
Abstract
Seventy-five patients underwent unilateral anterior cruciate ligament reconstruction with an ipsilateral bone-patellar tendon-bone autograft at our institution. The graft was harvested using a two-transverse-incision technique, and patellar and tibial bony defects were repaired with cored bone grafts collected by reaming the femoral socket and the tibial socket or tunnel. We evaluated the incidence of anterior knee pain, donor site tenderness, and sensory disturbance after use of these procedures. We also analyzed the correlation between anterior knee pain and age, sex, bone plug length, range of motion, postoperative stability, patellar tendon shortening, infrapatellar nerve injury, and the size of the patellar defect. Thirteen patients reported anterior knee pain. Donor site tenderness was detected in 10 patients and was located on the inferior pole of the patella, the tibial tubercle, or both. Sensory disturbance was found over the infrapatellar nerve area in 13 patients. Statistical analysis showed that anterior instability (side-to-side difference of 3 mm) and residual patellar bony defect (depth 2 mm) were risk factors for anterior knee pain. The results of our study suggest that cored cancellous bone grafting for complete restoration of the donor site bony defects and the two-transverse-incision technique to preserve the infrapatellar branch of the saphenous nerve contribute to prevention of anterior knee symptoms.
The use of the central one-third of the autogenous patellar tendon to reconstruct the torn ACL is recognized as a successful procedure with excellent clinical results. The advantages of bone-patellar tendon-bone graft include high initial tensile strength and stiffness,24,30,38 rigid fixation using the interference screw technique, 17 and direct bone-to-bone healing. 7 These biomechanical and biologic characteristics permit aggressive postoperative rehabilitation and an early return to sports activities. However, harvesting a bone-patellar tendon-bone autograft can harm the knee extensor mechanism and may cause serious complications involving patellar fracture,3,37 rupture of the remaining patellar tendon,18,19 and degeneration of the patellofemoral articular surface. 34
Anterior knee pain has been described as the most common complication after ACL reconstruction with a bone-patellar tendon-bone graft and results in a decrease in patient satisfaction. In previous reports, the rate of postoperative anterior knee pain ranged from 4% to more than 40%. 2,4,14,16,26,27,33 The donor site morbidity associated with harvesting a hamstring tendon graft is less common than that associated with harvesting a bone-patellar tendon-bone autograft.5,35,40 This is one of the reasons that surgeons have recently shifted to increased use of semitendinosus and gracilis tendon grafts. The relationship between postoperative anterior knee pain and flexion contracture,25,29 shortening of the remaining patellar tendon,1,23 residual anterior instability, 9 and a cyclops lesion 12 has been debated, but the causes of anterior knee pain are still unclear.
In 1998, our institute reported the results of a study that evaluated anterior knee pain after ACL reconstruction with an ipsilateral bone-patellar tendon-bone autograft and especially focused on donor-site tenderness and sensory disturbance. 8 Sixty-seven patients were observed for a minimum of 12 months, and 34% of them reported anterior knee pain. Donor-site tenderness was found on the inferior patella in 24% and on the tibial tubercle in 45%. Hypoesthesia or anesthesia over the area of the infrapatellar branch of the saphenous nerve was present in 93% of patients. These symptoms limited the patients’ ability to perform daily or sports activities. In our previous series, the bone-patellar tendon-bone autograft was harvested through a vertical incision placed on the medial border of the patellar tendon, and only the patellar bony defect was repaired by grafting with chipped cancellous bone. 8 We proposed that the residual bony defect at the donor site and damage to the infrapatellar nerve branch might be associated with anterior knee pain. Therefore, since 1996, we have harvested bone-patellar tendon-bone grafts using the two-transverse-incision technique instead of the traditional longitudinal incision technique and have refilled the patellar and tibial bony defects with cored cancellous bone in addition to chipped cancellous bone.
The first purpose of this study was to determine the incidence of donor-site tenderness, sensory disturbance, and anterior knee pain after ACL reconstruction using the two-transverse-incision technique and cored cancellous bone graft. The second purpose was to establish the risk factors for anterior knee pain after ACL reconstruction as they related to patients’ age and sex, the length of the bone plugs, postoperative range of motion, anterior laxity, patellar tendon shortening, infrapatellar nerve injury, and the size of the patellar bony defect. It was hypothesized that use of our current techniques could reduce donor-site tenderness, sensory disturbance, and anterior knee pain to a level less than that experienced by the patients in our previous series. Furthermore, we hypothesized that, despite use of the newer techniques, there would still be some risk for anterior knee pain due to the patellar bony defect and damage to the infrapatellar nerve branch.
Materials and Methods
Patients
From 1996 to 1997, 93 consecutive patients underwent ACL reconstruction using an ipsilateral bone-patellar tendon-bone autograft for acute or chronic ACL deficiency. Three experienced arthroscopic surgeons (YO, YI, or HO) performed all operative procedures at the Department of Orthopaedic Surgery, Hirosaki University. This series excluded patients who had patellofemoral disorders or tibiofemoral osteoarthritis, or who had undergone previous knee surgery or multiple ligament reconstructions (for example, ACL and PCL or ACL and posterolateral corner). Seventy-five patients, 39 women and 36 men, were observed for an average of 35 months (range, 24 to 45). The mean age was 22 years (range, 14 to 45) at ACL reconstruction. Preinjury activity was classified into four levels based on results of the International Knee Documentation Committee Knee Ligament standard evaluation form. Forty-eight patients were rated level I (strenuous activity), 21 were level II (moderate activity), and 6 were level III (light activity). The period from injury to reconstructive surgery ranged from 2 weeks to 60 months and was 35 weeks on average.
Techniques for ACL Reconstruction
The graft was harvested using the two-transverse-incision technique as the initial step (Fig. 1). A 4-cm proximal horizontal incision was made centered on the inferior pole of the patella. A distal horizontal incision was made on the proximal border of the tibial tubercle, extending from 2 cm medial to 1 cm lateral of the tibial tubercle. The medial and lateral ends of the proximal incision were used as medial and lateral infrapatellar portals, respectively, for arthroscopic procedures, and the distal incision was used for reaming the tibial tunnel. The deep retinacular layer and the peritenon were also dissected sharply and horizontally at the same levels as the two skin incisions to expose the patellar tendon and its insertions on the patella and the tibia. A custom-made parallel knife containing two No. 11 blades with a 10-mm wide interval was used. This produced two incisions on the patellar tendon from the patellar origin to the tibial insertion, parallel to the tendon fibers. A rectangular bone plug, 10 mm in width and 7 to 10 mm in depth, was removed from the tibial tubercle with an oscillating saw and an osteotome. Subsequently, the bone plug was pulled under the peritenon and out through the proximal incision. To completely harvest a 10-mm wide graft, another bone plug was cut from the distal patella in the same manner. In 48 patients the bone plugs were of conventional length (20 to 30 mm); and in 27 patients they were of minimum length (15 to 20 mm).

For the two-transverse-incision technique, the proximal horizontal incision centered on the inferior pole of the patella. The distal horizontal incision was made on the proximal border of the tibial tubercle with a slight medial offset.
The tibial tunnel or socket and femoral socket were made with a coring reamer (Arthrex, Naples, Florida) or a tube harvester (Arthrex) to obtain cored cancellous bone (Fig. 2). In the 48 patients who had conventional-sized bone plugs, 23 ACL reconstructions were performed using the endoscopic technique, that is, the anterior approach to reaming the tibial tunnel, the transtibial approach to reaming the femoral socket and the placement of the graft, and insertion of an interference screw inside-out into the femoral socket and outside-in into the tibial tunnel. The ACL of the remaining 25 patients was reconstructed using the all-inside technique. 22 One bone plug was flipped back over the adjacent patellar tendon and placed into the tibial socket. This technique enabled shortening of the tendinous portion of the graft to as long as the original ACL and fixation of the bone plugs close to the outlet of the bone sockets. Reaming of both the femoral and tibial sockets and insertion of interference screws were performed in an inside-out direction. All 27 patients with minimum bone plugs underwent endoscopic ACL reconstruction. Nine torn medial menisci and seven torn lateral menisci were partially resected, and nine medial meniscal tears were repaired using an inside-out suture technique.

Cored cancellous bone was collected by reaming the femoral socket with a tube harvester (left) and the tibial tunnel with a bone core reamer (right).
The patellar and tibial bony holes where the bone plugs were removed were refilled with cancellous bone graft. First, chipped cancellous bone trimmed from the bone plugs was packed into the bony defects. Then, cored cancellous bone removed by reaming the bone socket or tunnel was driven into the patellar and tibial defects with a bone impactor to flatten the anterior surface of the grafted bone and surrounding cortical edge (Fig. 3). With the tendon defect left open, the deep retinaculum and the soft tissue were closed over the donor site layer by layer.

The bony defect, after removal of a bone plug, was filled with a cored cancellous bone graft.
Postoperatively, continuous passive motion was performed starting from the day of operation, and weightbearing was allowed as tolerated. A modified accelerated rehabilitation program was followed with emphasis on maintaining patellar mobility and obtaining immediate full hyperextension. 32 Closed kinetic chain exercises were begun immediately and progressed in difficulty as tolerated. Jogging was allowed at 3 months after the operation, and gradual progression to agility exercises and sport-specific training was adopted.
Clinical Assessment
All patients underwent a physical examination, radiographic assessment, and questioning about anterior knee pain. Anterior knee pain was defined as subjective pain or discomfort located on the anterior region of the reconstructed knee during activities of daily living, sports activities, or during rest. Pain localized to the medial or the lateral tibiofemoral joint was excluded. The presence and location of donor-site tenderness were examined by palpation, and the region with sensory disturbance was determined using light-touch and pinprick testing. The presence of anterior knee pain was evaluated based on the following factors: age (the patients were divided into two groups: under 30 years and 30 years and over), sex, and bone plug length (conventional or minimum).
Flexion Contracture
Extension lag angle was determined in the manner described by Sachs et al. 29 and calculated by measuring the heel-height difference and the lower leg length. The patients were divided into groups based on extension lag angle: 0° to 2° or more than 2°.
Anterior Knee Laxity
Anterior tibial translation was measured using the KT-1000 arthrometer (MEDmetric Corp., San Diego, California) with the knee at 20° of flexion, and the side-to-side difference was recorded for the maximum manual test. The patients were divided into two groups based on side-to-side difference: 0 to 3 mm or more than 3 mm.
Injury to the Infrapatellar Branch
On the basis of the nerve distribution, sensory disturbance extending laterally beyond midline over the infrapatellar area was ascribed to injury to the infrapatellar branch of the saphenous nerve.13,21 The patients were divided into those who had injury to the infrapatellar branch nerve and those who did not.
Shortening of the Patellar Tendon
The patellar height ratio was evaluated according to the method described by Insall and Salvati. 10 It was calculated by dividing the length of the patellar tendon by the length of the patella on lateral radiographs taken with the patient in a supine position with the knee flexed to 60°. Then the postoperative patellar height ratio (PHRpost) at the latest follow-up was compared with the preoperative value (PHRpre). The patients were divided into two groups based on the change in the patellar height ratio: PHRpost/PHRpre less than 0.9, or PHRpost/PHRpre 0.9 or more.
Patellar Bony Defect
The patellar bony defect in the donor site was evaluated radiographically. The depth from the anterior cortical surface of the patella to the bottom of the bony defect was measured on a postoperative axial view of the patella with the knee flexed to 30° (Fig. 4). The patients were divided into two groups based on depth of the defect: 0 to 2 mm or more than 2 mm.
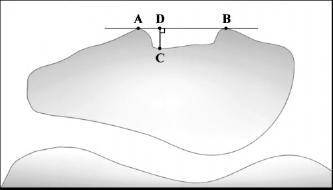
Radiographic measurement of the depth of the patellar bony defect. The first line was drawn through the lateral edge (A) and the medial edge (B), which were created by removing the bone plug. The second line was drawn perpendicular to the first line and passed through to the bottom of the bony defect (C). Point D was the intersection point of the two lines. The distance from C to D was measured, divided by the radiographic magnification coefficient, and recorded as the depth of the bony defect.
Statistical Analysis
Statistical analysis was performed using a chi-square test to characterize the relationship between anterior knee pain and the previously mentioned factors. Logistic multivariate linear regression analysis was used to determine risk factors for anterior knee pain. Significance was accepted at a P value of less than 0.05.
Results
None of the patients experienced patellar fracture or patellar tendon rupture. At the latest follow-up examinations, the mean side-to-side difference in the KT-1000 arthrometer measurement for the manual maximum test was 2.0 ± 1.5 mm. Nine knees (12%) showed more than 3 to 7 mm of side-to-side difference. Six knees (8%) had extension lags of more than 2° but less than 5°. In the radiographic evaluation, the averages in PHRpre and in PHRpost were 0.99 ± 0.11 and 0.94 ± 0.10, respectively, representing a significant difference by paired t-test (P < 0.05). Fourteen knees (19%) showed patellar tendon shortening, with 10% to 20% diminution of the patellar height. Eighteen knees (24%) showed a residual patellar bony defect of more than 2 to 7 mm in depth (Fig. 5).
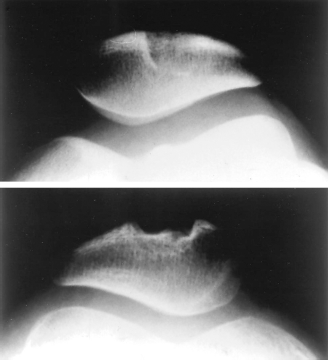
Axial radiographs of patellae showing the completely healed patellar donor site without bony step-off (above) and the poorly repaired patella (below).
Thirteen patients (17%) reported anterior knee pain, although none underwent further surgery to alleviate it. Eleven of these 13 patients reported slight pain with sports activity, and 2 patients had slight pain with daily activity. No patient, however, was impaired in their ability to perform any activities. The presence of anterior knee pain based on the factors for comparison in this study and the results of a chi-square test are shown in Table 1. A positive statistical correlation was detected between anterior knee pain and anterior knee laxity and between anterior knee pain and depth of the patellar bony defect.
Presence of Anterior Knee Pain and Results of Chi-Square Test
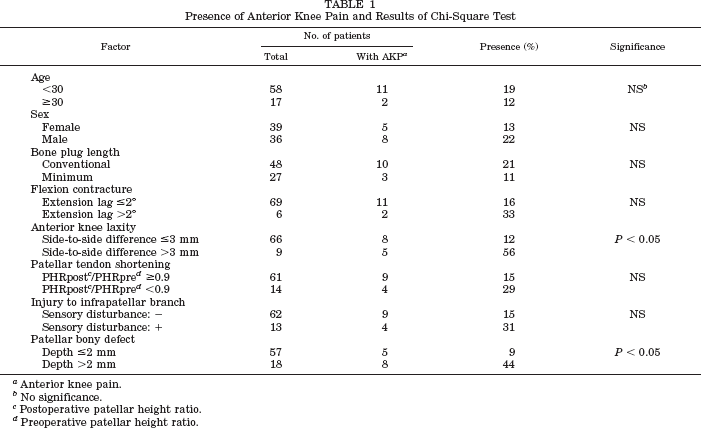
Anterior knee pain.
No significance.
Postoperative patellar height ratio.
Preoperative patellar height ratio.
The donor-site tenderness was located on the inferior pole of the patella in one patient (1%), on the tibial tubercle in five (7%), and on both in four (5%). All patients who had donor-site tenderness were in the conventional bone plug group. Furthermore, all patients who experienced patellar donor-site tenderness had a residual patellar bony defect of more than 2 mm. Sensory disturbance was found in 13 patients (17%), and the area of disturbed sensitivity extended over the lateral infrapatellar region without exception.
The logistic multivariate linear regression analysis showed that anterior laxity and patellar bony defect were independently associated with the anterior knee pain. We consequently considered residual anterior instability and incompletely repaired patellar bony defects as risk factors for anterior knee pain.
Discussion
The patients in our current study showed great improvement in donor-site symptoms compared with those in our previous series. Using two transverse incisions and cored cancellous bone grafts halved the incidence of anterior knee pain and reduced the incidence of donor-site tenderness and sensory disturbance to one-quarter and less than one-fifth, respectively, supporting our first hypothesis.
When the bone-patellar tendon-bone autograft is harvested through a longitudinal incision along the patellar tendon, there are high risks of damaging the infrapatellar branch and losing cutaneous sensation lateral to the incision.13,36 For this reason, the two-transverse-incision technique was chosen. Two incisions allow easy exposure of the distal half of the patella, the whole length of the patellar tendon, and the tibial tubercle. Mishra et al. 20 emphasized the cosmetic advantage of the two-transverse-incision. A widened scar from a longitudinal incision seriously decreases patient satisfaction, especially among adolescent girls. Mishra et al. described exposing the patellar tendon by splitting the retinacular layer vertically. However, we think that the retinacular layer should be opened horizontally because the infrapatellar branch frequently runs superficial to the retinacular layer. 11
The incidence of sensory disturbance was dramatically decreased by use of the two-transverse-incision technique; however, disturbance was still present in 17% of patients. These findings suggested that the infrapatellar nerve branch was left intact between the two incisions in most, but not all, cases. These cases may have been caused by injury to the infrapatellar branch of the saphenous nerve crossing over the patellar apex or the tibial tubercle during the incision, because the distribution of peripheral nerves varies.13,14,36 Therefore, the surgeon should make an effort to minimize the incision size, even when using the two-transverse-incision technique. We have recently had experience harvesting the bone-patellar tendon-bone graft through a single horizontal incision placed at the midlevel of the patellar tendon. This is one potential solution to lessen iatrogenic sensory disturbance.
Bone grafting of the patellar defect has also been advocated to decrease donor-site pain as well as to prevent patellar fractures. 6 Sharkey et al. 31 demonstrated that bone plug removal induced increases in axial strain of the patella, and filling the bony defect restored axial strain to normal values. These experimental findings support our clinical results that the incidence of anterior knee pain and patellar donor-site tenderness was significantly higher in knees with incompletely repaired patellar bony defects than in knees with well-refilled patellar donor sites.
Although we attempted to radiographically assess the size of tibial bony defects with lateral views, the bottom of the bony defect was not identified clearly enough to measure depth. Computed tomographic images, available in some cases, contained artifacts associated with the tibial interference screw, often degrading the profile of the tibial bony defect and making it impossible to provide accurate measurements. Therefore, we could not assess a correlation between the size of the tibial bony defect and anterior knee pain or tenderness. Although bone grafting into the tibial defect has been given little importance, the residual bony defect located on the tibial tubercle frequently induces pain with kneeling in daily and sports activities. We suggest that bone grafting should be completely achieved, not only in the patella but also in the tibial tubercle. Sufficient amounts of cored cancellous bone can be obtained for both bony defects by reaming the tibial tunnel (or socket) and the femoral socket. Although the over-shortened bone plug may jeopardize fixation strength of the replacement graft, harvesting the bone plug at a minimum length allows the bone defect to be packed more firmly. Pomeroy et al. 28 experimentally demonstrated that a bone plug longer than 10 mm did not have much mechanical advantage when using the interference fixation technique. In our current series, the mean lengths of the minimum-sized bone plugs removed from the patella and the tibia were 18.9 ± 2.3 mm and 17.0 ± 2.9 mm, respectively. No replacement graft was suspected of fixation failure.
It is widely established that ACL rupture results in abnormal tibiofemoral kinematics. 39 Equally important, it has been revealed that ACL deficiency alters patellofemoral kinematics. Hsieh et al. 9 experimentally showed that transection of the ACL resulted in lateral patellar tilt and shift, and ACL reconstruction normalized patellar tracking. These changes in patellofemoral contact characteristics might lead to abnormal pressure distribution and could be responsible for degeneration of cartilage, patellofemoral pain, and anterior knee discomfort. Our clinical outcome data, indicating that residual anterior instability is one of the risk factors for anterior knee pain, do not contradict the biomechanical findings of the Hsieh et al. study.
Because a limitation of the current study is the lack of a randomized control group, further research is needed to establish the cause of anterior knee pain after ACL reconstruction. The results of our study can, however, provide clues to solutions for donor-site morbidity associated with harvesting a bone-patellar tendon-bone autograft. We believe that cored cancellous bone grafting for complete restoration of the donor-site bony defect and the two-transverse-incision technique to preserve the infrapatellar branch of the saphenous nerve contribute to prevention of anterior knee symptoms. When these goals are successfully achieved, the bone-patellar tendon-bone autograft can continue to be the standard for an ACL substitute.