
Abstract
A retrospective review was performed of records for players who suffered fractures about the orbit during participation in officially sponsored activities of the National Football League from 1980 to 1997. Clinical information was obtained on 19 of 29 players who sustained orbital fractures. The most common signs and symptoms included decreased visual acuity (74%, 14), decreased eye movement (42%, 8), hyphema (37%, 7), and infraorbital numbness (21%, 4). The mechanisms of injury were a digital poke (74%, 14) and blunt facial trauma (26%, 5). There were significantly more orbital fractures than zygomatic fractures suffered by offensive linemen as compared with all other positions. Fifteen of 19 players were managed with surgical reconstruction; 4 players were treated nonoperatively. The mean time from injury to surgical procedure was 7.7 days (range, 0 to 42). The mean interval to follow-up was 45.6 months (range, 3 to 146). At follow-up examination, eight (53%) of the patients treated surgically still reported diplopia with upper field gaze. Three of the four patients treated nonoperatively were asymptomatic. The mean time lost from games or practice was 25 days (range, 5 to 56). Ultimately, 17 (89%) players with orbital fractures were able to return to full football activities. Two patients were unable to resume their careers because of residual visual impairment.
The majority of facial injuries in National Football League (NFL) players are relatively minor, consisting of lacerations, contusions, and abrasions. Occasionally, players will suffer facial fractures from blunt trauma during play or practice. However, more serious injuries, including fractures of the zygoma and orbit, may result in more functional disability for affected players.
Orbital fractures are categorized into two groups, orbital rim and orbital wall fractures. Orbital rim fractures are generally caused by a direct blow.3,6 In contrast, orbital wall fractures are usually caused by a trauma to the eye (globe). Limited eye movement and diplopia (double vision) may occur after this injury, despite the administration of appropriate operative or nonoperative treatment. The occurrence, management, and clinical outcome of orbital fractures in a group of high-level competitive athletes have not previously been documented. The purpose of this study was to examine the demographic data, clinical signs and symptoms, treatment, and outcome of NFL players who sustained fractures about the orbit.
Materials and Methods
A retrospective review was performed on records of NFL players who sustained fractures about the orbit while participating in officially sponsored NFL games or practices from 1980 to 1997. Athletes who experienced fractures of the orbit, the zygoma, the sinus cavities, or a combination thereof were anonymously identified by a review of the Med Sports Systems Limited (MSS) database (Iowa City, Iowa). Demographic data including year of injury, mechanism of injury, player position, clinical management, and playing time lost, were obtained from the MSS database.
Questionnaires were then sent to physicians and trainers of all 30 NFL teams requesting further information regarding clinical outcomes of these injuries. Only the initials of the players included in the study were used, to maintain confidentiality. Information recorded from each team included the player's age at the time of injury, the year of injury, position played, mechanism of injury, fracture type, initial clinical findings, mode of treatment, time from injury to surgical procedure, type of operation (if applicable), practices and games missed, and results of the most recent clinical follow-up.
Results
We found that 41 facial fractures were sustained by 41 athletes who played in the seasons between 1980 and 1997. There were 29 orbital fractures and 12 fractures of the zygomatic arch without orbital injury. The average annual occurrence of all facial fractures during this time period was 2.3 injuries per year (range, 0 injuries in 1990 and 1992 to 5 injuries in 1995). Twenty-five of the 30 NFL teams responded to the survey and provided clinical information on 19 of the 29 players with orbital fractures, who were from 15 teams.
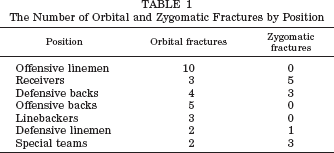
The most common clinical signs and symptoms immediately after orbital fracture were decreased visual acuity (14 of 19 players, 74%), decreased eye movement (8 players, 42%), hyphema (7 players, 37%), and infraorbital numbness (4 players, 21%). The most common mechanism of injury was a digital poke to the eye (14 players, 74%); the other five athletes experienced blunt trauma. There were significantly more orbital fractures than zygomatic fractures sustained by offensive linemen as compared with injuries to players in all other positions (P = 0.02, Fisher's exact test) (Table 1).
The Number of Orbital and Zygomatic Fractures by Position
Four of the 19 players with orbital fractures were treated nonoperatively, and 15 were treated with surgical reconstruction of the orbit (open reduction and internal fixation). The mean time from the injury to the operation was 7.7 days (range, 0 to 42). Autogenous bone graft, synthetic mesh, or silicone implants were used in some patients to provide structural support to the globe.
The mean interval from injury to follow-up was 45.6 months (range, 3 to 146). Range of eye movement and visual acuity improved in patients treated operatively and in those treated nonoperatively. Fourteen of the 15 patients (93%) treated surgically reported diplopia preoperatively, compared with 2 of 4 patients who were treated nonoperatively. At follow-up examination, 8 of the 15 patients who were treated surgically (53%) still reported diplopia with upper field gaze, whereas 3 of the 4 patients treated nonoperatively (75%) were asymptomatic at follow-up. One player, a wide receiver who was treated nonoperatively, experienced visual dysfunction with lateral gaze that resolved within 1 year. The mean duration of time lost from games or practice because of injury was 25 days (range, 5 to 56). Ultimately, 17 players with orbital fractures (89%) were able to return to full football activities. The players who were able to return to play with diplopia (upper field gaze) were offensive linemen, including the tight end position.
Two patients who underwent operative treatment for an orbital fracture sustained after a digital poke were unable to resume their careers. One was a 34-year-old offensive lineman who sustained an orbital fracture and a ruptured globe; he was left with permanent visual impairment. The second patient was a 28-year-old linebacker who returned to play for 1 month before he chose to retire; he also continued to have visual impairment at the time of his most recent follow-up examination.
A 31-year-old offensive lineman who sustained an orbital blow-out fracture from a digital poke returned to play after a 2-year hiatus from professional football. At the time of writing this article, this patient remained under the care of the senior author (RFW). The patient has undergone three procedures: one open reduction and internal fixation and two procedures for lysis of adhesions. His vision has improved, although he still has residual upper-field diplopia; he has functioned effectively despite the persistence of the visual field abnormality.
Discussion
The optimal management of orbital fractures remains unclear. Although there are numerous reports of retrospective studies on the results of both operative and nonoperative management of these injuries, no published study has addressed the outcome of these injuries in high-level athletes.1–8,11 From our data, it appears that orbital fractures occur at an average of twice per year in the NFL. Our findings suggest that, despite early surgical intervention, diplopia remained in more than half of the 19 athletes who were available for follow-up examination. However, despite the persistence of some visual impairment, 17 of the 19 affected athletes (89%) were ultimately able to return to play.
The term “blow-out” fracture was described by Smith and Regan 10 in 1957. Orbital blow-out fractures occur as a result of direct trauma to the eye. The eye is compressed, but the globe usually does not rupture. As the eye globe is compressed, the intraocular pressure increases, and the weakest area of the orbit, the posteromedial floor, gives way, leading to an orbital wall fracture (Fig. 1). 5 Soft tissues may herniate into the fracture site. These structures can include the fibrous connective tissue septa between the periosteum and muscle, orbital fat, or the inferior rectus muscle. 5
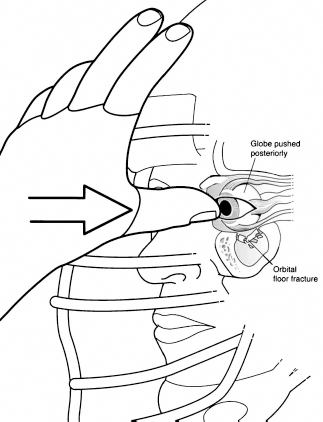
Mechanism of orbital fracture (“blowout” fracture) associated with a direct blow to the eye globe.
All patients suspected of having sustained a blow-out fracture should be thoroughly evaluated. The history should include the mechanism of injury, whether there was an associated loss of consciousness, any change in visual status, and an assessment of the intensity and location of pain. The physical examination should evaluate for findings specific for orbital blow-out fractures, such as diplopia, limitation of upward gaze, enophthalmos (backward displacement of the globe into the orbit), infraorbital nerve dysfunction, and a palpable deformity of the infraorbital rim. 5 Nonspecific signs include subconjunctival hemorrhage, eyelid edema, and hemorrhage. Computed tomography is the diagnostic imaging modality of choice to confirm the presence of the blow-out fracture and to define the pathoanatomy of the injury. Patients with suspected blow-out fractures should be imaged promptly and referred to an appropriate physician. 9
The appropriate treatment for blow-out fractures remains controversial. When there is no functional or cosmetic impairment, nonoperative treatment is appropriate. 8 Indications for early surgical repair include inferior rectus muscle entrapment, a large-sized fracture, and globe malposition. 5 Enophthalmos is also an indication for early surgical repair because late repair of this defect is technically difficult after fibrous scar formation takes place. 5 Surgical intervention is generally indicated within the 1st week after injury if any of these conditions are present. In many cases it is appropriate to allow the early hemorrhage and edema to resolve. During the initial nonoperative treatment, the patient is prescribed oral antibiotics and cool compresses. Oral corticosteroids are used to accelerate the resolution of edema. Subsequently, surgical intervention is appropriate if diplopia persists. 11 Surgery has been shown to lead to satisfactory results2,4,7; however, one study found persistent diplopia after surgical reconstruction in 37% of 54 patients. 1 We found that 53% of the 15 patients who were treated surgically had persistent diplopia with upper-field gaze, perhaps because they had particularly severe injuries.
We found that the average annual occurrence of orbital blow-out fractures was less than two per year in the NFL during the 18 years studied. The rate of injury was relatively stable, despite an increase in the number of NFL players because of league expansion. In our series, the players who underwent a surgical procedure had a higher incidence of persistent diplopia and of inability to return to play. This is likely because players who were treated nonoperatively had injuries that were less severe. Orbital blow-out fractures were most common in offensive linemen (10 of the 29 fractures), perhaps because of the techniques used by defensive linemen to avoid blocks, which can often involve accidental digital pokes to the facial area of the opposing player.
The main limitation of this study is that data collection was retrospective and there was incomplete follow-up. Although the NFL collects data in an organized and complete manner, it is possible that some facial fractures may have been omitted from the database.
Our results indicate that the average annual occurrence of orbital fractures in professional American football players is relatively low. Although it appears that visual disturbances are commonly associated with orbital fractures, persistent diplopia does not preclude a return to sport in the majority of affected players. In other cases, however, this visual disturbance can cause the end of a career. Certain NFL players have been wearing protective eye shields in recent years. Although we are not aware of any studies documenting the efficacy of these eye shields, we believe that players should consider using them on a routine basis to avoid this rare, but potentially devastating, injury.