
Abstract

Dear Editor:
In reading the article entitled “Osteochondritis Dissecans of the Patellofemoral Joint” (January/February 2000, pages 63–67) by Drs. Peters and McLean, it was gratifying to note that the findings and conclusions regarding osteochondritis dissecans of the trochlea coincided generally with those that I presented at the International Arthroscopy Association meeting in Sydney, Australia, in 1987, and published in 1990. 2 Both of these works apparently escaped the authors’ attention. There are, however, several points of significant disagreement between my work and the one cited here.
The authors treated almost half of their patients with chondroplasty. While I have doubts about the benefit of this procedure at any site by any means, the doubts are compounded when it is used for osteochondritis dissecans. The articular cartilage in osteochondritis dissecans lesions is normal (Fig. 1), as was emphasized by Teale 3 and Paget 1 (who described the condition second to Teale, and apologized for not being familiar with Teale's priority), and by most authors since those publications. If the fragment with its normal cartilage has displaced, the floor of the crater is bone or thin fibrocartilage, so that, with the possible exception of smoothing the margins of the lesion, there seems to be little indication for chondroplasty.
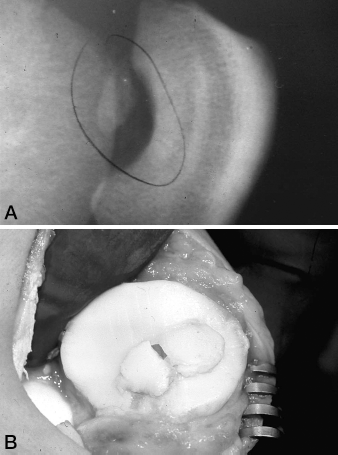
Osteochondritis dissecans of the patella. A, lateral radiograph of the patella showing the large bone fragment and corresponding site of origin. B, photograph of the patella at surgery. Except for the fracture surface of the fragment, the articular cartilage is completely normal.
It seems likely that, in some of their cases, the authors performed the chondroplasties for lesions other than osteochondritis dissecans. For instance, the patellar lesion in the top part of their Figure 3 is not consistent with findings of osteochondritis dissecans. There is no separate bone fragment, which is the essential lesion of osteochondritis dissecans; rather, there is an irregular area of resorption that is typical of the condition called dorsal defect of the patella. Other authors have also confused these conditions, treating cartilage lesions and cystic or lytic bone lesions, either of which excludes osteochondritis dissecans and both of which are typical of dorsal defect of the patella (Fig. 2). The radiologic literature suggests that these are insignificant incidental conditions, but our few cases were symptomatic and disabling.
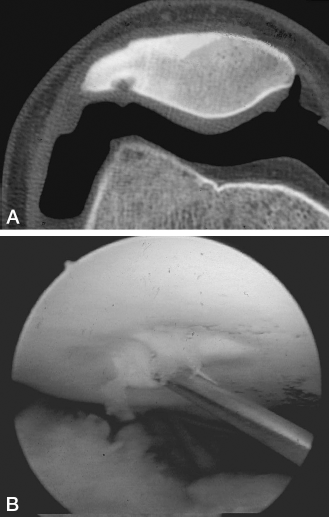
Dorsal defect of the patella. A, air-contrast CT of the patella, showing a lytic defect in the cortex and subchondral bone of the dorsal surface, without a separated bone fragment. The surface of the cartilage over the bone lesion is irregularly proud of the neighboring cartilage. B, arthroscopic view of the lesion with a biopsy needle in place. In contrast to osteochondritis dissecans, the cartilage is soft and uneven, and fibrillated centrally.
The authors deserve commendation for again emphasizing that, because of a missed or imprecise diagnosis, osteochondritis dissecans of the patellofemoral mechanism is probably more common than we think.
In regard to the “several points of significant disagreement” that you have raised pertaining to our recognition of osteochondritis dissecans and our treatment, first, I do not dispute the fact that the articular cartilage in osteochondritis dissecans is normal. The articular cartilage margins of the crater, however, vary enormously, depending on the site, size, the rate of separation, and whether it is fully detached. Approximately half of our patients underwent arthroscopy with associated chondroplasty, to tidy the articular margin of the crater. I did not do anything to the base of the crater, which I agree is bone and may be covered with scar tissue. This area is concave, and I see no reason to interfere with curettage, drilling, or the use of a “pic” in this area. These procedures are not part of a chondroplasty.
Second, I did perform a chondroplasty (to trim and tidy the articular margins) of the osteochondritis dissecans lesion of the patella shown in the top CT scan in Figure 3 of our article. This lesion is similar to that seen in the lower scan in Figure 3, except that the lesion has separated and was an osteochondral loose body removed from the joint at the arthroscopy.
Third, I agree with your distinction between osteochondritis dissecans and the irregular area of resorption called dorsal defect of the patella. In our series of 24 patellar osteochondritis dissecans lesions, there were only 4 cases that had a cystic or lytic appearance and that I considered were more likely an osteochondritis dissecans than a dorsal defect (similar to Fig. 3). Again, though, I think this is a point worth raising.
The dorsal defect of the patella is generally an insignificant incidental condition, noted on radiograph, CT scan, or MRI, but I have also found many of these defects that were symptomatic. These appear arthroscopically as a soft, irregular, hypertrophic, fibrocartilage at the lesion site. These were not included in this paper.