic Defects.
Harryman et al. 22 studied the effects of sectioning the rotator interval capsule in eight fresh-frozen cadaveric shoulders. They found that the function of the rotator interval capsule is to limit inferior translation of the glenohumeral joint in the adducted shoulder and to provide stability against posterior dislocation in flexion or abduction-external rotation. In addition, this structure limits the range of flexion, extension, adduction, and external rotation.
Clinical experience has demonstrated wide variability in the rotator interval capsule, including everything from a small opening to a wide cleft. The difficulty exists in deciding what is abnormal and what is contributing to the pathologic instability. A clinical report of the open closure of isolated rotator interval defects on a small group of patients recently reported excellent short-term results. 18 We have seen patients, however, who have developed recurrent instability into a large, inferior pouch after this type of limited surgical repair. 32 Caution should be exercised, therefore, before isolated closure of the rotator interval capsule is performed as the only surgical procedure for recurrent instability. Arthroscopic rotator interval closure used in conjunction with other techniques may help decrease the higher arthroscopic failure rates. There is only one report of which we are aware that describes this technique. The report lists favorable results at very short-term follow-up but did not delineate the pathologic processes in which this technique should be performed. 68
Dynamic Factors
Rotator Cuff
One of the main criticisms of most of the investigational studies on shoulder instability is the inability to factor in the dynamic function of the musculature.11,78 Stability is achieved through three mechanisms: 1) joint compression, 2) coordinated contraction of the rotator cuff muscles guiding the humeral head into the glenoid throughout the full range of motion, and 3) glenohumeral ligament dynamization through direct attachment to the rotator cuff.
The rotator cuff is ideally positioned to provide a compressive load throughout the range of motion of the glenohumeral joint. Lippitt et al. 34 described this concept as “concavity compression” and showed that with the intact labrum the humeral head resisted tangential forces of up to 60% of the compressive load. A chondral-labral defect (Bankart lesion) was created in a recent cadaveric study by Lazarus et al. 30 An anteroinferior chondral-labral defect reduced the height of the glenoid by approximately 80% and decreased the stability by 65% in the direction of the defect. Wuelker and associates 78 used a dynamic model and found that the dynamic stabilization of the rotator cuff was comparable to glenohumeral joint concavity-compression described by Lippitt et al. 34 and Bigliani et al. 7
Coordinated rotator cuff contraction plays a significant role in the maintenance of stability of the glenohumeral joint. 7 Kronberg and associates 29 showed altered rotator cuff activity in patients with generalized ligamentous laxity when compared with normal controls. Warner et al. 75 further demonstrated altered rotator cuff strength in patients with symptomatic shoulder instability. Athletes who use overhead throwing motions and develop rotator cuff fatigue, therefore, are at increased risk for developing injury to the anterior glenohumeral ligaments and capsule. The role of the rotator cuff in maintaining stability has been demonstrated in the normal shoulder, the lax shoulder, and the unstable shoulder.
Recently, shoulders with rotator cuff tears were studied to determine the contribution of the rotator cuff to stability. 27 Displacement of the humeral head increased with an increase in the size of the rotator cuff tear, with or without translational forces applied. Although some studies have shown the posterior cuff to be more active in maintaining stability, Soslowsky et al. 59 recently showed that the supraspinatus tendon was a much more effective stabilizer.
Finally, as has been previously well documented, the glenohumeral ligaments are lax in the midranges of shoulder motion.30,34 Joint compression and coordinated cuff contraction does contribute to the stability in this range, as detailed here. However, anatomic studies as well as intraoperative observations have shown the intimate relationship of the glenohumeral capsule (and ligaments) to the rotator cuff. 17 It is possible, therefore, that the capsule and ligaments are tensioned during active contraction of the rotator cuff muscles. At this time, however, we are unaware of any literature that definitively demonstrates this ligament dynamization.
Biceps Tendon
Rodosky et al. 51 showed that the long head of the biceps muscle contributes to anterior shoulder stability by resisting excessive external rotatory forces that occur in the abducted and externally rotated position. They also showed that the biceps played a protective role by decreasing the stress placed on the inferior glenohumeral ligament. Pagnani and associates 47 supported these findings in a cadaveric study of 10 shoulders. Anteroposterior and superoinferior translations were reduced after a force was applied to the biceps tendon. They found that the role of the biceps was related to shoulder position. The biceps tended to stabilize the joint anteriorly with the arm in internal rotation, and it acted as a posterior stabilizer with the arm in external rotation.
Proprioception
Ligaments can stabilize a joint by providing neurologic feedback that directly mediates joint position sensibility and muscular reflex stabilization. This feedback mechanism is referred to as proprioception. A recent investigation has demonstrated neural structures and mechanoreceptors in the capsule and ligaments of the shoulder joint. 70 Lephart et al. 31 showed that proprioception of the symptomatic shoulder was disrupted in patients with glenohumeral instability compared with the asymptomatic extremity. Interestingly, these differences were eliminated after shoulder reconstruction, which suggests that reconstructive surgery restores some of the proprioceptive characteristics. Recently, Tibone et al. 64 evaluated 28 shoulders by somatosensory cortical-evoked potentials during arthroscopy. A direct afferent neurologic pathway between the proprioceptive receptors in the joint capsule and the cerebral cortex was demonstrated. This study did not, however, demonstrate a statistically significant difference between the reflex-arc results of patients with stable and unstable shoulders.
As our understanding of these proprioceptive feedback mechanisms continues to grow, it is hoped that we may be better able to treat patients with symptomatic instability nonoperatively. Obviously, much more research is necessary in the future to fully appreciate the role of proprioception in the unstable shoulder.
Summary
Our understanding of the pathophysiology of shoulder instability has improved over the last several decades. The primary abnormality is related to the labral detachment and associated loss of tension in the glenohumeral ligaments, and to injury to the capsular mechanism itself. When nonoperative intervention fails, treatment should be directed at these pathologic processes. This is true whether the surgeon chooses an arthroscopic or an open technique for repair.
The dynamic role of the rotator cuff is evolving and further research is necessary to better outline the exact mechanism of action between the static and dynamic stabilizers of the shoulder joint. Finally, proprioceptive feedback mechanisms have been demonstrated in the shoulder and provide exciting potential for future research and treatment of patients with unstable shoulders.