
Abstract
We described histologic changes in patellar tendon autografts that occur over time within the tibial tunnel in specimens harvested from patients undergoing revision anterior cruciate ligament reconstruction. Ten patients, averaging 21.2 years of age, were divided into two groups based on the time period between their original and revision surgery: early revision (less than 1 year, four patients) and late revision (more than 1 year, six patients). Among the early revision group, the tendon within the tunnel showed increased cellularity and random collagen bundles. A specimen from the shortest early revision case revealed a normal original bone-tendon junction, whereas others showed an obscured structure. Between the tendon and the tunnel wall, granulation tissue was seen and the bone-tendon junction was still immature. In the late revision group, the tendon appeared similar to normal ligament. The original bone-tendon junction was not seen, and the tendon continued completely to the tunnel wall with Sharpey-like fibers. Observations in the early revision group suggest that tendon remodeling and bone-tendon integration continue for at least several months after transplantation. The original bone-tendon junction appears to have shifted to the proximal patellar tendon-tunnel wall junction with time. These findings are in agreement with prior animal studies.
During the last 20 years, many studies have been performed regarding the ACL, and, as a consequence, methods for reconstructing the ACL have progressed notably. Recently, the bone-patellar tendon-bone autograft and hamstring tendon autograft have been accepted as the standard graft materials. The outcome of these biologic ACL graft materials depends on numerous mechanical factors, such as the mechanical property of the graft,18,27 positioning of the graft,8,10,17 fixation method,6,14 and initial tension of the graft,28,29 as well as histologic factors. The histologic structure of the articular portion of graft materials has been evaluated extensively,1,11,13,15,16,23,25 but there is little knowledge about the equally important graft incorporation to the bone tunnel, especially in humans. 21
The bone-patellar tendon-bone graft in ACL reconstruction has several advantages: it is the strongest of all biologic substitutes, 18 achieving strong initial graft fixation using Kurosaka interference screws 14 and rapid biologic bone-to-bone fixation. 18 It also has several disadvantages: one is the space between the tendinous portion of the graft and the tunnel wall, because the tendinous portion is always longer than the normal ACL. 25 This space may unfavorably affect knee stability 25 and prolong tendon-to-bone healing proximal to the bone plug of the graft. Also, this space is considered to be the cause of tunnel enlargement after ACL reconstruction because it permits windshield-wiper motion of the graft within the tunnel and synovial fluid infiltration into the tunnel. 26 The purpose of this study was to describe the histologic changes that occur over time in the bone-patellar tendon-bone autograft within the tibial tunnel using specimens harvested from patients undergoing revision ACL reconstruction and to compare these findings with those of prior studies.
Materials and Methods
Ten patients (four men and six women) with an average age of 21.2 years (range, 16 to 26) were included in this study (Table 1). All of their original reconstructions were performed with bone-patellar tendon-bone autograft fixed by interference screws. Causes of revision surgery included reinjury from sports-related activity or trauma (50%), technical failure of the original reconstruction for reasons such as anterior placement of the femoral tunnel (20%), and unknown reasons (30%). The mean period from the original reconstruction to revision surgery was 2 years and 10 months. Four patients in this series underwent revision surgery within 1 year of the original surgery (average, 6.25 months) and were included in the early revision group. The cause of revision surgery in all of the early revision group patients was reinjury. The other six patients underwent revision surgery more than 1 year after the original surgery (average, 4 years and 4 months) and were included in the late revision group. The choice of 1 year as the cutoff between the early and late revision groups was decided on the basis of data from prior histologic studies of specimens obtained by arthroscopic methods.1,11,13,16,23,25 All patients were involved in recreational or competitive sports (Table 1).
Characteristics of Patients and Bone-Patellar Tendon-Bone Grafts a
–, not identified; ±, obscured or partially identified; +, normal or nearly normal; + +, increased.
Harvest of Specimens
All revision ACL reconstructions were performed using hamstring tendons (semitendinosus and gracilis tendons) with the EndoButton (Acufex Microsurgical, Mansfield, Massachusetts) technique. After removal of the interference screws used in the original surgery, the tibial bone tunnel was made using a coring reamer as described by Pinczewski et al. 21 In this series, none of the cases had eccentric tibial tunnel placement in the original operation. The harvest technique allowed for biopsy of the tendinous portion of the bone-patellar tendon-bone autograft within the tunnel and from the tendon-bone interface in the harvested bone core.
Histologic Examination
The specimens were fixed in 20% formalin after biopsy. The bones then were decalcified using Plank-Rychlo solution and were embedded in paraffin. Specimens from the tibial bone tunnel were cut longitudinally into 5 μm thick sections. These sections were stained with hematoxylin and eosin and were examined under a light microscope with or without compensated polarization (AHBS, Olympas Optical Co., Tokyo, Japan). In the tendinous portion within the tunnel, a qualitative evaluation of the cellularity, vascularity, collagen organization, and crimp pattern was made. The original bone-tendon junction of the graft and the newly formed interface between the tendon and the tunnel wall were also evaluated. A pathologist (TK) who did not know the history of these patients evaluated all specimens.
Results
Gross examination of the tendinous tissue revealed a white fibrillary structure with an avascular appearance in the harvested bone core in all 10 cases. The bone plug of the graft was not seen macroscopically in any of the cases because it was well incorporated into the surrounding bone.
Early Revision Group
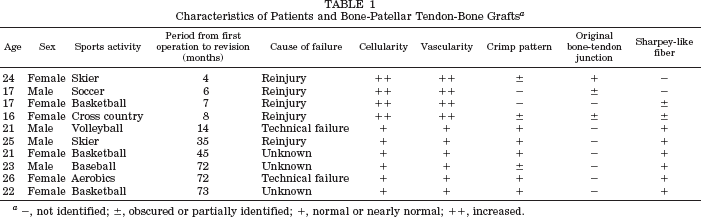
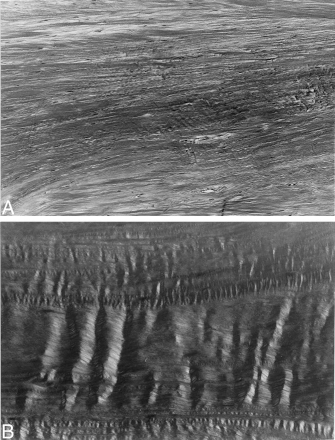
The tendinous portion within the tunnel evidenced increased cellularity and vascularity in all of the early revision patients (Fig. 1, A through C). Graft necrosis was not identified in any of the early revision patients. In the two patients with the shortest time interval between the original procedure and the revision (4 and 6 months), nuclei in most of the increased cells were round and randomly oriented (Fig. 1, A and B). In the other two patients in this group, who had a longer time interval between the original procedure and revision, the nuclei were predominantly spindle shaped (Fig. 1C). The orientation of the collagen bundles showed a relatively random pattern and did not demonstrate a uniform sinusoidal crimp pattern under polarized microscopy (Fig. 1D).
The tendinous portion within the tunnel in the early revision group seen under routine light microscopy and polarized microscopy (longitudinal section; H&E; original magnification, ×25). A, specimen from a patient taken 4 months after the original operation (the shortest time interval in this study) shows the collagen bundle orientation with a relatively regular pattern and round nuclei increased among these bundles. B, this specimen, from a patient whose time interval between the original procedure and the revision was 6 months, showed that nuclei in most of the increased cells were round, and collagen bundles were randomly oriented. C, in a patient with an 8-month time interval, nuclei were predominantly spindle shaped. D, collagen bundles did not demonstrate a uniform sinusoidal crimp pattern under polarized microscopy in a patient with a 7-month interval.
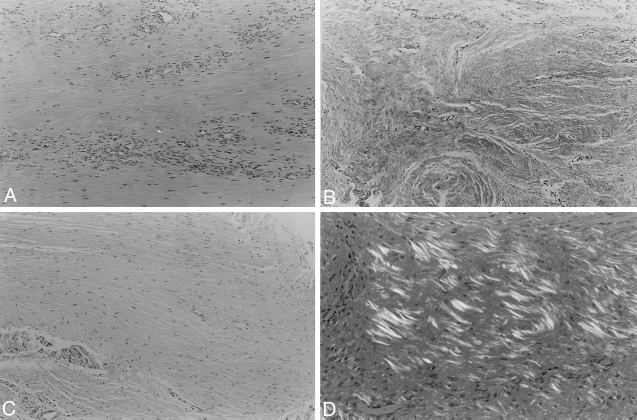
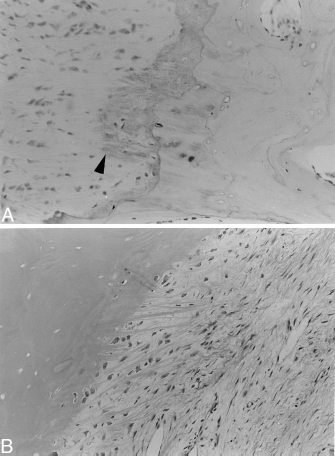
Microscopically, the original bone-tendon junction of the graft was found in three of four patients. The patient with the shortest time interval between the original procedure and revision (4 months) showed a normal bone-tendon junction with four distinct zones and an apparent tidemark (mineralization front) (Fig. 2A). In two other early revision patients (6 and 8 months after the original operation), the original bone-tendon junction was identified, but its structure was obscured (Fig. 2B). Granulation interface tissue was seen between the tendon and the tunnel wall in all four cases (Fig. 3A), and these were considered immature bone-tendon junctions. Although Sharpey's fibers were not identified with the polarized light microscope, the interface tissues were oriented to the collagen bundles within the tunnel (Fig. 3B).
The original bone-tendon junction of the bone-patellar tendon-bone graft in the early revision group seen under routine light microscopy (longitudinal section; H&E; original magnification, ×50). A, specimen from a patient taken 4 months after the original operation (the shortest time interval in this study) showed a normal bone-tendon junction, with four distinct zones and an apparent tidemark (arrowhead). B, in this specimen from a patient whose time interval between operations was 6 months, the original bone-tendon junction was identified, but its structure was obscured.
Newly formed structure between the tendon (T) and bone tunnel wall (W) in the early revision group under routine light microscopy and polarized microscopy (longitudinal section; H&E; original magnification, ×50). A, in all of the early revision patients, granulation interface tissue (I) was seen, which was considered to be an immature bone-tendon junction. B, under polarized light microscopy, Sharpey's fibers were not identified, although collagen continuity was identified between the tendon and the surrounding tunnel wall.
Late Revision Group
In the tendinous portion within the tunnel, both cellularity and vascularity decreased until they were similar to that of normal ligament tissue (Fig. 4A). Graft necrosis was not identified in any of the late revision cases. Nuclei of fibroblasts showed a more uniform spindle-shaped appearance. Relatively mature longitudinally oriented collagen bundles were seen in all late revision cases. Polarized microscopic examination also showed relatively uniform sinusoidal crimp patterns, but these were not identical to those in the native ACL (Fig. 4B). These findings were similar among all patients in this group, regardless of the wide range of time between the original surgery and revision surgery (1 year and 2 months to 6 years and 1 month).
The tendinous portion within the tunnel in the late revision group seen under routine light microscopy and polarized microscopy (longitudinal section; H&E; original magnification, ×25). A, both cellularity and vascularity decreased until they were similar to that of normal ligament tissue. Fibroblast nuclei showed a more uniform spindle-shaped appearance. B, the polarized microscope also showed relatively uniform sinusoidal crimp patterns, but they were not identical to those in native ACL.
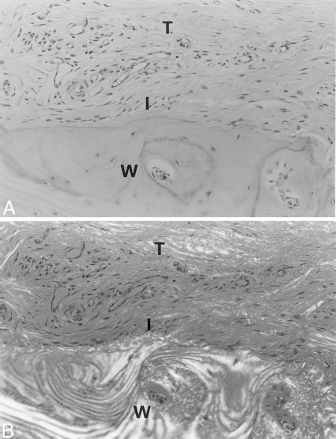
Microscopically, the original bone plug of the graft was not found in any of the late revision cases and therefore could not be evaluated. The granulation tissue, which was seen between the tendon and tunnel wall in the early revision group, was replaced by a thin transitional fibrous tissue, and the tendinous portion of the graft was completely adherent to the tunnel wall (Fig. 5A). The fibrous tissue showed orientation in the direction of the collagen bundles of the tendon within the tunnel. Four distinct zones and tidemarks were observed, but they were not as apparent as the normal bone-tendon junction of the graft. The Sharpey-like fibers were identified in all late revision specimens with polarized light microscopy (Fig. 5B).

The junction between the tendon (T) and tunnel wall (W) in the late revision group under routine light microscopy and polarized microscopy (longitudinal section; H&E; original magnification, ×50). A, a thin transition fibrous tissue replaced the granulation tissue, and the tendinous portion of the graft was completely adherent to the tunnel wall. Four distinct zones and tidemarks were observed (arrowhead), but they were not as apparent as in a normal bone-tendon junction of bone-patellar tendon-bone graft. B, the Sharpey-like fibers were identified in all late revision cases with polarized light microscopy.
Discussion
The maturation process of the graft substitute in the joint has been extensively studied in animal models. Several studies have shown that patellar tendon grafted for ACL reconstruction undergoes central degeneration at 2 to 6 weeks after surgery and changes into a structure similar to that of the native ACL between 6 and 12 months after surgery.2–5,7 Goradia et al. 9 reported the histologic structure of the intraarticular segment of a hamstring autograft used for ACL reconstruction in a sheep model and showed that the hamstring autograft also comes to resemble the ACL over the initial year after surgery. They did not find graft necrosis at any time period. Shino et al. 24 performed ACL reconstruction using an allogenic tendon graft in the dog and reported that grafted allogenic tendons adapt themselves to the normal ACL through the process of ischemic necrosis, revascularization, and gradual remodeling.
In clinical studies, these maturation processes were evaluated by biopsy using an arthroscopic technique.1,11,13,16,23,25 Abe et al. 1 evaluated the remodeling process of autogenous patellar tendon graft by means of light and electron microscopic examination. Their results with ultrastructural study suggest that grafts are still immature at 1 year, even if microscopic examination shows gross similarity to the original ACL. Rougraff et al. 23 also reported histologic analysis of human patellar tendon autograft. They concluded that the grafts are viable as early as 3 weeks postoperatively and may not go through a necrotic stage. They also progress through a prolonged process of “ligamentization” that takes as long as 3 years to complete. In contrast, Johnson 12 performed an arthroscopic biopsy of semitendinosus tendon grafts and reported that these grafts appeared histologically similar to the native ACL as early as 4 months after reconstruction. Horstman et al. 11 reported histologic changes in allografts used for ACL reconstruction. There was a progressive decrease in cellularity and vascularity as the allograft matured, but the maturation process was still ongoing 20 months postoperatively.
One of the limitations of these clinical studies was that the biopsy was performed in small focal areas, without examining the entire graft, as would be done in an animal model.2–5,7,9,24 This problem may be one of the reasons why these clinical data partially differed. Regardless, these ligamentization processes showed similar changes among graft substitutes and among species. Rougraff et al. 23 identified four stages of ligamentization after reconstruction: repopulation, rapid remodeling, maturation, and quiescence. Unfortunately, we could not distinguish the four distinct stages of ligamentization clearly because this study was not a prospective study. However, similar processes in the tendinous portion of the graft within the tunnel were observed in this study. The early revision group showed stages of repopulation and rapid remodeling, and the late revision group showed stages of maturation or quiescence. These results indicate that tendon grafted within the bone tunnel progressed through the same process as that in the articular portion of the graft. However, the fact that the patient with the shortest time before revision still showed the repopulation stage at 4 months after the original reconstruction (Fig. 1A) may suggest that this process progressed more slowly than that in the articular portion.
Although it is important to know about the maturation process of the ligament substitute, knowledge of the integration process of the bone-tendon junction is also important for planning postoperative rehabilitation. 22 However, few studies have investigated the healing of ligament to bone, especially in the human, because harvest of the articular portion of the graft is easy using an arthroscopic technique, whereas harvest of the bone-tendon junction is truly difficult. 21 Pinczewski et al. 21 examined the histologic findings from the bone-tendon junction of two specimens retrieved from patients undergoing revision surgery at 12 and 15 weeks after reconstruction. Although there were collagen fiber continuities between bone and tendon, those interface tissues were still thick and seemed to be immature. This histologic finding agrees with ours seen in the early revision group (Fig. 3, A and B). We believe that bone-tendon integration is still ongoing for at least several months. Because there was no difference between the results seen by Pinczewski et al. and ours, the space between the tendinous portion of the graft and the tunnel wall may not affect bone-tendon integration in ACL reconstruction.
There are several experimental studies that show the integration process of the bone-tendon junction.19,20,22,24 Shino et al. 24 reported that allogenic patellar tendon attached to the bone after 30 weeks in dogs. Rodeo et al. 22 observed in a dog model that the biologic fixation of a tendon inside a bone tunnel occurs by the formation of Sharpey-like fibers, and all pullout tests resulted in graft slippage from the clamp or graft rupture by 12 weeks. These results imply that the tunnel-graft interface was no longer the weakest link. Panni et al. 19 showed that a complete bone-ligament junction having four distinct zones was formed after 16 weeks in a rabbit model. In these animal studies, the integration process of the bone-tendon junction was more rapid than was seen in our patients. This may be because most of the animal studies were performed in immature animals, which have faster healing potential.
Recently, Panni et al. 20 compared two different types of reconstruction with bone-patellar tendon-bone graft in a rabbit model and showed that the remodeling process occurs more dramatically when the original bone-tendon junction was placed inside the bone tunnel, as in the outside-in technique. They concluded that the original bone-tendon junction is partially unloaded and undergoes a modification of its morphologic structure as a function of the distribution of the loads to which the graft is subjected inside the tunnel. In our study, we observed similar morphologic changes in the early revision group. The shortest revision case had a normal bone-tendon junction with an apparent tidemark, whereas in the other early revision cases the original bone-tendon junction was identified, but its structure was obscured. Although one advantage of bone-patellar tendon-bone graft is the ability to obtain biologic fixation at the bone plug level, the ligament-tunnel wall interface proximal to the bone plug develops fixation postoperatively. We found that the space between the patellar tendon and the tunnel wall did not unfavorably affect bone-tendon healing.
As far as we know, this is the first study observing graft incorporation within the bone tunnel in a series of patients. However, this study had several limitations. One was that there were not enough cases to evaluate the complete maturation process of the graft, as would be done in animal prospective studies. Because no specimen was examined at less than 4 months after the original operation, there was a lack of information about the initial remodeling stage. Another limitation was that all specimens were retrieved from revision patients. Harvest of specimens during revision surgery is considered to be the best way or, indeed, the only way to observe a bone-tendon junction in the human. However, these conditions likely affected the biopsy results. Reinjury, elongation of the graft, or both, which were the reasons the revision surgeries were needed, unload the stress into the ligament and bone-tendon junction within the tunnel and may influence their morphologic characteristics. In this study, we could not find any differences in the morphologic characteristics of the graft among the patients whose revision was performed for different causes, such as reinjury or technical failure.
In spite of these limitations, we believe that the results of this study demonstrate the maturation process of ligament within the tunnel and graft incorporation to the bone tunnel in the human. The ligament maturation within the tunnel progresses similarly to that in the articular portion of the graft, as seen in both animal and human studies. Observations of graft incorporation into the bone tunnel seen in this study are in agreement with those seen in previous animal studies. We conclude that the bone-tendon junction of the reconstructed ACL is shifted from the original bone-tendon junction of the graft to the proximal patellar tendon-tunnel wall junction with time, as Panni et al. 20 described. Further study is required to confirm this healing process within the tunnel, especially in human ACL reconstructions using hamstring tendon, in which most of the bone tunnel is occupied with soft tissue and the success of reconstruction relies on the firm healing of tendon to bone.