
Abstract
To determine the relationship between previous lower-limb loading and current self-reported hip and knee disability, we sent a questionnaire to 1321 former elite male athletes who had represented Finland between 1920 and 1965 in international competitions and to 814 control subjects who had been classified as healthy at the age of 20. After adjustment for age, body mass index, and occupational group, the odds ratios of hip disability in the athletes compared with control subjects were 0.35 in endurance athletes (95% confidence interval, 0.14 to 0.85, P 0.02), 0.56 in team sport athletes (0.28 to 1.10, P 0.09), 0.30 in track and field athletes (0.12 to 0.73, P 0.01), 0.84 in power sport athletes (0.51 to 1.39, P 0.49), 0.30 in shooters (0.07 to 1.32, P 0.11), and 0.54 (0.36 to 0.82, P 0.01) in all athletes combined. Compared with control subjects, only team sport athletes had a higher risk of knee disability (odds ratio, 1.76; 95% confidence interval, 1.03 to 3.02; P 0.04). Even though athletes have been reported to be at an increased risk for lower-limb osteoarthritis, our data show that former elite male endurance and track and field athletes and all athletes combined reported less hip disability than the control subjects. The effect of vigorous athletic activity on the function of knee joints is more controversial, because sports that involve a high risk of knee injury are likely to lead to pain, disability, and osteoarthritis.
The proportion of elderly people in the population is increasing rapidly, and the relationship between physical activity and a disability-free life is highly relevant for public health. Lifelong physical activity reduces the risk of several major chronic diseases, such as coronary heart disease and non-insulin-dependent diabetes mellitus. In contrast, sports-related joint loading13,18,26 and strenuous occupational loading3,27 have been shown to increase the risk of hip or knee osteoarthritis. Lower-limb injuries, such as knee and ankle sprains in soccer, accelerate the development of osteoarthritis. However, our knowledge of the role of sports-related activity in youth in lower-limb function in old age is limited.
Musculoskeletal disability decreases quality of life. In a previous study from our institution, we found that former elite athletes with knee osteoarthritis were more likely to report knee pain and disability than were athletes without knee osteoarthritis. 12 On the other hand, physical activity helps maintain good lower-limb function, which is an important factor for independent living in old age. Among 75-year-old men and women, good maximal strength levels have been positively associated with mobility. 22 Furthermore, aerobic or resistance exercise has been reported to reduce knee pain and disability, 6 and good lower-limb muscle function among former elite athletes, even among those with hip or knee osteoarthritis, has been reported. 11 Thus, different types of exercise-related physical loading during adolescence and adulthood may increase the risk for lower-limb osteoarthritis, but the same activity may also have a favorable effect on mobility and may delay the onset of physical disability. The purpose of this paper was to investigate the association between participation in different types of sports during adolescence and adulthood and self-reported lower-limb pain and disability in older men. These findings are compared with those for a control group whose subjects were reported to be healthy at the age of 20.
Materials and Methods
Subjects
We identified male athletes who had participated at least once in the Olympic Games, World or European championships, or international competitions (athletic contests between two or more countries) between 1920 and 1965. Control subjects were selected among Finnish men who had been found to be completely healthy at the time of their military induction physicals (age, 20 years old). 24 In earlier investigations of the various health effects of different types of athletic activity the athletes were grouped according to the type of training needed to achieve maximal results, that is, principally aerobic training, principally anaerobic training, or mixed training.14,15,24 In the present study we followed the same classification system, but athletes with mixed training were further classified into two subgroups according to the risk of injury to the lower-limb joints. Thus, endurance athletes (long-distance runners, cross-country skiers) are those who experience a high amount of repetitive loading of the weightbearing joints; power sport athletes (boxers, wrestlers, weight lifters, throwers) are exposed to fewer repetitions but higher forces when loading the joints; track and field athletes (jumpers, sprinters, hurdlers, middle-distance runners, decathlon athletes) are at a greater risk of high-impact loads but at a lesser risk of joint sprains; team sport athletes (soccer, ice hockey, and basketball players) include those with a greater risk of high-impact loads and sprains of the joints; and shooters take light-to-moderate general exercise involving some kneeling and squatting. Because, among the power sports group, in particular, there is variation in loading patterns, some stratified data are also given for each sport event.
The 1995 Questionnaire
In 1995, a questionnaire was mailed to the cohort of surviving former athletes (N = 1321) and control subjects (N = 814). The response rate was 75.0% (991) for the athletes and 70.9% (577) for the control subjects. The questionnaire included items on physician-diagnosed hip or knee osteoarthritis (yes/no), separately for onset before and after the age of 45 years. Information was also elicited on physician-diagnosed knee ligament injuries, knee meniscal injuries, and the need of hospital admission for knee injury. Table 1 shows the characteristics of the study subjects. Body mass index was calculated based on self-reported weight and height.
Characteristics of the Study Subjects a
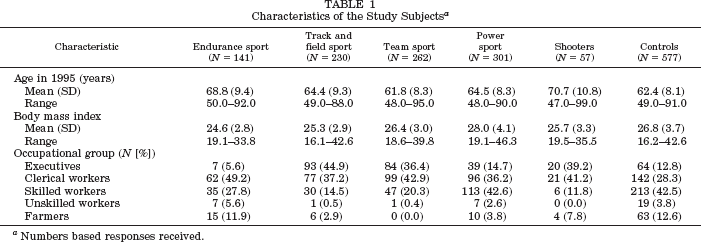
Numbers based responses received.
Occupational groups were classified into the following categories: executives, clerical workers, skilled workers, unskilled workers, and farmers. 24 Each person was classified into the group in which he had been occupationally active the longest (Table 1). The category “executives” was used as a reference group when analyzing the association between occupational group and disability.
Occurrence of joint pain during the previous year and the occurrence of disability was determined separately for the hips and knees. Those who reported having hip or knee pain at least once per month were classified as having monthly hip or knee pain. Hip and knee disability was scored depending on whether the subjects reported pain or disability (yes = 1, no = 0) during 1) nocturnal bedrest, 2) more than 5 minutes in the morning after getting of bed, 3) sitting for 30 minutes, 4) full support by the legs, 5) walking more than 100 meters, 6) going up or down stairs, and 7) squatting or bending forward. The sum of positive responses (0 to 7) was calculated and subjects who scored at least 3 points for either the hip or knee were considered to have hip or knee disability.
Statistical Analyses
The statistical analyses were performed using BMDP Statistical software (SPSS Inc., Chicago, Illinois). We used stepwise logistic regression models to analyze the association between different covariates and hip and knee osteoarthritis, pain, and disability. Odds ratios computed from the logistic regression model were used to evaluate the strength of the association.
Results
As expected, the risk for either hip or knee disability was higher among older subjects than younger subjects, and subjects with a high body mass index had higher risk for both hip and knee disability than subjects with low body mass index (Table 2). Moreover, occupational group was associated with the risk of either hip or knee disability (Table 2). Subjects with knee ligament or meniscal injury reported more knee disability (29.5%; 95% confidence interval [CI], 24.5% to 34.6%) than subjects without injury (7.7%; 6.0% to 9.6%) (P < 0.0001).
Odds Ratios (OR) and 95% Confidence Intervals (CI) for Hip and Knee Disability Among Subjects Who Completed the 1995 Questionnaire a
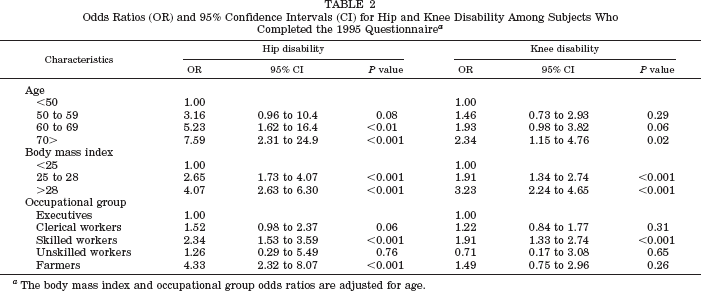
The body mass index and occupational group odds ratios are adjusted for age.
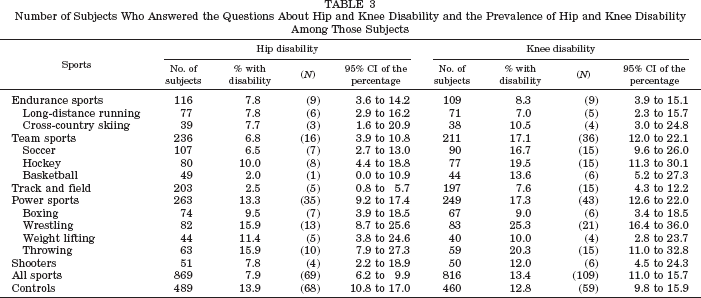
Table 3 shows the number of subjects who answered the questions about hip and knee disability and the prevalence of hip or knee disability among those subjects. Based on the questionnaire, the age-adjusted risk of hip disability was lower among endurance, team sport, and track and field athletes, and also among all athletes combined (Table 4) when compared with control subjects. Additionally, the age-adjusted odds ratio of at least monthly hip pain was lower among endurance, team sport, track and field athletes, shooters, and all athletes when compared with control subjects (Table 5). Compared with control subjects, the risk of hip disability among endurance, track and field athletes, and all athletes combined (Table 4), and hip pain among endurance athletes, shooters, and all athletes combined (Table 5) was still lower after adjustment for age, occupational group, and body mass index. The risk of knee disability (Table 4) and pain (Table 5) was similar in athletes and control subjects except for those who competed in the team sports in which there was an increased likelihood of knee disability and pain. Figure 1 shows the age-adjusted risk of having hip or knee disability by various sports events compared with control subjects.
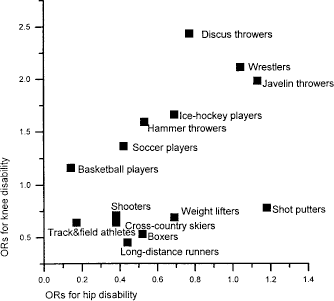
Age-adjusted odds ratios (OR) of hip and knee disability among various sport events for elite former male athletes compared with control subjects.
Number of Subjects Who Answered the Questions About Hip and Knee Disability and the Prevalence of Hip and Knee Disability Among Those Subjects
Adjusted Odds Ratios for Hip (N = 1358) and Knee (N = 1276) Disability in Subjects Who Completed the 1995 Questionnaire
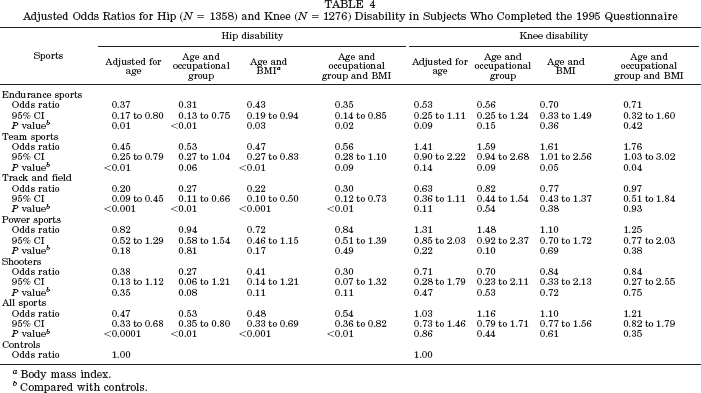
Body mass index.
Compared with controls.
Adjusted Odds Ratios (OR) and 95% Confidence Intervals (CI) for Hip and Knee Osteoarthritis and Pain Among Former Athletes and Control Subjects
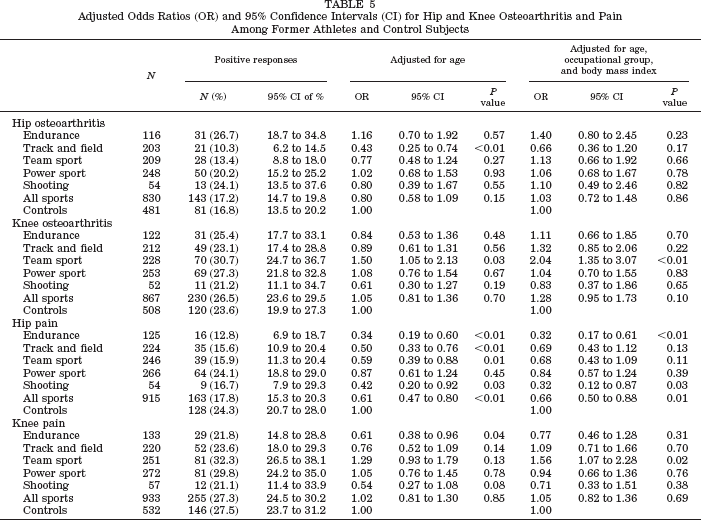
There was no difference in the risk of physician-diagnosed hip osteoarthritis between athletes and control subjects when the results were adjusted for age, body mass index, and occupational group (Table 5). Team sport athletes had a higher risk for knee osteoarthritis after adjustment for age, body mass index, and occupational group (Table 5). Moreover, compared with control subjects, the age-adjusted risk for physician-diagnosed knee osteoarthritis (N = 73) before the age of 45 was significantly higher among team sport athletes (odds ratio, 2.92; 95% CI, 1.49 to 5.73; P < 0.01) and power sport athletes (odds ratio, 2.13; 95% CI, 1.06 to 4.29; P = 0.03). The covariate-adjusted risk of knee osteoarthritis before the age of 45 was particularly high among team sport athletes (odds ratio, 3.38; 95% CI, 1.55 to 7.37; P < 0.01). When the sports groups were combined, all athletes had higher age-adjusted risk for physician-diagnosed knee osteoarthritis (odds ratio, 1.98; 95% CI, 1.06 to 3.69; P = 0.03) before the age of 45 when compared with control subjects. The risk of hip osteoarthritis (N = 27) before age 45 among athletes and control subjects was similar.
Physician-diagnosed knee ligament injuries were rare among long-distance runners (7%, 5 of 73), shooters (9%, 4 of 47), and control subjects (11%, 51 of 473) but were common among soccer players (41%, 38 of 92), wrestlers (30%, 25 of 84), and throwers (26%, 15 of 57) (P < 0.0001, for group differences). Fifteen percent of shooters (7 of 48) and control subjects (76 of 492) reported physician-diagnosed knee meniscal injuries, but the proportion of meniscal injuries was high among soccer players (45%, 48 of 107), wrestlers (33%, 28 of 84), and throwers (31%, 18 of 59) (P < 0.0001). Moreover, 52% (61 of 118) of soccer players reported that they had needed hospital treatment for knee injuries.
Discussion
Age is a major factor in determining the risk of hip or knee disability, followed by body mass index and occupational group. Because of this, we used these as covariates when analyzing the risk of hip or knee disability among former elite athletes. Using the covariate-adjusted method, our endurance athletes, track and field athletes, power sport athletes, and shooters did not report more hip or knee disability than did our control subjects. The covariate-adjusted odds ratios of hip disability were lower among endurance, track and field, and all athletes combined. On the other hand, team sport athletes had a slightly higher odds ratio for knee disability when compared with control subjects.
Investigations to record lifetime physical loading generally encounter difficulties. These problems can be reduced by studying former elite athletes, because their loading patterns are rather specific, they follow well-planned and defined training routines, and their exercise histories are more reliable than are those obtained from someone who has exercised only recreationally.
Our cohort included elite athletes, who were a selected group in many ways. First, various selective factors, such as muscle fiber composition, play a role in enabling some athletes to reach top levels in competitions. Second, the athletes were presumably free from hip or knee osteoarthritis at the time they participated in top-level sports, where good lower-limb function is a prerequisite. Thus, subjects with sports-related injuries during their early athletic career are likely to be dropouts. In this respect, our results may underestimate the harmful effects of athletic loading on lower limbs.
Our athletes had represented Finland on an international level at least once between 1920 and 1965. In 1985, a questionnaire was given to our subjects to obtain historical data mainly for follow-up studies. 24 Of the subjects who were still competing in 1985, only 9% reported having knee disability in 1995. The reported rate of hip disability among those athletes was 4%. Among the subjects who reported that they had never participated in competitive sports, the reported rate for knee disability was 13.0% and for hip disability was 13.8%. The most important reasons for ending a sports career were age (31.4%), lack of interest (22.9%), and injuries (20.0%).
Several methods have been used to measure pain4,10,17 and disability5,8,21 among osteoarthritic subjects. However, there is no general agreement on how to measure disability in epidemiologic studies. We measured hip disability and knee disability with questions on activities that both former athletes and control subjects do in their daily life. The subjects who scored at least three points of seven for either hip or knee disability were classified as having hip or knee disability. We calculated both hip disability and knee disability using different cut points, but the results of those calculations were similar. Moreover, a significant association between our disability score and radiographic knee osteoarthritis 12 and jumping height 11 has been shown.
Strenuous occupational loading predisposes people to lower-limb osteoarthritis. Therefore, we calculated each subject's work years in terms of various work-related physical loading. Only 6.5% of executives compared with 68.9% of unskilled workers had spent at least 10 years in heavy work. Because the occurrence of osteoarthritis-related disability may affect the ability to continue heavy work and because we found associations between work-related loading and occupational group, we used occupational group as a covariate when analyzing the association between athletic activity and hip or knee disability.
Despite the reported relationship between running and radiographic hip osteoarthritis, 20 former athletes’ joints may show radiographic osteoarthritic changes without loss of function. 1 Moreover, the odds ratios of hip pain and disability were low among our endurance athletes. Low development of disability among older runners who had engaged in running and other aerobic activities has been reported; this association is probably related to increased aerobic capacity, strength, fitness, and increased organ reserve rather than to the effects of postponed osteoarthritis development. 7 Also, lower body mass index in endurance athletes may prevent the occurrence of hip problems, especially in walking and going up or down stairs. Lysholm and Wiklander 19 reported that active long-distance runners have hip problems, but in old age these problems do not result in more years with hip pain and disability. Likewise, we did not find any evidence that repetitive loading with low injury risk during adolescence and adulthood has harmful effects on knee joint function at older ages.
Kujala and coworkers 13 concluded that mixed sport and power sport athletes need more hospital care than control subjects because of premature osteoarthritis of the hip, knee, or ankle; however, in endurance athletes the admissions are at an older age than in control subjects. They also pointed out that in only the most severe cases did patients need hospital treatment. We used the same subjects in this study as those in the Kujala et al. study and our team sport athletes had high odds ratios for knee osteoarthritis. Knee injuries were common, especially among soccer players. Previous knee injuries are risk factors for knee osteoarthritis.2,9,12,25 Thus it seems that the increased risk of knee osteoarthritis among team sport athletes is explained in part by knee injuries. One limitation of our study is the diagnosis of osteoarthritis. We used physician-diagnosed osteoarthritis, and it is possible that some subjects with knee injury and knee pain were falsely classified as having osteoarthritis based on clinical pain without radiographic confirmation.
Nevertheless, participation in mixed training has a favorable effect on lower-limb muscle function.11,16 McAlindon and coworkers 21 concluded that quadriceps muscle strength is a more important determinant of functional impairment in elderly subjects than the severity of knee osteoarthritis as assessed radiographically. However, knee injuries are probably etiologically related to knee osteoarthritis, and the risk for knee disability was high among team sport athletes. Therefore, knee injury prevention and effective treatment of such injuries are important for the prevention of injury-related knee disability. Furthermore, our study is in agreement with earlier observations that lower-limb pain and disability are more commonly attributed to knee rather than hip problems. 23
Heavy weight training and high body mass index among power sport athletes may predispose them to knee osteoarthritis. Subjects with a high body mass index had higher odds ratios for hip and knee disability than subjects with a low body mass index. In our previous study, 12 high body mass index at age 20 explained some of the increased knee osteoarthritis risk among former elite weight lifters. Our power sport athletes had a high age-adjusted odds ratio for knee osteoarthritis before the age of 45. Thus, the low odds ratio for hip or knee disability among weight lifters was an unexpected finding. Possibly, lower-limb joint loading in the physiologic flexion-extension direction is less harmful for joint function than the type of knee loading encountered in team sports, throwing, and wrestling. The tendency toward increased odds ratios for hip and knee disability among javelin throwers and wrestlers (Fig. 1) may be explained by nonphysiologic rotational or mediolateral loading and injuries among these athletes. Even though the original cohort included all Finnish male former elite athletes, the number of subjects in each sport group was low. The limited number of subjects in those groups did not allow sufficient statistical power for studying the risk for hip or knee disability among subjects with or without reported hip or knee injury. Moreover, when using a retrospective study design the subjects with disability may remember their injuries better than subjects without disability, and this may overrate the role of injury as a risk factor for disability.
Despite the reported relationship between long-term vigorous physical activity and radiographic lower-limb osteoarthritis, little is known about the effects of physical activity on lower-limb function. Low aerobic work capacity and lower-limb muscle weakness are associated with disability, and so aerobic or resistance exercise programs have been recommended to reduce self-reported disability and pain among subjects with knee osteoarthritis. 6 Ettinger and coworkers 6 have also pointed out that long-term compliance with exercise regimens is possibly more important than the type of therapy or training to reduce pain and disability. Our former athletes are a selected group and therefore our results cannot be generalized widely. However, our results are consistent with the recommendation that leisure physical activity, especially aerobic training with low risk of injury, has favorable effects on mobility and health.
In conclusion, despite reports of the role of leisure-time physical activity as a risk factor for lower-limb osteoarthritis, former elite male endurance and track and field athletes and all athletes combined reported less hip disability than did their control subjects. The role of vigorous athletic activity for the function of knee joints is more controversial, because sports that involve a high risk of knee injury are likely to lead to pain, disability, and osteoarthritis. Therefore, our results support the thesis that aerobic activity, especially with its many health benefits and low risk of injury, can be recommended to maintain health and a disability-free life in old age.