
Abstract
To evaluate the development of postoperative patellofemoral osteoarthritis, we performed a retrospective clinical and radiographic study of 100 patients who had undergone anterior cruciate ligament reconstruction with a bone-patellar tendon-bone autograft an average of 7 years before the follow-up. Radiographic evaluation showed no patellofemoral osteoarthritis in 53 patients (group I), mild osteoarthritis in 34 patients (group II), moderate osteoarthritis in 12 patients, and severe osteoarthritis in 1 patient (group III, moderate and severe changes). The average shortening of the patellar tendon was 2.4 mm in group I, 3.9 mm in group II, and 6.8 mm in group III. The placement of the femoral or tibial tunnel of the graft, as measured from lateral radiographs, did not correlate significantly with the degree of patellofemoral osteoarthritis. Patients who developed patellofemoral osteoarthritis experienced worse final outcomes, were more often dissatisfied with the condition of the operated knee, experienced more frequent pain and swelling in the knee joint, and had poorer range of motion and poorerquadriceps muscle strength than did patients without patellofemoral osteoarthritis. Only three patients had an unstable knee, and degenerative changes in the tibiofemoral joint were uncommon.
Anterior cruciate ligament insufficiency with anterolateral instability is likely to lead to degenerative osteoarthritis of the knee12,27; therefore, one reason for ACL reconstruction is prevention of these late degenerative changes of the knee joint. 11 Anterior cruciate ligament reconstruction with a bone-patellar tendon-bone autograft has shown good long-term results,25,26 and today this method is considered the standard treatment for ACL ruptures.6,10,22,25 However, the procedure is not without postoperative problems. One of them is patellofemoral osteoarthritis, which often causes pain, crepitation, and incomplete range of motion of the knee.1,2 Several authors have also reported that the patellar tendon shortens after an ACL reconstruction with a bone-patellar tendon-bone autograft,4,19–21 but the significance of this change with respect to the subjective and clinical outcome of the surgery is unclear. Aglietti et al. 2 compared the outcome of the bone-patellar tendon-bone procedure to that of reconstruction with the semitendinosus and gracilis tendons and observed that the former resulted in better stability but created more frequent patellofemoral problems.
The aim of this study was to evaluate the degree of patellofemoral osteoarthritis 5 to 9 years after an ACL reconstruction using bone-patellar tendon-bone autograft and to analyze its relationship to the amount of postoperative shortening of the patellar tendon and the placement of the femoral and tibial tunnels of the graft as measured from the lateral radiographs. We also examined the association between the presence of patellofemoral osteoarthritis and the clinical outcome of the patients.
Materials and Methods
Patients
The 144 patients who underwent an ACL reconstruction (using bone-patellar tendon-bone autograft and the miniarthrotomy technique) at the Tampere University Hospital between January 1989 and December 1991 formed the basic population of the study. Of these 144 patients, 130 (90%) could be contacted and interviewed with a questionnaire and 101 (70%) were able to attend the follow-up examination. One woman was pregnant and could not undergo radiographic examination, so the final number of patients for the injured-to-uninjured knee comparison was 100. Preoperative radiographs were not available for 14 patients, thus leaving 86 patients with radiographs of the knees before and after ACL reconstruction.
Among the 100 patients, there were 70 men and 30 women with a mean age of 31 years (range, 15 to 61) at the time of their surgical procedure. The mean delay between the time of injury and the reconstruction was 1.7 years (range, 0 days to 20 years). Forty-five patients were operated on within 1 week after injury, 6 between 1 and 2 weeks, 3 between 2 and 8 weeks, 7 between 2 and 6 months, 9 between 6 and 12 months, and 30 more than 1 year after injury. The mean follow-up time was 7.0 years (range, 4.6 to 8.8).
Operative Technique and Postoperative Rehabilitation
A miniarthrotomy technique with a bone-patellar tendon-bone autograft was used for all patients. A 10-cm longitudinal skin incision was made in the midline of the patellar tendon. The superficial fascia was reflected and the medial and lateral edges of the tendon defined. The central third of the tendon, approximately 9 mm in width, was removed with bone plugs at both ends. A miniarthrotomy was then performed, with the underlying fat and synovium incised in a sagittal direction and the intercondylar area exposed. A notchplasty was performed so that the osteochondral junction at the posterior inlet of the femoral notch could be felt.
A drill guide was used for precise placement of the femoral and tibial drill holes because one of the most important parts of the operation was to ensure the accurate anatomic location of the drill holes. The patellar tendon graft was fitted (with the bone plugs at both ends) into drilled holes and fixed with 6.5–mm AO cancellous screws inserted between the plug and the bony tunnel. The femoral site was fixed first, and, before screwing the tibial site, the isometric position of the graft was tested by flexing and extending the knee. Finally, the patellar tendon defect was closed with sutures.
After the operation, the knee was fixed in a brace at 35° of flexion for the first 2 weeks, and patients remained nonweightbearing on crutches. After 2 weeks, the hinges of the brace were adjusted to allow movement from 30° to 60° and weightbearing was gradually increased. Isometric quadriceps muscle exercises were started on the 1st postoperative day, followed later by isotonic quadriceps muscle training. The brace was removed 5 to 7 weeks after the operation. Full weightbearing was allowed when the patient could extend the knee fully. Running was allowed 12 to 16 weeks after the operation, but ball games were not permitted until after 6 months.
Follow-up Evaluation
The clinical follow-up evaluation was performed by one surgeon (TJ) who had not operated on any of the patients in the study. The standard knee ligament evaluation form of the International Knee Documentation Committee (IKDC), 7 the Lysholm 15 (0 to 100 points), and the Marshall 17 (0 to 50 points) knee scores were used. The parameters of the IKDC score include 1) subjective assessment of the knee, 2) knee symptoms (pain, swelling, and partial or full giving way), 3) range of motion (knee flexion and extension measured with a goniometer), 4) stability evaluation (Lachman, anterior drawer, medial and lateral joint opening, and pivot shift tests), 5) evaluation of patellofemoral and tibiofemoral crepitation, 6) presence of anterior knee pain, 7) radiographic evaluations (weightbearing AP, lateral, and patellofemoral projections), and 8) the single-legged hop test for distance (the test was performed three times, averaged, and compared with the results for the opposite limb). According to the IKDC scale, all the parameters were graded as normal (A), nearly normal (B), abnormal (C), or severely abnormal (D), and the first four parameters were included in the final evaluation of the IKDC rating system when comparing the injured and the uninjured knee. In the IKDC system, the lowest grade within a group determines the group grade, and the worst group grade determines the final evaluation.
The knee laxity measurements (AP stability) were made with the KT-1000 arthrometer (MEDmetric Corporation, San Diego, California), as described by Daniel et al., 5 at 30° of knee flexion using a force of 89 N. The laxity was measured twice in the injured and uninjured knees and an average value was recorded, including the side-to-side difference. The result of the test was graded as normal (0 to 2 mm of laxity), nearly normal (3 to 5 mm of laxity), abnormal (6 to 10 mm of laxity), or severely abnormal (>10 mm of laxity).
The isokinetic extension and flexion strength evaluation of the knees was performed with a Cybex 6000 (Cybex International, Inc., Medway, Massachusetts) with the knee angle velocities of 60, 180, and 240 deg/sec, and the interlimb difference was recorded.
The radiographic analysis of the knees was done by one experienced radiologist (TP). The follow-up radiographs of the injured knee were compared with those of the uninjured knee (N = 100) as well as with those of the injured knee taken before the ACL reconstruction (N = 86). Several scoring scales for radiologic evaluation of posttraumatic osteoarthritis of the knee joint are available.9,13,27 For this study, we selected the IKDC evaluation system. 7 A bilateral AP weightbearing radiograph with the knee at 35° to 45° of flexion (tunnel view) was used to evaluate narrowing and other changes in the medial and lateral tibiofemoral joint spaces. The Merchant view 18 with the knee at 45° was used to analyze the medial and lateral facets of the patellofemoral joint. Mild osteoarthritis was defined as minimal radiographic findings (for example, small osteophytes, slight sclerosis or subchondral cysts, or flattening of the femoral condyles) and a patellofemoral joint space wider than 4 mm. Moderate osteoarthritis was defined as the same radiographic findings as well as joint space narrowing (patellofemoral joint space 2 to 4 mm in width). Severe osteoarthritis was defined as radiographic findings plus significant joint space narrowing (joint space of less than 2 mm).
The lateral view of the knee radiographs was used to evaluate the lengths of the patella and the patellar tendon as well as the placement of the graft. Placement of the femoral tunnel was measured on a lateral radiograph from the posterior femoral cortex along Blumensaat's line to the center of the femoral tunnel. The percentage of the entire length of the femoral condyle along Blumensaat's line that this distance represented was recorded. Placement of the tibial tunnel was measured from the anterior corner of the tibial plateau to the center of the tibial tunnel along the tibial plateau, and this distance from the entire length of the tibial plateau was reported as a percentage.
Statistical Analysis
Statistical analysis was performed using the SPSS 7.5 software package (SPSS, Inc., Chicago, Illinois). The calculations between the differences of means were performed with analysis of variance (ANOVA) or paired Student's t-test, and those of the frequencies with the chi-square test. The significance level was set at P < 0.05.
Results
Degenerative Changes in the Patellofemoral and Tibiofemoral Joints
At the follow-up examination, the radiographs showed that 53 patients (53%, 35 men and 18 women) had no signs of patellofemoral osteoarthritis (group I), whereas such changes were seen in the remaining 47 patients (47%). Of these 47 patients, 34 patients (34% of the entire patient population, 24 men and 10 women) had mild degenerative changes (group II), 12 (12%, 11 men and 1 women) had moderate degenerative changes, and 1 woman had severe degenerative changes (moderate and severe changes, group III) (Fig. 1).
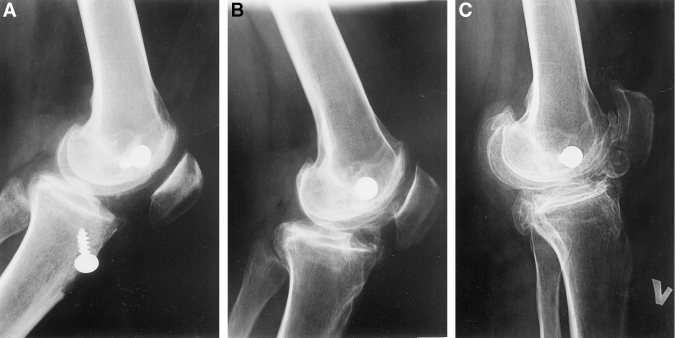
Development of severe patellofemoral osteoarthritis after an ACL reconstruction with a bone-patellar tendon-bone autograft. A, the lateral radiograph just after the reconstruction. B, a lateral radiograph 2 years after surgery. C, a lateral radiograph 9 years after surgery. In this particular case, the femoral tunnel of the graft is clearly too anteriorly placed.
In the lateral tibiofemoral joint, 86 patients (86%) had no degenerative changes, 10 patients (10%) had mild changes, and 4 patients (4%) had moderate degenerative changes. In the medial tibiofemoral joint, the corresponding numbers were 82 (82%), 14 (14%), and 4 (4%).
Shortening of the Patellar Tendon after the ACL Reconstruction and Its Relationship to Patellofemoral Osteoarthritis
The average shortening of the patellar tendon in each group was significantly different from that in the other groups. The patellar tendon was shortest in patients who had moderate or severe osteoarthritis. The average lengthening of the patella (caused by osteophytes) was not significantly different between the groups (Table 1). An example of the shortening of the patellar tendon during the follow-up is shown in Figure 2.
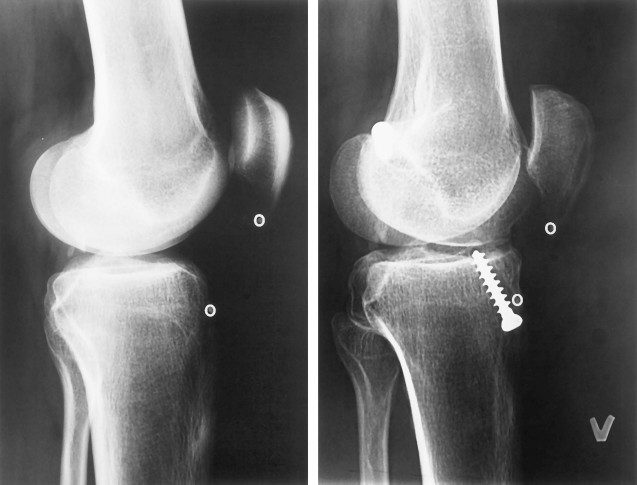
Shortening of the patellar tendon. The patellar tendon has shortened 14.0 mm during the follow-up, as evidenced by comparing the preoperative (A) and follow-up (B) radiographs. The patellar tendon length is measured from the lower pole of the patella to a small depression in the tibia (marked with a circle). In this case, the graft placement is much better than that in Figure 1.
Relationship of Patellofemoral Osteoarthritis 7 Years After ACL Reconstruction to Shortening of the Patellar Tendon, Lengthening of the Patella, and the Insall-Salvati Index (Mean and SD)
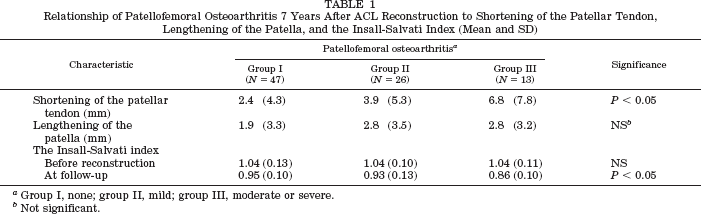
Group I, none; group II, mild; group III, moderate or severe.
Not significant.
The Placement of the Femoral and Tibial Tunnels of the Graft and Its Relationship to Patellofemoral Osteoarthritis
The placement of the femoral tunnel, as measured from the posterior femoral cortex and reported as a percentage of the entire length of the femoral condyle along Blumensaat's line, and placement of the tibial tunnel, as measured from the anterior corner of the tibial plateau and reported as a percentage of the entire length of the tibial plateau, did not correlate significantly with the degree of patellofemoral osteoarthritis (Table 2).
Relationship of Patellofemoral Osteoarthritis 7 Years After an ACL Reconstruction to the Placement of the Femoral and Tibial Tunnels (Mean and SD)
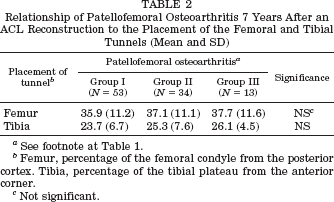
See footnote at Table 1.
Femur, percentage of the femoral condyle from the posterior cortex. Tibia, percentage of the tibial plateau from the anterior corner.
Not significant.
Association between Patellofemoral Osteoarthritis and the Clinical Outcome of the Patients
According to the IKDC rating scale, 13 patients (25%) in group I had normal knees, 34 patients (64%) had nearly normal knees, and 6 patients (11%) had abnormal knees. The corresponding figures were 10 (29%), 16 (47%), and 8 (24%) in group II. In group III there were no normal knees, six (46%) nearly normal knees, five (39%) abnormal knees, and two (15%) severely abnormal knees (the differences in the number of patients in each group with normal, nearly normal, abnormal and severely abnormal knees were significant, P < 0.001).
The results of the functional and clinical Lysholm and Marshall knee scores are shown in Table 3. The best results were in group I and the worst results were in group III. The difference between the groups was significant (P < 0.001).
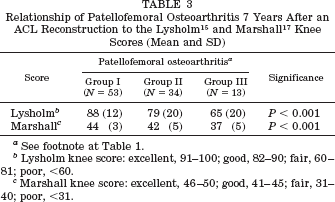
See footnote at Table 1.
Lysholm knee score: excellent, 91–100; good, 82–90; fair, 60–81; poor, <60.
Marshall knee score: excellent, 46–50; good, 41–45; fair, 31–40; poor, <31.
Subjectively, 25 patients (47%) in group I considered their knees normal, 24 (45%) nearly normal, and 4 (8%) abnormal. The corresponding numbers were 14 (41%), 16 (47%), and 4 (12%) in group II, and 1 (8%), 8 (61%), and 4 (31%) in group III (P < 0.05).
The outcome of the objective tests are summarized in Table 4. There were no significant differences between groups except for range of motion and crepitation (P < 0.001). In the isokinetic test of muscle strength, the operated limb of the group I patients showed an average 8% deficit in knee extension at a speed of 60 deg/sec. In knee flexion, there was not any side-to-side difference. At 180 deg/sec, the extension strength deficit was 4%, and, again, the flexion strengths were equal. At 240 deg/sec, the corresponding numbers were 5% and 2%. In group II, these numbers were 8% and 0% at a speed of 60 deg/sec, 3% and 0% at a speed of 180 deg/sec, and 3% and 2% at a speed of 240 deg/sec, respectively. In group III, the similar numbers were 26% and 6% at a speed of 60 deg/sec, 13% and 4% at a speed of 180 deg/sec, and 11% and 2% at a speed of 240 deg/sec, respectively. The group difference was significant in extension at a speed of 60 deg/sec (P < 0.001) and at a speed of 180 deg/sec (P = 0.045).
Results of Objective Follow-up Tests a
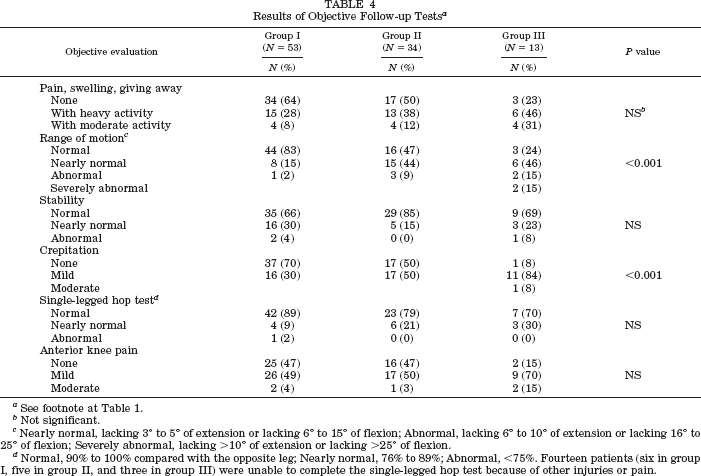
See footnote at Table 1.
Not significant.
Nearly normal, lacking 3° to 5° of extension or lacking 6° to 15° of flexion; Abnormal, lacking 6° to 10° of extension or lacking 16° to 25° of flexion; Severely abnormal, lacking >10° of extension or lacking >25° of flexion.
Normal, 90% to 100% compared with the opposite leg; Nearly normal, 76% to 89%; Abnormal, <75%. Fourteen patients (six in group I, five in group II, and three in group III) were unable to complete the single-legged hop test because of other injuries or pain.
Discussion
Degenerative changes of the patellofemoral joint were very common in the patients we studied an average of 7 years after they underwent ACL reconstruction with the bone-patellar tendon-bone autograft. Almost half of our 100 patients exhibited mild or moderate degenerative changes in the patellofemoral joint, although only 18% of the patients had medial tibiofemoral osteoarthritis and only 14% had lateral tibiofemoral osteoarthritis.
The correlation between patellofemoral osteoarthritis and the presence of patellofemoral crepitation was statistically significant. However, it was somewhat surprising that the correlation between patellofemoral osteoarthritis and anterior knee pain was not significant, although patients with moderate or severe patellofemoral osteoarthritis had worse pain than did the other patients.
Several authors have reported patellofemoral problems, such as crepitation, pain, and limitations in the range of motion of the knee, after an ACL reconstruction.1,2,4,16,23,24 Rosenberg et al. 23 reported that 5 of their 10 patients had abnormal patellar signs seen on radiographic evaluation and that the effect of the procedure on the extensor mechanism of the knee was also significant.
Among our patients, shortening of the patellar tendon seemed to correlate with the severity of the patellofemoral osteoarthritis. Breitfuss et al. 4 observed that shortening of the patellar tendon influences the biomechanics of the patellofemoral joint, although in their study only 10 of the 41 patients (25%) exhibited degenerative changes in the patellofemoral joint at an average of 2 years after the operation. In our study, the Insall-Salvati index 8 was significantly lower among patients with degenerative changes in the patellofemoral joint than in those without such changes (Table 1). Berg et al. 3 recently compared four methods for measuring patellar height and concluded that patellar height ratio changes greater than 0.06 represent a true change in the patellar height. In our study, the changes in the Insall-Salvati index exceeded this value.
Placement of the femoral or tibial tunnel of the graft, as measured on a lateral radiograph, did not correlate significantly with the degree of patellofemoral osteoarthritis in the injured knee. However, the patients with patellofemoral osteoarthritis tended to have more anterior placement of the femoral tunnel and more posterior placement of the tibial tunnel than did the patients without patellofemoral osteoarthritis. If the population of this study had been larger, some statistically significant relationship might have been shown between the placement of the graft and the occurrence of patellofemoral osteoarthritis. Khalfayan et al. 14 reported that the optimal placement of the femoral tunnel, as viewed on a lateral radiograph, should be more than 60% along Blumensaat's line from anterior to posterior (that is, less than 40% in our measurement). The optimal placement of the tibial tunnel should be more than 20% along the tibial plateau, as measured in an anterior-to-posterior direction, according to Khalfayan et al. 14 In our study, the average placement of the femoral and tibial tunnels of the graft was within these limits in every group (Table 2).
The Lysholm 15 and Marshall 17 knee scores were significantly lower in our patients who had patellofemoral osteoarthritis than in patients without it. Similar results were found in the final evaluation of the IKDC rating scale. The patients free of patellofemoral osteoarthritis were subjectively more often satisfied with the operated knee and had less pain and swelling in the knee joint than the patients with patellofemoral osteoarthritis. Also, the range of motion of the knee was significantly better among patients free of patellofemoral osteoarthritis than in those with this condition. Neither the ability to perform the single-legged hop test nor the ligamentous stability of the knee correlated with the presence of patellofemoral osteoarthritis; however, only three of our patients had an unstable knee.
In our study, results of isokinetic testing showed an average quadriceps muscle strength deficit of 26% at the speed of 60 deg/sec in patients with moderate or severe patellofemoral osteoarthritis; this deficit was significantly lower (8%) among patients in the other two groups. Rosenberg et al. 23 reported an average quadriceps muscle strength deficit of 18% in patients who had undergone ACL reconstruction, but they did not correlate the findings with the occurrence of patellofemoral osteoarthritis.
Our study had some limitations. First, this was a retrospective study without any control group. Therefore, we do not know whether the primary injury itself, in addition to the surgical procedure, had some effect on the development of the patellofemoral osteoarthritis. Second, the reconstruction was done with a miniarthrotomy technique and a large notchplasty, which may also have contributed to the osteoarthritic process. The surgical technique we currently use is an arthroscopic ACL reconstruction without the large notchplasty. We have also abandoned the use of braced immobilization after ACL reconstruction. The coming years will show whether these changes in our treatment protocol can reduce the rate and incidence of the development of patellofemoral osteoarthritis after ACL reconstruction.
In summary, the results of our long-term follow-up study showed that, after an ACL reconstruction with a bone-patellar tendon-bone autograft using a miniarthrotomy technique, patellofemoral osteoarthritis occurs frequently and has a clear association with the clinical outcome of the patient. The shortening of the patellar tendon correlates with the severity of the patellofemoral osteoarthritis so that the greatest shortening is seen among patients with the most severe osteoarthritic changes. However, osteoarthritis has many causes, and, therefore, further studies are needed to verify our finding related to shortening of the patellar tendon and to clarify the main determinants of the shortening.