
Abstract
We compared anterior cruciate ligament function in skeletally mature patients after treatment of tibial eminence fractures with that of patients in two other groups: patients who had anterior cruciate ligament deficiency and patients who had undergone anterior cruciate ligament reconstruction using bone-patellar tendon-bone autografts. The Lysholm questionnaire was used to evaluate symptoms and KT-1000 arthrometry was used to determine objective knee laxity at an average follow-up of 5.2 years. Knee joint proprioception was assessed with a new method designed to test joint position sense. The Lysholm score for the tibial eminence group was 94 7. Only the patients in the anterior cruciate ligament-deficient group demonstrated statistically significantly increased laxity and inferior proprioception when the injured leg was compared with the uninjured leg. Both laxity and proprioception were statistically inferior for the anterior cruciate ligament-deficient group when compared with both the treated tibial eminence fracture group and the anterior cruciate ligament-reconstructed group. No statistically significant difference was observed between the anterior cruciate ligament-reconstructed and treated tibial eminence fracture groups. Correlation was observed between laxity and proprioception when all patients were analyzed. The results demonstrate that appropriate treatment of tibial eminence fractures restores stability and proprioception to the knee.
Tibial eminence fractures result from extreme ACL tension that causes tibial bone avulsion rather than ACL substance rupture. These fractures functionally disrupt the ACL complex and may cause knee instability. Furthermore, the intraarticular fragment may cause mechanical blocking to knee flexion-extension and joint surface incongruity if the fracture extends into the tibial plateau articular surface. These injuries are most often reported in children, in whom immature growth plates are responsible for the relative bony weakness. These injuries do occur in adults, however, and with significant incidence.8,12,22
Most authors believe that tibial spine fractures are more common in children than in adults,27,29,38 and several studies have reported on tibial eminence fractures in children only.9,21,25 Biomechanical studies have demonstrated that ligament failure characteristics are influenced by overall age and skeletal maturity.36,37 Results of clinical studies have also suggested that the pathologic condition and outcome of tibial eminence fractures are different for skeletally mature patients than they are for those who are skeletally immature.12,24,27,35 Noyes et al. 28 demonstrated that a significant amount of plastic deformation of the ligament occurs before failure. Despite successful healing of the eminence fragment, the ACL may therefore be functionally incompetent, with resulting knee instability. A preferred treatment option may then be ACL reconstruction. Evidence now suggests that the ACL has proprioceptive properties that assist in the neuromuscular control of the knee.5–7,13,14,18 Therefore, these properties may be preserved with fixation of tibial eminence fractures.
This study was undertaken to evaluate the function of the ACL after the treatment of tibial eminence fractures in skeletally mature patients. The evaluation of ACL function focused on quantitated symptoms, objective knee stability, and knee joint proprioception. For comparison, groups of ACL-deficient and ACL-reconstructed patients were also evaluated.
Materials and Methods
Ten skeletally mature patients with tibial eminence fractures were treated at our institution during a 5-year period from 1992 to 1997; information about them is summarized in Table 1. The group consisted of five men and five women with an average age of 34.5 years (range, 15 to 66). The mechanism of injury was a noncontact twisting of the knee except in one patient who was a passenger in a motor vehicle accident. All patients developed an acute hemarthrosis at the time of injury. Plain radiographs were used to classify the fractures according to Meyers and McKeever, 26 and mature growth plates were observed in all patients.
Description of Patients Treated for Tibial Eminence Fractures
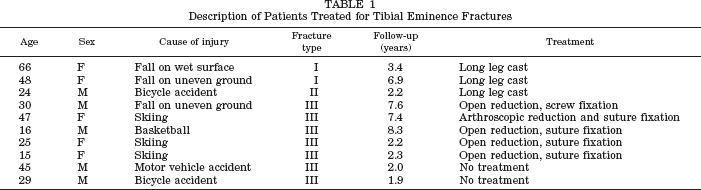
The two patients with type I fractures (Fig. 1) were treated with closed reduction and immobilization for 4 to 6 weeks in a long leg cast with the knee in full extension. This was followed by physical therapy to increase range of motion and strengthen the quadriceps muscles. One patient with a type II fracture was treated by closed reduction and immobilization for 4 to 6 weeks followed by physical therapy. One patient with a type III fracture was treated with open reduction and screw fixation similar to the procedure described by Keys and Walter. 15 A 5-cm incision adjacent to the medial aspect of the patellar tendon was created. The fragment was reduced using an awl, and a 4.5-mm cortical screw was placed just anterior to the ACL. Three patients with type III fractures were treated with open reduction and suture fixation. A 5-cm incision was made just medial to the patellar tendon. Two drill holes were made through the anterior tibia and into the reduced fragment adjacent to the ACL insertion. Non-absorbable sutures were passed through the drill holes and through the substance of the ACL and then tied over the anterior cortex of the tibia. One patient underwent arthroscopic reduction and suture fixation. An ACL guide was used to reduce the fragment, and drill holes were made through the anterior cortex into the fracture fragment adjacent to the ACL. A nonabsorbable suture was passed through the drill holes and through the ACL arthroscopically, using suture-passing techniques, and then tied over the anterior tibia. Postoperatively, patients treated with arthroscopic reduction and suture fixation had their knee immobilized for 2 to 3 weeks. Immobilization was followed by physical therapy to increase range of motion and strengthen the quadriceps and hamstring muscles. The average time for patients with displaced eminence fractures to return to their preinjury level of activity, including sports, was 4 months.
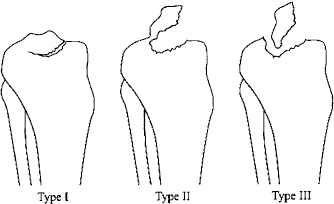
Classification of tibial eminence fractures. Type I, minimal displacement; Type II, hinged posteriorly; Type III, complete separation. (Modified from Meyers and McKeever. 27 )
Two patients with untreated type III fractures were seen more than 1 year after injury with complaints of knee instability. They each had radiographic evidence of tibial spine fracture nonunion, demonstrated by clear separation between the fragment and its bed on the tibia. These patients were evaluated separately from the group whose tibial eminence fractures had been successfully treated.
At follow-up, the Lysholm knee scoring system, which emphasizes knee stability, was used to assess symptoms. 20 Objective laxity was determined by arthrometry, with side-to-side differences obtained with 15, 20, and 30 pounds of force (KT-1000 arthrometer, MEDmetric Corp., San Diego, California).
Proprioception was assessed using three different tests. A standing test was performed that was a modification of that described by Al-Othman et al. 1 (Fig. 2). With the patient standing and blindfolded, the position of the feet was marked on the floor. The patient then raised one leg so that the knee and hip both flexed to 90°. The patient then repositioned his or her foot to the original starting position on the floor as accurately as possible. The patient practiced the movement twice, then the trial was repeated six times, with measurements taken of the deviation from the original starting position. The contralateral leg was then tested in the same fashion.
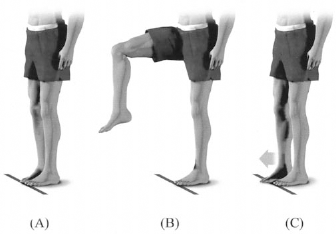
Standing proprioception test: A, initial position; B, flexed position; C, return to initial position.
A supine test was performed with the patient lying on an examination table (Fig. 3). The patient's feet were positioned on an adjacent wall approximately 30 cm above his or her hips, keeping the knees and hips flexed 30°. The patient maximally flexed both the hip and knee of the leg being tested and attempted to reposition his or her foot to the original starting position. After two practice movements, the trial was repeated six times with measurements taken of the deviation from the starting position. The contralateral leg was then tested in the same manner.
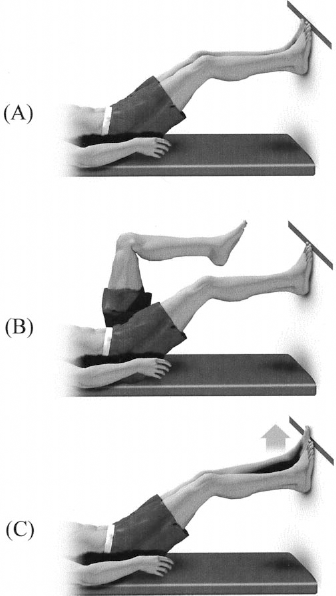
Supine proprioception test: A, initial position; B, flexed position; C, return to initial position.
A sitting test was performed and is depicted in Figure 4. The patient positioned his or her leg with the knee flexed to 30°, then let the legs hang to 90° and attempted to reposition them to the original starting position of 30° of knee flexion. After two practice movements, a trial of six movements was performed, with measurement of the deviations from the starting point. The contralateral leg was then tested. In all cases, the leg tested first was chosen randomly. For each leg, the six measured deviations were averaged. The difference in average deviation between the legs was then calculated.
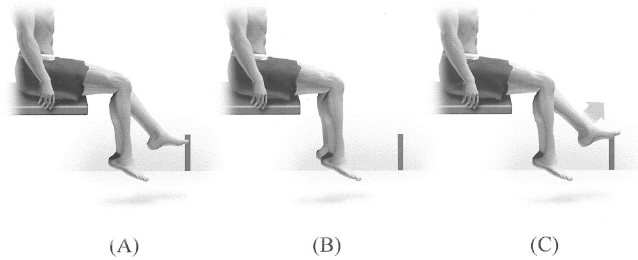
Sitting proprioception test: A, initial position; B, flexed position; C, return to initial position.
For comparison with the tibial eminence fracture group and overall validation of the proprioception testing, a control group of 10 patients with known ACL deficiency underwent the three proprioception tests and KT-1000 arthrometer testing. Anterior cruciate ligament deficiency was documented in all cases by MRI. All of the ACL-deficient patients had undergone a period of physical therapy consisting of range of motion and quadriceps and hamstring muscle strengthening before testing.
A third group consisted of 10 patients who had undergone ACL reconstruction with bone-patellar tendon-bone autografts. None of these patients had a pathologic condition of the meniscus or other ligamentous injury, and they experienced no postoperative complications. These patients underwent the three proprioception tests and KT-1000 arthrometer testing. In all cases and for all groups, the examiner was blinded as to which knee had been injured.
The injured knee was compared with the uninjured knee in all three groups using a paired Student's t-test. The Student's t-test was used to compare the tibial eminence fracture group with the ACL-deficient group, the tibial eminence fracture group with the ACL-reconstructed group, and the ACL-reconstructed group with the ACL-deficient group. The Bonferroni adjustment was made to correct for the use of multiple comparisons. Correlation analysis was performed to determine the relationship between knee laxity and proprioception among all patients, using the Spearman nonparametric analysis.
Results
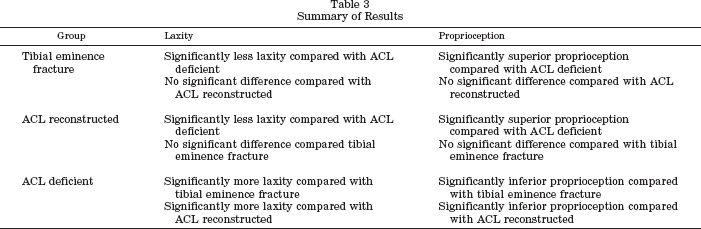
The average Lysholm knee score was 94 for the tibial eminence fracture group. Results of KT-1000 arthrometer side-to-side difference testing and proprioception testing side-to-side difference are summarized in Table 2. Compared with the ACL-deficient group, the tibial eminence fracture group demonstrated significantly less laxity in all three tests (P < 0.05) and superior proprioception in all three tests (P < 0.05). Compared with the ACL-deficient group, the ACL-reconstruction group demonstrated significantly less laxity in all three tests (P < 0.05) and superior proprioception in all three tests (P < 0.05). The tibial eminence fracture group was not significantly different from the ACL-reconstructed group with respect to laxity and proprioception. All results are summarized in Table 3.
Side-to-Side Differences in Laxity (KT-1000) and Proprioception Testing for the Three Groups

Summary of Results
When comparing the injured knee with the uninjured knee within the ACL-deficient group, the injured knee had significantly greater laxity (P < 0.05) and inferior proprioception (P < 0.05). Significant differences were not observed when comparing the injured knee with the uninjured knee in the tibial eminence fracture group or the ACL-reconstruction group.
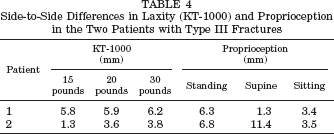
The two patients with untreated type III fractures both had greater than a 3-mm side-to-side difference on KT-1000 arthrometer testing, indicating incompetence of the ACL (Table 4). Furthermore, they had inferior proprioception when compared with the treated tibial eminence fracture group, which was a finding more typical of the ACL-deficient group.
Side-to-Side Differences in Laxity (KT-1000) and Proprioception in the Two Patients with Type III Fractures
Correlation was observed between laxity measured by KT-1000 arthrometer testing at 30 pounds of force and proprioception while standing (r = 0.631), lying supine (r = 0.582), and sitting (r = 0.608).
One patient experienced loss of range of motion immediately after immobilization of a type I fracture for 6 weeks. Aggressive physical therapy was initiated and full range of motion was regained. No patients demonstrated limited range of motion at follow-up.
Discussion
The first series of patients with tibial eminence fractures was reported by Garcia and Neer 8 in 1958. Meyers and McKeever 27 later developed a well-accepted classification system based on the amount of displacement of the fragment. The most common treatment recommendation for type I and type II fractures, which are nondisplaced or minimally displaced, has been closed reduction and immobilization. 26 For completely displaced type III fractures, both open and arthroscopic techniques with fixation including sutures, wires, and screws, have been recommended.24,27,29,33,34,38 The goals of treatment include restoring the stabilizing function of the native ACL and eliminating any mechanical block to motion. However, follow-up studies have demonstrated a disturbing amount of residual laxity.4,9,11,12,32,35,38
Several open surgical techniques have been designed to reduce and stabilize the fragment. Fixation methods have included use of suture,9,16,26,27,33,35,36 K-wires,2,35,36,38 and screws. 15 McLennan 24 believed that arthroscopic techniques allowed early mobilization, reduced hospital stay, and allowed faster rehabilitation. In addition, arthroscopic procedures allow for complete inspection of the joint for associated injuries, including osteochondral injuries and meniscal tears.12,24,34 Furthermore, type II and III fractures may be difficult to differentiate on radiographs and may be more accurately assessed arthroscopically. 34 Many authors have described arthroscopic techniques for suture fixation12,23,24,35,36 and screw fixation.19,34 Arthroscopic reduction and fixation may be technically demanding, however.
We treated 10 patients with tibial eminence fractures, 8 of whom had acute injuries. Of these, two patients were treated with a closed procedure, five with an open procedure, and one was treated arthroscopically, according to the preference and ability of the treating surgeon. The eight patients with acute injuries had anatomic reduction and bony union as demonstrated by plain radiographs at follow-up examination. Thus, although the treatment methods differed, the treatment goals of anatomic reduction and bony union were achieved in all cases. Therefore, these patients were used as subjects to analyze ACL function after injury to the ACL complex with bony fracture.
Several studies have reported on tibial eminence fractures in children only,9,21,25 and most authors believe that these fractures are more common in children than in adults.27,29,38 Hayes and Masear, 10 however, surveyed the literature and found that 40% of these fractures occur in adults. Skeletally mature patients may have different outcomes than children. They do not have the immature growth plates responsible for the relative bony weakness and do not have growth potential that may affect healing and ultimate length of the stretched ACL. In addition, a treatment option for skeletally mature patients with ACL incompetence is ACL reconstruction. Retaining the native ACL by reduction and fixation of the eminence fracture has the potential advantages of maintaining the proprioceptive function and the biomechanical stabilizing function of the ACL.
Biomechanical studies have demonstrated that a significant amount of plastic deformation of the ligament occurs before failure, 28 and clinical reports have demonstrated significant knee laxity at follow-up.4,11,12,32,35,36,38 Two factors are likely responsible for the residual laxity. One, imperfect reduction may result in malunion that effectively lengthens the ACL complex. Two, plastic deformation of the ligament (by as much as 50%) before ultimate bony fracture may lead to laxity. 28 Several researchers have observed symptoms related to the residual laxity,9,36 and others have found patients asymptomatic.11,35 Wiley and Baxter 35 found that only in patients with type III fractures was there a correlation between fracture displacement after healing and knee laxity, as well as between knee laxity and Lysholm score.
In a recent study, Mah et al. 21 reported on nine skeletally immature patients with type III fractures who were all treated with arthroscopic reduction and suture fixation. At follow-up, all patients had a negative Lachman score and pivot shift examination. The KT-1000 arthrometry results averaged 2.5 mm of side-to-side difference with 20 pounds of force.
Our laxity examination using KT-1000 arthrometry demonstrated an average side-to-side difference of 1.4 mm with 30 pounds of force for the tibial eminence fracture group. These results indicate a competent ACL. Furthermore, the tibial eminence fracture group had statistically less laxity than the ACL-deficient group by KT-1000 arthrometry testing. All patients in the tibial eminence fracture group denied episodes of instability and scored well on the Lysholm questionnaire, which is sensitive to symptoms related to instability. This indicates that proper reduction and healing of tibial eminence fractures can restore anterior knee stability in adults.
In addition to providing static anterior stability, evidence now suggests that the ACL also acts as a source for neuromuscular control of the knee. Morphologic studies of the ACL have confirmed the presence of mechanoreceptors in and surrounding the human ACL.13,14,30,31 Differences in proprioception in the ACL-deficient knee when compared with normal control groups have been documented.1,3,5,7 Al-Othman et al. 1 compared position sense in patients with ACL-deficient knees with that in a normal control group by testing their ability to reposition the foot to an initial starting position. They demonstrated significantly higher mean values (43.8%) for the injured compared with the uninjured limb in the ACL-deficient group, which was not observed in the control group (4.8%).
Kennedy et al. 13 hypothesized that failure of a damaged ligament to provide neural feedback may contribute to further instability and result in progressive ligamentous laxity. Beard et al. 5 studied reflex hamstring muscle contraction latency and found significantly higher values in ACL-deficient patients versus control subjects. They found a correlation between reflex hamstring muscle contraction latency and episodes of instability and concluded that functional instability may result from the loss of proprioception associated with ACL tears. Corrigan et al. 7 investigated the hamstring-to-quadriceps power ratio and found that it correlated with proprioception. Those patients with hamstring strength dominance demonstrated better proprioception than those without. Caraffa et al. 6 conducted a prospective study of soccer players and found that the prevalence of ACL injury was lower in players who participated in proprioceptive training. They concluded that it might be possible to prevent certain injuries of the ACL with enhancement of neuromuscular control. Lephart et al. 18 studied patients after ACL reconstructions and rehabilitation and found that there was partial return of proprioceptive function.
When evaluating ACL function, we placed particular emphasis on assessing proprioception in addition to laxity. We designed a new proprioception testing method based on that described previously by Al-Othman et al. 1 In all of the tests, the uninjured limb was used as a reference, and we used the side-to-side difference to calculate our data. To validate this new method, we first tested patients with ACL-deficient knees. The ACL-deficient group demonstrated significantly higher mean values for the injured compared with the uninjured limb. The ACL-deficient group showed inferior proprioception in all three proprioception tests when compared with the ACL-reconstructed group and the tibial eminence fracture group. Although our testing method was clearly able to distinguish the ACL-deficient group from both the reconstructed and the tibial eminence fracture groups, it did not show a statistically significant difference between the tibial eminence fracture group and the ACL-reconstructed group. Several factors may contribute to why we did not see a significant difference. Some studies have demonstrated return of proprioceptive function after ACL reconstruction 17 and proprioceptive training. 6 Our testing method may not be sensitive enough to distinguish the more subtle proprioceptive differences between the ACL-reconstructed group and the tibial eminence fracture group. In addition, we found a correlation between knee laxity and proprioception. These results are consistent with the literature demonstrating the proprioceptive function of the ACL. In addition, two patients were seen late with type III eminence fractures, several months after their initial injury. Radiographs revealed nonunion of the bony fragment. In both of these cases, the laxity and proprioception testing results were more typical of the ACL-deficient patients.
Our new testing method was sensitive to detecting inferior proprioception in ACL-deficient knees. Our standing test was similar to that described by Al-Othman et al., 1 whose results were similar to ours. The standing method of testing, however, requires the proprioception of the contralateral hip and knee in addition to the ipsilateral hip for foot placement on the floor. We developed the supine and sitting tests in an effort to minimize the contribution of hip and contralateral knee proprioception to the overall measurements. With the patient in the supine position, the involvement of the contralateral hip and knee is eliminated when positioning the foot, although the ipsilateral hip participates. With the patient in the seated position, involvement of both hips and the contralateral knee are eliminated when positioning the foot. In addition, the knee flexion angle for the supine and seated position is 30°, which is similar to that of a Lachman examination. Also, the force acting on the tibia due to gravity in both the supine and seated examinations has a greater anterior-posterior component than in the standing position, and thus may better isolate ACL proprioception.
We have demonstrated that proper treatment of tibial eminence fractures in adults restores both stability and proprioception to the knee. Thus, reduction and fixation of the fracture fragment, either open or arthroscopic, is a viable alternative to ACL reconstruction in adult patients with tibial eminence fractures. Rehabilitation time is not significantly different because bone-to-bone healing is still required; however, there is no graft site morbidity or problems related to allograft tissue. Therefore, tibial eminence fractures in adults, often treated with ACL reconstruction, can also be treated successfully with fracture reduction and fixation, yielding a functionally stable knee that retains its proprioceptive function.