
Abstract
Muscle injuries are challenging problems in traumatology and the most frequent injuries in sports medicine. Muscle injuries are capable of healing, although slowly and occasionally with incomplete functional recovery. We observed that lacerated muscle undergoes a rapid process of regeneration, which is hindered by the development of fibrosis. Biologic approaches to enhance muscle regeneration and prevent fibrosis are being investigated to improve muscle healing after injuries. We observed that growth factors can improve muscle regeneration but cannot prevent muscle fibrosis. We investigated the use of an antifibrosis substance, decorin, as an approach to prevent fibrosis and thereby improve muscle healing after injury in murine muscle. We observed that direct injection of human recombinant decorin can efficiently prevent fibrosis and enhance muscle regeneration in the lacerated muscle. More importantly, decorin can improve the recovery of strength in the injured muscle to a level similar to that observed in normal noninjured muscle. These results suggest that injection of decorin improves both the muscle structure and the function of the lacerated muscle to near complete recovery. This study will contribute significantly to the development of strategies to promote efficient muscle healing and complete functional recovery after muscle injuries.
Muscle injury is a challenging problem in traumatology and is seen very frequently in sports medicine. Muscle injuries occur by a variety of mechanisms, such as direct forces, including muscle lacerations and contusions, and indirect forces related to strains.11,14,18,19,24,32,33,36–38,40 Injured muscle usually undergoes a process of degeneration and regeneration. It has been observed that the injured muscle fibers first undergo necrotic changes, during which the damaged myofibers are removed by macro-phages. 22 New muscle fibers regenerate within the connective tissue framework of the damaged muscle. Even though these new muscle fibers have the ability to regenerate after injury, the healing process proves to be very slow and often leads to incomplete functional recovery.
We have developed a reproducible muscle laceration injury model in mice.32,37,38 We have chosen a model of muscle laceration rather than other forms of muscle injury for our study because this model is most easily reproduced and repeated in the laboratory. We are aware that muscle strains are very common clinically, and therefore we are working toward the application of these biologic approaches to prevent muscle fibrosis and improve muscle healing after strain.
The natural healing process of lacerated muscle has been monitored at different time points after injury. Recovery from muscle laceration has been evaluated by regular muscle histologic techniques, immunohistochemistry with specific marker protein, and measurement of the injured muscle's physiologic contractile properties.8,9,25,26,32,33,37,38 A regeneration process has been observed in injured muscle; however, complete recovery after injury has been hindered by the development of fibrosis, which has been found to appear during the 2nd week after muscle injury and increases over time.32,33,37,38
The long-term goal of our study is to develop biologic interventions to improve muscle healing after injuries. To achieve this goal, our research team is investigating two major procedures: the enhancement of muscle regeneration and the prevention of muscle fibrosis. Although we have observed that direct injection of specific growth factors, such as insulin-like growth factor-1 (IGF-1), basic fibroblast growth factor, and nerve growth factor, can significantly enhance muscle regeneration, the healing process remains incomplete at 1 month after injury.32,33,37,38 Moreover, we have observed that treating the injured muscle with growth factors cannot block the development of muscle fibrosis.32,33,37,38 We have further investigated the use of immobilization and suturing as means to limit fibrosis after laceration. Our results suggest that immobilization has no effect on the development of fibrosis and that the suture limits scar tissue formation in the deep part of the injured muscle but cannot prevent formation of superficial scar tissue. 38
We have therefore focused our recent effort on the development of biologic approaches to prevent muscle fibrosis after muscle injuries. Recent reports indicate that overproduction of transforming growth factor-β (TGF-β) in response to injury and disease is a major cause of tissue fibrosis in animals and humans.6,39,50,52 Decorin is a human proteoglycan that inactivates the effect of TGF-β and therefore displays a beneficial effect of antifibrosis in various tissues, such as kidney, liver, and lung.15,20,27 The aim of this study was to characterize the use of decorin as an antifibrosis agent to reduce the development of scar tissue formation after laceration and consequently improve muscle healing after injury.
Materials and Methods
The Effect of Decorin and TGF-β on Myofibroblasts in Vitro
Preparation of Myofibroblasts
The gastrocnemius muscles were removed from the hindlimbs of 3-week-old mice (C57BL10J+/+), and muscle tissue was isolated from other connective tissue. The isolated myogenic tissue was dissociated by enzymatic treatment with collagenase 0.2% (1 hour) and trypsin 0.1% (30 minutes). The preplate technique was used to dissociate the myofibroblasts from the myogenic cells because myofibroblasts tend to adhere to the substratum faster than do myoblasts and other muscle cell types.43,45 The myofibroblasts were obtained in the first preplate and suspended in 24-cm2 tissue-culture flasks coated with collagen (1 hour). The myofibroblasts were maintained in Dulbecco's modified Eagle medium without serum. The cells were stained with desmin, a myogenic marker, to test for their myogenicity.8,9 As previously reported, we observed that the cell population obtained at the first preplate contained less than 5% desmin-positive cells.43,45 These cells were consequently extremely rich in myofibroblasts and were selected for our myofibroblast cell culture in vitro.
The myofibroblasts (500,000 cells) were incubated with TGF-β (25 μg), decorin (25 μg), or TGF-β and decorin (25 μg/25 μg). Each group was composed of five samples. We then compared the level of cell proliferation to that of the control (serum-free medium without TGF-β and decorin) at 24, 48, and 72 hours after the incubation. The number of cells was monitored and compared among the different groups.
Determination of the Biologic and Physiologic Effects of Decorin on Muscle Healing after Laceration
Animal Model of Muscle Laceration
Sixteen mice (C57BL10J+/+; 3 weeks of age; approximate weight, 15 to 20 g) were used in this experiment. The policies and procedures of the animal laboratory are in accordance with those detailed by the United States Department of Health and Human Services. The Animal Research and Care Committee of the authors’ institutions approved the research protocols used for these experiments (protocol no. 2/98). A muscle laceration model was developed in mice with the gastrocnemius muscle of each leg lacerated.32,37,38 The mice were anesthetized using 0.03 ml ketamine (100 mg/ml) and 0.02 ml xylazine (20 mg/ml) by intramuscular injection. The muscles were lacerated with a surgical blade (No. 11) at the largest diameter, through the lateral 50% of their width and 100% of their thickness.1,32,37,38 Polydioxanone suture material (PDSII 5–0, Ethicon, Somerville, New Jersey), 4 mm in length, was placed at the medial edge of the lacerated site and left on the skin on the posterior side of each leg as a marker for the lacerated site. After the laceration was made, the skin was closed with 4–0 black silk.
The injection of decorin was performed along the polydioxanone suture material with a microsyringe. The mice were divided into four groups with different time points (0, 5, 10, and 15 days) of injection after laceration. At each time point, four different concentrations of human recombinant decorin were used (0, 5, 25, and 50 μg in 20 μl of phosphate-buffered saline solution). In the sham-injected group, the negative control, the muscle was lacerated the same way but injected with phosphate-buffered saline solution alone. Each group consisted of two muscles each for histologic examination. All animals were sacrificed for evaluation of healing and regeneration 2 weeks after the injection. The gastrocnemius muscles were isolated and frozen in 2-methylbutane precooled in liquid nitrogen. Regular histologic and immunohistochemical techniques for the expression of vimentin were monitored to evaluate the development of scar tissue formation after injury.
Characterization of Muscle Fibrosis after Decorin Injection
Twelve mice were used in this experiment. The mice were divided into four different decorin concentration groups and a normal control group. Decorin was injected 15 days after laceration. The concentrations were 0 (control), 5, 25, and 50 μg of decorin in 20 μl of phosphate-buffered saline solution. Two weeks after the injection, all animals were sacrificed for evaluation of healing and regeneration. Two muscles of each group were used for the regular histologic and immunohistochemical techniques for vimentin expression. The vimentin was monitored to evaluate the development of scar tissue formation within the injured muscle after injury.
We measured the surface area of muscle fibrosis among the different groups using a technique previously described.32,33 These measurements were made in a blinded manner by an independent investigator who was unaware which groups were treated or used as a control to ensure the objectivity of the results. Briefly, to measure the total vimentin-positive area under the fluorescence microscope, 10 random fields were selected for each sample and images were collected using an Olympus Provis epifluorescence microscope (Olympus Optical Co., Ltd., Tokyo, Japan) and a Sony 970 3 chip CCD camera (Sony, Tokyo, Japan). Images were digitized using a Coreco frame grabber board (Coreco Imaging, St. Laurent, Quebec, Canada) and rendered to monochrome, features were extracted, and the absolute area of vimentin-positive staining was measured in each image field.
Characterization of Muscle Regeneration after Decorin Injection
We monitored the number and diameter of the regenerating myofibers within the injured site treated with human recombinant decorin (0, 5, 25, and 50 μg in 20 μl of phosphate-buffered saline solution) and compared the results among the different groups. Again, these measurements were made in a blinded manner to ensure the objectivity of the results. Five random fields were selected for each sample to measure the total number and diameter of regenerating myofibers within the injured site using a protocol previously described.32,33,37
Characterization of Muscle Strength after Decorin Injection
The muscle was lacerated as described earlier and injected with decorin 15 days after injury. Groups injected with 0 (control) and 50 μg of decorin in 20 μl of phosphate-buffered saline solution were examined by physiologic testing for functional recovery 15 days after injection. Five muscles per group were assayed to analyze fast-twitch and tetanus strength and compared with a normal age-matched noninjured muscle. The mice were anesthetized using 0.03 ml ketamine (100 mg/ml) and 0.02 ml xylazine (20 mg/ml) by intramuscular injection. Both gastrocnemius muscles were removed, mounted in a double-jacketed organ bath of 5 ml of Krebs solution at 36°C (millimole/liter: NaCl, 113; KCl, 4.7; CaCl2, 1.25; MgSO4, 1.2; NaHCO3, 25; KHPO4, 1.2; glucose, 11.5), and constantly bubbled with a mixture of 95% oxygen and 5% carbon dioxide. The initial tension was set at 20 mN, and isometric contractions were measured with strain gauge transducers coupled with a TBM4 strain gauge amplifier (World Precision Instruments, Sarasota, Florida) and recorded on a computer using a data acquisition program (Windaq, DATAQ Instruments Inc., Akron, Ohio). After 20 minutes of equilibration, electrical field stimuli were applied through two platinum wire electrodes positioned on the top and bottom of the organ bath and separated by 4 cm. The muscles were stimulated with square wave pulses of 0.25 ms duration with maximal voltage (50 V). First, 1-Hz stimulation was applied, and the muscle twitches were recorded for 6 minutes; then six tetanic stimulations were applied for 0.5 seconds. Train duration was measured at 100 Hz every 10 seconds. Finally, the muscle strength was reported in millinewtons (mN).
Statistical Analyses
The average and standard deviation of the vimentin-positive area, number of regenerating myofibers, diameter of the myofibers, fast-twitch strength, and tetanus strength were compared among the different groups using a Student's t-test for statistical analysis. Statistical significance was defined as P < 0.05.
Results
The Effect of Decorin and TGF-β on the Proliferation of Myofibroblasts in Vitro
The effect of decorin and TGF-β on the proliferation of myofibroblasts 72 hours after incubation is shown in Figure 1. Transforming growth factor-β has a stimulating effect on myofibroblast proliferation in vitro. Indeed, the number of myofibroblasts in the group treated with TGF-β was significantly higher at 48 and 72 hours after incubation when compared with the numbers in the control group (Fig. 1). Decorin, in contrast, inhibited myofibroblast proliferation at 72 hours after incubation when compared with the control group. In fact, the number of myofibroblasts in the decorin-treated group was significantly lower at 48 and 72 hours after incubation when compared with the number in the control group (Fig. 1). The cells treated with both TGF-β and decorin showed a similar pattern of cell proliferation as observed in the control group. In fact, the co-incubation of decorin with TGF-β significantly reduced the stimulating effect of TGF-β and thereby decreased the level of myofibroblast proliferation.
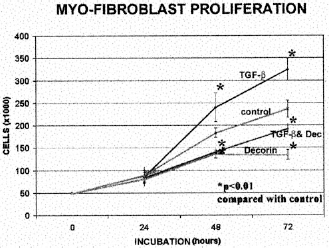
Effect of TGF-β and decorin on the proliferation of myofibroblasts in vitro at 24, 48, and 72 hours after incubation. The asterisks indicate a significant difference between the control and treated groups.
Determination of the Biologic and Physiologic Effects of Decorin on Muscle Regeneration
We observed that direct injection of human recombinant decorin (50 μg) at 10 and 15 days after injury significantly decreased the amount of fibrosis and enhanced muscle regeneration when compared with the muscles in the control group injected with saline solution.
Muscle Fibrosis and Regeneration
Injection of high concentrations of human recombinant decorin (25 to 50 μg in 20 μl phosphate-buffered saline solution) appeared to result in better prevention of fibrosis than the lower concentrations of decorin (25 and 0 μg) (Figs. 2 through 4), as seen in the histologic examination. By using immunohistochemical techniques for vimentin staining to characterize the muscle fibrosis area, we were able to observe that scar tissue formation was significantly less in the experimental groups treated with 25 and 50 μg of decorin than in the control group (P < 0.05). Moreover, the positive effect of decorin in the development of muscle fibrosis seemed to be dose-dependent (Figs. 2 through 4). Although a significant reduction of fibrosis was observed with doses between 5 and 50 μg of decorin, no significant difference was observed between 5 and 25 μg or between 25 and 50 μg.
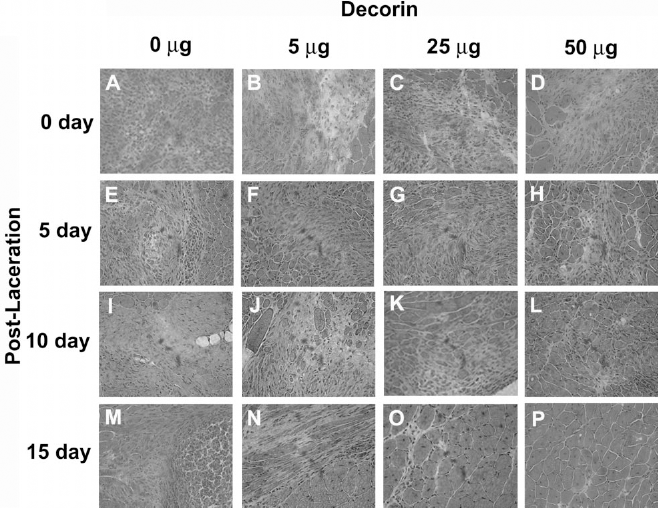
Histologic evaluation of the lacerated muscle after decorin injection. Panels A, B, C, and D show lacerated muscle injected immediately after the injury with 0, 5, 25, and 50 μg of decorin. Panels E, F, G, and H show muscle injected with 0, 5, 25, and 50 μg of decorin 5 days after laceration. Panels I, J, K, and L show muscle injected with 0, 5, 25, and 50 μg of decorin 10 days after laceration. Panels M, N, O, and P show muscle injected with 0, 5, 25, and 50 μg of decorin 15 days after laceration. (original magnification, ×20)
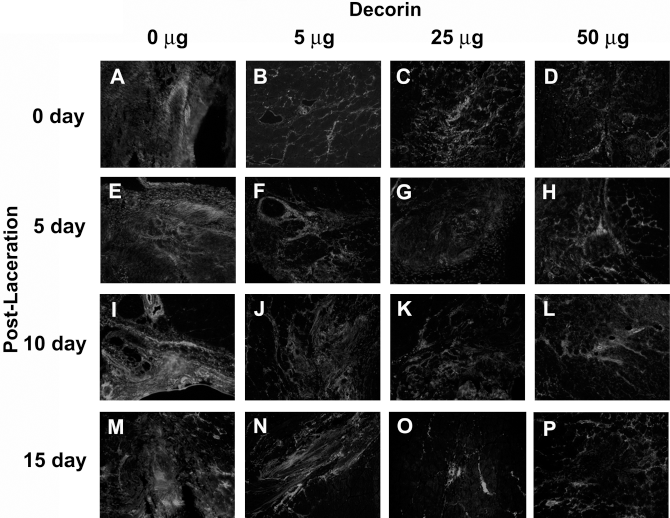
Immunohistochemical staining forvimentin (fibrosis) in the lacerated muscle injected with decorin. Panels A, B, C, and D show lacerated muscle injected immediately after the injury with 0, 5, 25, and 50 μg of decorin. The muscles in panels E, F, G, and H were injected with 0, 5, 25, and 50 μg of decorin at 5 days after laceration. The muscles in panels I, J, K, and L were injected with 0, 5, 25, and 50 μg of decorin at 10 days after laceration. The muscles in panels M, N, O, and P were injected with 0, 5, 25, and 50 μg of decorin at 15 days after laceration. (original magnification, ×20)
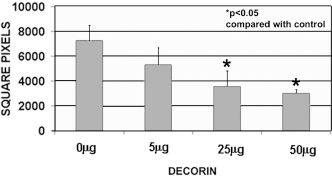
Quantitation of the surface area of fibrosis found in muscles injected with various amounts of decorin and compared with the control group.
The histologic findings support the contention that decorin at high concentrations inhibits the development of fibrosis (Fig. 2). In addition, by monitoring the number of regenerating myofibers (center-nucleated myofibers) within the injured site, we observed a significantly higher number of regenerating myofibers in all the decorin-treated groups when compared with the controls injected with phosphate-buffered saline solution alone (P < 0.01) (Fig. 5A). We also observed a significantly higher number of regenerating myofibers in the other experimental groups: 50 μg compared with 5 μg, and 50 μg compared with 25 μg. When the diameter of regenerating myofibers was measured, we observed that the high dose of decorin (25 to 50 μg) led to an increase in the diameter of the regenerating myofibers when compared with those from the control group (P < 0.01) (Fig. 5B). Again, a similar trend was observed with the diameter of regenerating myofibers, and a significant difference was observed between the experimental groups: 50 μg compared with 5 μg and 50 μg compared with 25 μg. However, no significant difference was observed between the 5 μg and 25 μg groups.
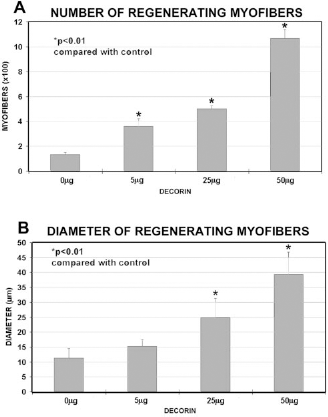
A, the number of regenerating myofibers according to the level of decorin administered. B, the diameter of regenerated myofibers according to the level of decorin administered.
Physiologic Testing of the Injured Muscle Treated with Decorin
The muscles treated with the highest dose of decorin (50 μg) were selected for physiologic testing. The muscle was lacerated as described earlier, and the decorin was injected at 2 weeks after injury. The effect on the lacerated muscle was observed by physiologic testing (tetanus strength and fast-twitch strength) and compared with that in the control group. The fast-twitch muscle strength was 38.17 ± 4.01 mN in the normal muscle group, 20.75 ± 2.26 mN in the control group (20 μl phosphate-buffered saline solution), and 38.04 ± 4.86 mN in the decorin-treated group (50 μg in 20 μl phosphate-buffered saline solution). There was no major difference between the normal noninjured and decorin-treated groups (Fig. 6A). However, we observed significant differences between the control group and the decorin-treated group (Fig. 6A).
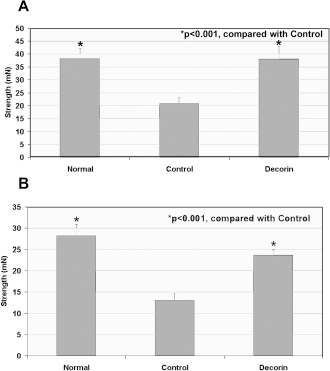
Physiologic effects of decorin injection on muscle strength. The injection of a high dose of decorin (50 μg) at 15 days after laceration led to a significant improvement of fast-twitch (A) and tetanus (B) strength of the lacerated muscle when compared with the control group (P < 0.05). More importantly, the muscle strength of the injured muscle treated with decorin was not significantly different from the strength of a normal age-matched noninjured muscle.
Similarly, the tetanus muscle strength was 28.15 ± 2.70 mN in the normal muscle group, 13.02 ± 1.52 mN in the control group, and 23.67 ± 1.27 mN in the decorin-treated group. There was still a significant difference between the control group and the decorin-treated group (P < 0.001) (Fig. 6B). The tetanus strength of the injured muscle healed with decorin was not significantly different from that in a normal noninjured muscle.
Discussion
Muscle injuries account for a large number of professional and recreational sports injuries.34,42 The long-term goal of treatment for muscle injury is complete recovery for both muscle healing and function. The best treatment for these injuries has not yet been clearly defined, and the recommended treatment regimens vary widely depending on the severity of the injury. 49 The suggested treatments currently include rest, ice, heat, water pool, compression, elevation, immobilization, aggressive full range of motion through passive motion machine, drugs, and hospitalization.3,4,10,23,28,46 These procedures are generally not sufficient to efficiently enhance muscle regeneration and prevent muscle fibrosis, especially in patients who wish to return quickly to high levels of sports activity. In addition, significant complications, such as early functional and structural deficits, reinjury, muscle atrophy, contracture, and pain often occur after muscle injuries, resulting in, for example, time lost from training and competition.3,4,10,23,28,46 These unmet medical needs prompted us to seek novel strategies to improve muscle healing.
Discerning the ability of muscle cells to regenerate after injury is essential to the understanding of many diseases affecting skeletal muscle, such as muscular dystrophy. Skeletal muscle is capable of extensive regeneration after injuries including contusions, lacerations, and strains.11,14,18,19,24,32,33,36–38,40 The myogenic cells responsible for this regeneration are the mononucleated satellite cells, located between the basal lamina and plasma membrane of the muscle fiber.7,25 After muscle injury, it is hypothesized that disruption of the basal lamina and plasma membrane releases and activates the satellite cells.7,25 The satellite cells begin to proliferate and differentiate into multinucleated myotubes and eventually into myofibers. The growth of these regenerating myofibers into the injured site promotes the healing of the muscles.
The events in muscle tissue repair have been observed in both animal models and clinical experience25,26; however, muscle injuries seen in medical practice are usually found to be more destructive than those in animal models. 25 The injured gap is usually filled with hematoma, which matures into proliferating granulation tissue and eventually results in the formation of connective scar tissue. These events not only make the repair complex, but they may also inhibit the complete regeneration of muscle tissue and contribute to only partial functional recovery. 25 The parallel occurrence of muscle regeneration and scar tissue formation in the injured muscle may lead to a competition between systems during the healing process.32,33,37,38
Many growth factors have been shown capable of stimulating growth and protein secretion of musculoskeletal cells. 51 During muscle regeneration, it is presumed that trophic substances released by the injured muscle activate the satellite cells.1,7,25,48,51 Preliminary data have further suggested that individual growth factors play a specific role during muscle regeneration.2,12,21,29–31,36,47
Another group of growth factors, IGF-1 and IGF-2, have been found mitogenic for myoblasts.17,44 Insulin-like growth factor-1 is critical in mediating the growth of muscle and other tissues. 16 Systemic administration of IGF-1 results in increased muscle protein content and reduced protein degradation. 53 More importantly, overexpression of IGF-1 has been correlated with muscle hypertrophy in transgenic mouse lines. 13 With aging, a decrease in the production and activity of the growth hormone/IGF-1 axis leads to an increase in catabolic processes, which is exhibited by the age-related loss of muscle mass and strength. 35 Muscle mass loss has been prevented in healthy people by administering growth hormone that increases the level of IGF-1. 41 Recently, gene transfer of IGF-1 by an adeno-associated vector into mouse skeletal muscle was shown to significantly slow the aging process. 5
We have characterized the efficiency of muscle recovery after different models of muscle injury and have observed an active muscle regeneration process occurring in the early stages of healing that eventually becomes impaired by the development of scar tissue in the injured muscle.32,33,37,38 We have also identified specific growth factors (IGF-1, basic fibroblast growth factor, and nerve growth factor) capable of enhancing myoblast proliferation and differentiation in vitro and investigated the delivery of these growth factors into the injured muscle to improve muscle healing in vivo.32,33,37 Although the direct injection of the recombinant proteins basic fibroblast growth factor and nerve growth factor displays some beneficial effect on muscle healing after injuries, IGF-1 has been found capable of mediating the highest improvement of muscle healing after all of the muscle injuries tested: laceration, contusion, and strain.32,33,37 These growth factors enhanced muscle regeneration but were unable to prevent scar tissue formation, which still occurs in the injured muscle and therefore impairs the healing process.32,33,37
Although we are working on the development of approaches to achieve a persistent level of expression of growth factors into the injured muscle using cell and gene therapy, we recently attempted to develop biologic approaches to directly block muscle fibrosis. We observed that immobilization of the lacerated muscle has no significant effect on the development of fibrosis, whereas suture is capable of limiting fibrosis deep in the injured muscle but is still incapable of eliminating the superficial muscle fibrosis. 38
Decorin is a human proteoglycan that inactivates the effect of TGF-β6,39,50,52 and therefore displays a beneficial effect of antifibrosis in various tissues, such as kidney, liver, and lung.15,20,27 The decorin gene has been successfully delivered into skeletal muscle, and the secreted decorin protein prevented fibrotic disease in a rat kidney. 27 No toxicity has been detected as a result of decorin gene transfer. The antifibrosis effect of decorin has not been reported in skeletal muscle thus far. In our study, we investigated the antifibrosis effects of decorin in lacerated muscle tissues using the direct injection of various concentrations of the recombinant protein decorin at different time points after laceration. The effect of decorin on muscle fibrosis, muscle regeneration, and the overall muscle healing was determined at various time points after injection. The salient features of the results presented in this report include the following.
Decorin Inactivates the Stimulating Effect of TGF-β on Myofibroblast in Vitro. We tested in vitro whether decorin acts as an inhibitor of TGF-β on the proliferation of myofibroblasts, which is the likely cellular source of muscle fibrosis. We observed that TGF-β significantly increased the level of myofibroblast proliferation at 72 hours after incubation when compared with the control group. In contrast, decorin decreased the proliferation of myofibroblasts in vitro when compared with the control group. Moreover, the co-incubation of decorin with TGF-β neutralized the stimulating effect of TGF-β on the proliferation of myofibroblasts. Although the mechanism by which decorin acts on TGF-β was not investigated in this study, the ability of decorin to bind to TGF-β and prevent its association with its receptor is a likely mechanism of action in muscle healing.15,20,27
Beneficial Effect of Decorin in Muscle Fibrosis. We observed that direct injection of human recombinant decorin protein into the lacerated muscle in vivo decreased the amount of fibrosis in injured muscle. We injected different doses of decorin at different time points after muscle laceration and monitored the level of fibrosis at 2 weeks after the decorin injection. When we compared histologic findings within muscles with the same time point of injection, we observed that 50 μg of human recombinant decorin injection decreased fibrous scar tissue formation more than did the amounts of the other experimental groups at all time points tested. Also, we observed many regenerated myofibers within the lacerated site in the experimental group treated with decorin; the lacerated site was usually filled with fibrous scar tissue in the non-decorin-treated groups. Furthermore, when we compared the same doses of decorin injected at different time points, we observed that the injection of decorin at 10 and 15 days after injury led to the maximal antifibrosis effect.
The Antifibrosis Effect of Decorin Leads to an Enhancement of Muscle Regeneration. The groups injected with decorin (25 and 50 μg) at 15 days after injury displayed an enhancement of muscle regeneration. Indeed, both the number and the diameter of regenerating myofibers were increased in the decorin-treated group. These data suggest that human recombinant decorin injection is capable of preventing fibrous scar tissue formation and consequently of improving muscle regeneration. Our results indicated a dose-dependent effect of decorin at 2 weeks after laceration.
The Use of Decorin Leads to an Enhancement of Muscle Strength. Biologic and physiologic effects of decorin injection were monitored in our third experiment. Two weeks after laceration, we injected 50 μg of decorin to improve muscle strength in the lacerated muscle. The results of physiologic testing showed that there was significant improvement in muscle strength in the decorin-treated groups when compared with the control group (lacerated muscle injected with phosphate-buffered saline solution alone). More importantly, we observed that the decorin was capable of improving recovery of muscle strength of the injured muscle at a level similar to that observed in noninjured muscle at the same age. These results strongly suggest that injection of 50 μg of decorin improved the functional muscle recovery of the lacerated muscle to a near complete recovery at 2 weeks after injection.
Summary
We observed that injection of decorin at 2 weeks after muscle laceration resulted in an effective prevention of muscle fibrosis and enhancement of muscle regeneration and led to a near-complete functional muscle recovery. In the future, we will attempt to study the effect of decorin injection on other muscle injuries, especially muscle strain. Muscle strain is the most frequent type of muscle injury seen in sports medicine. 18 For our initial study we selected the muscle laceration model because of its ease of reproducibility. Muscle strains differ from lacerations because they are caused by forcible stretching of the muscle, most often during eccentric contraction. This results in an injury at the site of the muscle-tendon junction, a phenomenon not usually present in muscle laceration injuries. 18 Other aspects of strains, however, are similar to the characteristics of lacerations, such as the development of significant fibrosis and the ensuing process of muscle regeneration. 32 Therefore, we will apply similar techniques of decorin injection in future studies of muscle strain injuries.
Although a major improvement in muscle healing was observed in this study, a large amount of recombinant protein was required to efficiently improve the healing of a very small mouse muscle. We will therefore further investigate the use of gene therapy and cell therapy procedures (direct and ex vivo) to deliver a high level of decorin expression to the injured muscle. Those procedures should deliver a persistent high level of expression of the antifibrosis substance and thereby may improve muscle healing more effectively in human patients, who would otherwise require very large amounts of those proteins. It will also be necessary to study the safety of the use of antifibrosis agents on human subjects before these results can be applied clinically. These studies should help develop strategies to promote efficient, functional recovery after laceration injury. We hope that with further study the utility of antifibrosis agents in the treatment of other common muscle injuries can be evaluated.