
Abstract
The position of the fibula around the proximal tibia varies in different people; it was therefore hypothesized that this variation would affect the orientation of the lateral collateral ligament and the popliteofibular ligament complex. This hypothesis was studied in 10 cadaveric knees by measuring the orientation and length changes in these structures as the knee was flexed. The data were correlated with tibiofibular joint position. The strength of the ligaments was also tested. There were significant correlations between fibular head position and ligament orientation with the knee extended. The lateral collateral ligament slackened significantly with knee flexion, whereas the popliteofibular ligament complex did not. The structures became significantly steeper in the sagittal plane as the knee was flexed. The lateral collateral ligament passed through vertical at 70° of knee flexion and was thus poorly oriented to withstand tibial external rotation. The lateral collateral and popliteofibular ligaments had tensile strengths of 309 and 186 N, respectively. The popliteofibular ligament is dominant when the knee is flexed, because of the slackening of the lateral collateral ligament, and so it should always be reconstructed. The anatomic variation causes some knees to have better ligament orientations to withstand posterolateral tibial displacements and, conversely, other knees may be inherently more difficult to stabilize by reconstruction.
The posterolateral corner of the knee has a complex and variable anatomy, and the results of reconstructive surgery have been inconsistent. However, there has recently been an increasing awareness of the importance of the structures crossing the posterolateral corner of the knee in providing functional stability. Earlier studies of the posterolateral structures have included detailed anatomic descriptions1,5,7,9,12 and biomechanical evaluation of the strength of the lateral collateral and popliteofibular ligaments. 6 Other researchers have examined the contributions to knee stability made by these structures, in particular to resisting varus (adduction) and external tibial rotations and posterior tibial translation, both singly and in combination.2–4,7,10
One of the factors that makes surgery of the posterolateral corner so difficult, and hence limits its success, is anatomic variability. Watanabe et al. 12 examined the incidence of different posterolateral structures and found a popliteofibular ligament in 94% of 115 knees. Both Watanabe et al. and Hunziker et al. 5 showed that different combinations among the lateral collateral, popliteofibular, arcuate, and fabellofibular ligaments can be encountered in different knees. Surgeons usually reconstruct the lateral collateral, the popliteofibular ligament, or both, depending on their assessment of what has been damaged. Attention is focused on these structures because the lateral collateral ligament is a primary restraint against varus (adduction) angulation, 3 and the popliteofibular ligament against tibial external rotation. 10
To complement studies of the soft tissues, Sugita et al. 8 studied the bony anatomy of the posterolateral corner of the knee by plain radiographs and computed tomography. They reported that the position of the fibula varied around the lateral and posterior aspects of the tibia. Noting this, we hypothesized that the variation of tibiofibular joint position could be correlated to variations in the associated soft tissues that attach to the fibular head, and that this might explain the variable success of reconstructions.
The aim of this study was to examine the knee to try to correlate details of the soft tissues with the variations of the bones to gain greater understanding of how these structures act to stabilize the knee. The specific aim was to check the hypothesis that the orientations of the lateral collateral ligament and of the popliteofibular ligament complex (the popliteus tendon plus popliteofibular ligament) attaching to the fibular head would correlate with different positions of the fibula around the tibia. We also studied how knee flexion affected the orientations of the lateral collateral ligament and popliteofibular ligament complex, measured the patterns of slackening and tightening of these structures during knee flexion, and measured the strength of the lateral collateral and popliteofibular ligaments.
Materials and Methods
This study used 10 frozen cadaveric knees with a mean age of approximately 70 years (not all specimens had age data available). After the specimens were thawed, all tests and measurements were made at room temperature with the tissues protected from dehydration by wrapping in water-soaked tissue paper when this did not interfere with the work. One knee was used to develop the experimental method, and data are presented for the remaining nine. The specimens had been supplied with the skin and fat layer removed and included approximately 120 mm of the tibia and 160 mm of the femur. The knee extensor apparatus and other superficial muscles were removed, leaving the capsular ligaments and associated tissues intact. The knees were prepared for mounting in a measuring fixture by potting the distal tibia along the central axis of a cylindrical stainless steel tube using polymethyl methacrylate bone cement. The proximal fibula was secured in its anatomic position beside the tibia using two 4.5-mm cortical bone screws that passed transversely through the fibula and into the tibia, approximately 25 and 45 mm from the proximal tip of the fibula. The screws stabilized the fibula in the absence of the distal tibiofibular joint from the specimens. The femoral diaphysis was also potted into a steel tube using bone cement. A stainless steel intramedullary rod, 12 mm in diameter by 300 mm long, was cemented into the femur through the base of the pot.
Care was taken when dissecting the lateral aspect of the knees to identify the tissues attaching to the fibular head, especially approaching the popliteofibular ligament, which was usually embedded below variable fascial layers and the arcuate ligament. The lateral collateral ligament, popliteus tendon, and popliteofibular ligament were traced to their bony attachments on the femur and fibula, and these areas were identified. Pins were then driven into the centers of these attachments until the head of the pin was against the bone surface.
The relative positions of the ligament and tendon attachments were photographed at knee flexion angles from 0° to 120°. The tibial pot was secured vertically on a rotating bearing, to allow internal-external rotation. A Nikon F3 camera with 105-mm microNikkor lens (Nikon Corp., Chiyoda-ku, Tokyo, Japan) was mounted horizontally on a tripod 1 meter from the knee. The orientation of the specimen was set before measurements were taken; with the knee held in full extension, the medial-lateral direction was defined as being parallel to the most posterior points of the femoral condyles. These points were identifiable through the thin capsule, and a stainless steel wire, 300 mm long by 3 mm in diameter, was rested on them. The knee was then rotated in the tibial bearing, and the height of the camera adjusted until the wire was end-on when viewed through the camera, at which point the tibial bearing was locked in place. The femoral intramedullary rod could be rested on adjustable stops at known angles of knee flexion. This arrangement did not constrain any secondary movements of the femur as it flexed, and care was taken not to impose any perceptible force as the femoral rod was lowered from one stop to the next. A ruler was hung alongside the knee to provide a vertical datum. Knee flexion was measured using a circular protractor mounted on the femoral intramedullary rod in the sagittal plane, with a hanging pointer. A lateral-medial photograph was taken using color slide film. The distances between the attachments of the lateral collateral ligament and from the femoral attachment of the popliteus tendon to the fibular attachment of the popliteofibular ligament (popliteofibular ligament complex) were measured using dividers located against the pinheads and a ruler (accuracy, ±0.5 mm). Once this had been repeated at 30°, 60°, 90°, and 120° of knee flexion, the tibial mounting plate was rotated through 90° to yield a set of posterior-anterior views in the same way. It was known from prior work, in which a knee had been remounted and photographed another day, that this method gave angular measurements between pairs of points reproducible to ±1°.
To document the positions of the ligament attachments to the fibular head in relation to the tibial plateau, all soft tissues linking the femur to the tibia were divided, leaving the femorofibular attachments intact. The femur was lifted aside and the tibial plateau photographed in a proximal-distal direction while ensuring that the heads of pins in the fibular attachments were visible. The fibula was separated from the tibia, leaving a preparation with the fibula linked to the femur by the lateral collateral ligament and popliteofibular ligament complex.
To document where the tibiofibular joint was located below the tibial plateau, a 1.5-mm wire was drilled into the tibia at the center of the articular surface of the tibiofibular joint, parallel to the tibial shaft, until it emerged through the tibial plateau. The tibial plateau was then photographed.
The color slides were projected onto drawing paper at approximately twice life size, and the centers of the pinheads in the tendon and ligament attachments were recorded. From these, the orientations of the lateral collateral ligament and popliteofibular ligament complex were measured. The position of the tibiofibular joint was defined in degrees of rotation about the geometric center of the tibial plateau, posteriorly from the lateral direction (see Fig. 3).
The relationships between the following variables were examined using linear correlation: the inclinations of the lateral collateral ligament and popliteofibular ligament complex in the sagittal and coronal planes with knee flexion and also with tibiofibular joint position, the lengths of the lateral collateral ligament and popliteofibular ligament complex with knee flexion, and the strength of the lateral collateral ligament with the strength of the popliteofibular ligament complex. Differences of ligament length between one knee flexion angle and another and differences between the tensile properties of the lateral collateral ligament and popliteofibular ligament complex were tested using the Student's paired two-tailed t-test with a significance level of 0.05.
The knees were prepared for testing the tensile properties of the lateral collateral ligament and the popliteofibular ligament complex. To test them separately, the head of the fibula was split longitudinally between their attachments. The halves of the proximal fibula were potted into steel tubes using polymethyl methacrylate bone cement. The bone fragments were completely embedded, with the cement pulled back from around the ligaments before it set. The steel tube containing the femur was fitted into an adjustable fixture on the bed of an Instron 1122 materials testing machine (Instron, Canton, Massachusetts), and the popliteofibular ligament complex pot was placed into a similar fixture on the moving crosshead. The fixtures were adjusted until the popliteofibular ligament complex was aligned with the loading axis of the test machine and the bones were in the correct anatomic relationship. The assembly was then extended to failure at 200 mm/min, with no preconditioning load cycles, and a force-extension graph was recorded. The lateral collateral ligament was then tested similarly. Failure strains were calculated from the lengths measured with the knee fully extended.
Results
Orientation of Ligaments in the Sagittal Plane with Knee Flexion
When the knee was extended, both the lateral collateral ligament and the popliteofibular ligament complex slanted posteriorly as they passed from the femur to the fibula (Fig. 1). The femoral attachments moved posteriorly relative to the tibial plateau with knee flexion. Thus, the inclination of the lateral collateral ligament relative to the anterior-posterior direction in the sagittal plane increased significantly with knee flexion (r 2 = 0.526, P < 0.0001), from 74° ± 3° at 0° of knee flexion to 96° ± 13° at 90° of knee flexion. The lateral collateral ligament passed through vertical at approximately 70° of knee flexion (Fig. 2). The popliteofibular ligament complex behaved similarly; its inclination increased from 49° ± 6° at 0° of knee flexion to 71° ± 12° at 90° of knee flexion (r 2 = 0.624, P < 0.0001) (Fig. 2).
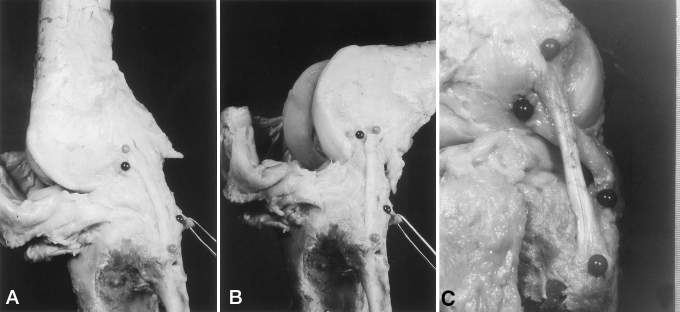
Lateral-medial view of a left knee at 5° (A) and 70° (B) of flexion showing pinheads in the attachments of the lateral collateral ligament (lighter pinheads) and popliteofibular ligament complex (darker pinheads). The popliteofibular ligament fibers (C) descend from the popliteus tendon to the proximal posterior tip of the fibular head.
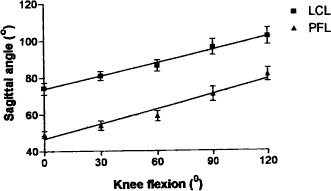
Variation of sagittal plane inclination of the lateral collateral ligament (LCL) and popliteofibular ligament complex (PFL) with knee flexion. The sagittal angle is 0° in the anterior-posterior direction, with values from 0° to 90° indicating a direction tending posteriorly and distally (mean ± 1 SD). The inclination of both structures increased significantly as the knee flexed (lateral collateral ligament: r 2 = 0.526, P < 0.0001; popliteofibular ligament complex: r 2 = 0.624, P < 0.0001).
Relationship between Tibiofibular Joint Position and Soft Tissue Orientation
The tibiofibular joint had a mean position of 26° ± 5° (mean ± 1 SD), range 18° to 33°, around the tibial plateau (Fig. 3). There was a significant correlation between the position of the fibular head around the tibial plateau and the inclination of both the lateral collateral ligament (r 2 = 0.809, P = 0.001) and of the popliteofibular ligament complex (r 2 = 0.525, P = 0.027) in the sagittal plane with the knee fully extended (Fig. 4A). The more posterior the fibular head, the less was the inclination of the ligaments. There was a similar tendency for the inclination of these structures in the coronal plane to reduce as the fibular head was located more posteriorly and medially, but this tendency did not reach significance with the number of knees examined (lateral collateral ligament: r 2 = 0.430, P = 0.055; popliteofibular ligament complex: r 2 = 0.365, P = 0.085) (Fig. 4B).
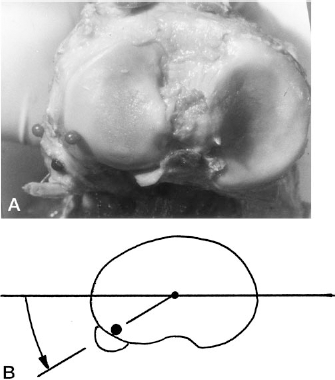
A, view of the tibial plateau of a left knee. The center of the tibiofibular joint is below the pinhead in the tibial plateau. The other pinheads are in the attachments to the fibular head of the lateral collateral ligament (lighter pinhead at extreme left) and popliteofibular ligament (darker pinhead, posteriorly). B, the diagram shows how the position of the tibiofibular joint around the tibial plateau was defined.
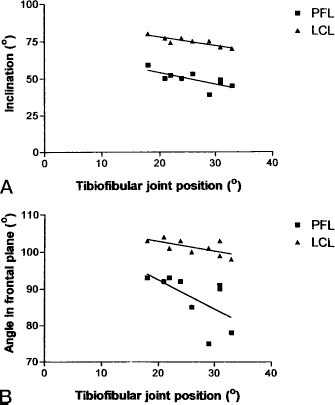
Relationships between the inclinations of the lateral collateral ligament and popliteofibular ligament complex and the position of the tibiofibular joint around the tibial plateau when the knee is extended. A, there was a significant correlation between the position of the fibular head around the tibial plateau and the inclination of both the lateral collateral ligament (r 2 = 0.809, P = 0.001) and of the popliteofibular ligament complex (r 2 = 0.525, P = 0.027) in the sagittal plane. B, in the coronal plane this tendency did not reach significance with the number of knees examined (lateral collateral ligament: r 2 = 0.430, P = 0.055; popliteofibular ligament complex: r 2 = 0.365, P = 0.085).
Relationship between Knee Flexion Angle and Ligament Lengths
The lateral collateral ligament had a mean length (distance between the femoral and fibular attachments) of 59.2 ± 4.3 mm (range, 51.5 to 64) with the knee fully extended, which reduced significantly and the ligament slackened as the knee flexed (r 2 = 0.194, P = 0.002) (Fig. 5). The length at 90° of knee flexion was significantly less than at 0° (P = 0.007). The popliteofibular ligament complex had a length of 42.6 ± 7.3 mm (range, 34 to 51) at full knee extension, and a significant difference as the knee flexed could not be demonstrated with the number of specimens available; the length at 60° of knee flexion was 48.0 ± 3.5 mm and at 90° of knee flexion was 46.6 ± 2.9 mm (r 2 = 0.072, P = 0.252) (Fig. 5).
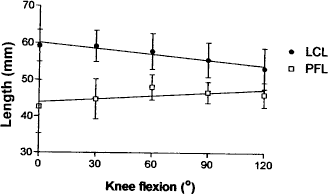
Variation of length (attachment site separation distance) of the lateral collateral ligament and popliteofibular ligament complex with knee flexion (mean ± 1 SD). The lateral collateral ligament slackened significantly as the knee flexed (r 2 = 0.194, P = 0.002), whereas the popliteofibular ligament complex length did not change significantly based on the number of knees tested (r 2 = 0.072, P = 0.252)
Tensile Properties
The lateral collateral ligament sustained a significantly higher failure load than did the popliteofibular ligament complex (P = 0.007) (Table 1), and also a significantly greater elongation to failure (P = 0.0014). The elongations reflected the initial lengths, which were greater for the lateral collateral ligament (Fig. 5), and, therefore, no significant difference could be found for strain to failure (P = 0.978). Similarly, no significant difference could be found for linear stiffness (the slope of the load versus displacement curve after the initial toe region and before nonlinearity due to impending failure) (P = 0.168). No significant correlation could be demonstrated between the failure strengths of the lateral collateral ligament and popliteofibular ligament complex in each knee (r 2 = 0.259, P = 0.244).
Tensile Properties of Lateral Collateral Ligament (LCL) and Popliteofibular Ligament Complex (PFLC)

Discussion
The aim of this study was to gain greater understanding of the function of the posterolateral structures of the knee. It had been noted previously that the position of the tibiofibular joint is variable around the proximal tibia among individual people, 8 and we hypothesized that this variation could be correlated with aspects of the function of the soft tissue structures attaching to the fibular head. For example, it could be envisaged that a relatively posterior placement of the fibular head would cause the lateral collateral ligament and popliteofibular ligament complex to have a less steep angle from the anterior-posterior direction. Thus, they would be more efficiently oriented to withstand posterior displacement of the fibular head in relation to the lateral femoral epicondyle, that is, to resist posterolateral displacement or external rotation of the tibia. Because it was also known that the popliteofibular, arcuate, and fabellofibular ligaments are not always present,5,12 it might also be expected that variations in the skeletal geometry might be related to the different soft tissue structures, perhaps either their presence or bulk.
In this study, we found significant correlations between tibiofibular joint position around the proximal tibia and the orientations of the lateral collateral ligament and popliteofibular ligament complex. The range of tibiofibular joint position was only 15° (18° to 33°) in this study, whereas Sugita et al. 8 showed a greater range of positions in their paper on 671 knees, but they did not measure this. This spread could reflect a difference between the English and Japanese knees studied, but may also reflect the small number of knees available for this study. We infer from our findings that the variable orientation of the tissues will cause some knees, those with a relatively posteriorly placed fibula, to be better able to withstand tibial external rotation loads. Conversely, knees with posterolateral rotatory instability that have a relatively laterally placed fibula may be more difficult to stabilize effectively by reconstruction.
We found significant changes in ligament orientation as the knee flexed. Knee flexion caused the femoral attachments of both the lateral collateral ligament and popliteofibular ligament complex to be carried posteriorly. This was expected, as femoral “roll-back” with knee flexion is well known. The ligament structures therefore became more steeply oriented in relation to the anterior-posterior direction and hence less able to resist posterior displacement of the fibular head (Fig. 6). The lateral collateral ligament passed through vertical as the knee flexed through 70°, so that it was then parallel to the length of the tibia. With greater knee flexion, the lateral collateral ligament reversed its slope and so had no ability to control external tibial rotation without first slackening and re-tightening (Fig. 6). The popliteofibular ligament complex maintained a more efficient orientation for resisting tibial posterior displacement and external rotation than the lateral collateral ligament at all knee flexion angles.
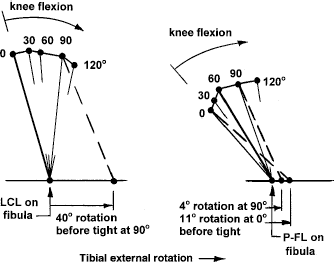
Variation of orientation and length of the lateral collateral ligament (LCL) and popliteofibular ligament complex (P-FL) in the sagittal plane with knee flexion. It is assumed that the fibular attachments are stationary, and the relative displacements of the femoral attachments are shown. The plane of the drawing has anterior to the left, proximal to the top, when the knee is extended. The interrupted lines show the configurations where the ligaments become tight in response to tibial external rotation. The lateral collateral ligament was tight in neutral tibial rotation at 0° of knee flexion, and the popliteofibular ligament complex was tight at 60° of knee flexion, the configurations shown with bold lines.
The distances between the attachments of the lateral collateral ligament and popliteofibular ligament complex were also affected by knee flexion (Fig. 6). The lateral collateral ligament attachment approached the tibial plateau as the knee flexed, and the ligament slackened progressively by 11% at 120° (Fig. 5). Wang et al. 11 found that the lateral collateral ligament slackened by 25% at 120° of knee flexion. Conversely, the femoral attachment of the popliteus tendon moved upward from the tibial plateau as the knee flexed, and the popliteofibular ligament complex remained tight. Watanabe et al. 12 found tightening of the anterior fibers and slackening of the posterior fibers of the popliteus tendon with knee flexion and speculated that a central attachment could be isometric.
The function of the lateral collateral ligament is affected greatly by knee flexion because it is poorly oriented to resist tibial external rotation and is slack when the knee is flexed, whereas the popliteofibular ligament complex retains a reasonable orientation and does not slacken significantly. Some calculations can illustrate these effects. If it is assumed that the ligaments in Figure 6 are at a radius of 50 mm from the axis of tibial external rotation, which is near the center of the knee, tibial rotations before the ligaments become taut can be calculated. This is clearly a simplification but is sufficient to illustrate the point. The popliteofibular ligament complex was just taut where the bone attachments were furthest apart, at 60° of knee flexion, so it resists external tibial rotation within 10° of tibial rotation at other angles of knee flexion. The lateral collateral ligament resists tibial external rotation immediately from neutral tibial rotation at 0° of knee flexion. However, nearly 40° of external tibial rotation is required before it becomes taut at 90° of knee flexion, so the popliteofibular ligament complex is dominant and will rupture before the lateral collateral ligament in this situation.
Because the popliteofibular ligament complex is both tight and well aligned for resisting tibial external rotation at all angles of knee flexion, abnormally increased external tibial rotation at any angle of knee flexion suggests popliteofibular ligament complex damage; the popliteofibular ligament complex is a primary restraint against this motion. 10 Conversely, abnormally increased external tibial rotation at 90° of knee flexion does not mean that the lateral collateral ligament is damaged, because a large external rotation is needed to even bring it to the slack-taut transition point. The lateral collateral ligament is the primary passive restraint to varus tibial rotation (adduction) with the knee extended,2–4 so this test must be applied to check lateral collateral ligament integrity.
The results of this study provide an explanation for data published previously. Veltri et al. 10 found the popliteofibular ligament complex to be a primary restraint to external tibial rotation, and Shahane et al. 7 found that tibial external rotation and varus laxity increased mostly when the lateral collateral ligament was cut with the knee extended and after the popliteofibular ligament was cut at 90° of knee flexion. We found the tensile strength of the lateral collateral ligament and popliteofibular ligament complex to be 309 N and 186 N, respectively, whereas Maynard et al. 6 found them to be 750 N and 425 N. It is possible that the lower strength seen in our study was due to more complete dissection of overlying fascial tissues and not specimen age.
The main limitation of this study was the use of elderly cadaveric joints, and it is important not to extend the implications beyond the passive stabilizing structures, which are not affected significantly by post mortem changes. The ligaments may not have been as strong or as stiff as in a young adult, who would be more typical as a sports injury patient, but young specimens were not available. Data are available for the effect of age on the strength of the ACL, showing that specimens 20 to 30 years of age are 2.5 times stronger than those 70 years of age or older. 13 If this tendency is the same for the lateral collateral ligament and popliteofibular ligament complex, they would have breaking strengths of 773 and 465 N in young adults. In life, the structures studied are affected by active tensions in the popliteus and biceps muscles and the iliotibial tract, and these may affect the contributions of the ligaments linking to the fibular head. The forces applied in this study did not aim to reproduce those imposed during sporting activities, as this was a study of passive knee motion.
This work shows why the popliteofibular ligament complex is important in resisting posterolateral tibial displacements at all angles of knee flexion, whereas the lateral collateral ligament becomes more slack and less well aligned with knee flexion. Although Watanabe et al. 12 did not find the popliteofibular ligament in 6% of the 115 knees examined, we have found it in 25 consecutive joints in this and another study, so it seems, based on our anatomic study, that it would be reasonable to make a popliteofibular ligament complex reconstruction during surgery to correct posterolateral knee instability.