
Abstract
Cyclops syndrome has been defined as a loss of knee extension due to impingement of a pedunculated proliferative tissue mass after anterior cruciate ligament reconstruction. We describe four patients who were operated on for progressive loss of knee extension after minor knee injury. During the arthroscopic procedure, the consistent finding was a fibrous pedunculated nodule adhering to the anterolateral aspect of the original anterior cruciate ligament, obstructing extension by impingement in the anterior aspect of the knee. At least part of the anterior cruciate ligament was intact in all cases. These patients were compared with seven patients who developed cyclops syndrome after anterior cruciate ligament reconstruction. Clinical and arthroscopic findings were the same in both groups. An arthroscopic excision of the nodule, performed an average of 12 weeks after knee trauma or after reconstruction, gave very good results. Histologic examination of the excised nodules from both groups showed fibroelastic connective tissue proliferation, thromboangiitis, and areas of necrotic bone and foreign body giant cell granuloma. On the basis of our observations, we conclude that formation of a fibrous pedunculated nodule may occur after an anterior cruciate ligament injury as well as after surgical reconstruction of the anterior cruciate ligament.
Jackson and Schaefer 11 first defined the cyclops syndrome in 1990 as a loss of extension after ACL reconstruction due to a pedunculated nodule of fibrovascular proliferative tissue arising from an ACL graft. The nodule was named because of its arthroscopic appearance resembling an eye. They thought it was caused by bone and cartilage residues remaining in the joint after tunnel drilling. Later, different authors proposed various other causes, and a multifactorial cause was suggested (Refs. 3, 4, 15; V. Chassaing, unpublished data, 1994).
In published studies, the cyclops syndrome has been reported as a complication of ACL reconstruction with use of the patellar tendon,1,6–9,11,12,14,15,17,19,20,22 hamstring tendons, 5 fascia lata, 10 and even the Leeds-Keio (Dacron) scaffold, 3 or as a complication after total knee replacement. 18 Delincé et al., 4 however, reported on three patients who already had a nodule at the time of ACL reconstruction but lacked the typical symptoms. In four cases reported by McMahon et al., 16 a cyclops nodule was responsible for diminished knee extension after ACL rupture.
In a previous article we described a patient who developed the symptoms of a cyclops syndrome, associated with the characteristic arthroscopic and histologic findings, after a partial ACL rupture not treated by surgical reconstruction. 21 In the current article, we describe a series of patients with progressive loss of extension after ACL injury without reconstruction. The morphologic and histologic characteristics of the lesion that they had was compared with those of patients who had cyclops syndrome after ACL reconstruction.
Materials and Methods
From January 1994 through December 1998, 127 patients were operated on at the Medical Centre in Ljubljana for lack of extension after an acute traumatic event. In four of the patients (3.1%) with partial rupture of the ACL, a pedunculated nodule was found in the anterior part of the intercondylar notch, preventing extension by impinging between the anterior aspect of the tibia and the roof of the intercondylar notch. In four other patients (3.1%), the cause of the extension deficit was diffuse fibrous proliferation. In 83 patients (65%), the locking was caused by an incarcerated meniscus. Three patients (2.4%) had an osteochondral fragment and 33 (26%) had no identifiable mechanical cause of extension loss. Sixty-nine patients (54%) had medial meniscal tears and 14 (11%) had lateral meniscal tears.
The 4 patients with loss of extension due to impingement of a pedunculated nodule after knee injury were compared with 7 patients of 232 (3%) who underwent ACL reconstruction during the same period and developed cyclops syndrome. The clinical course, arthroscopic appearance, and histologic findings were compared in both groups of patients. Conventional histologic and immunohistologic examinations were performed.
Results
Men were in the majority (75%, 3 of 4) in the acute injury group, whereas in the ACL reconstruction group, women predominated (71%, 5 of 7). The average age was comparable in both groups: 24 years (range, 17 to 38) in the injury group and 23 years (range, 19 to 38) in the reconstruction group. The average interval between ACL reconstruction and the second-look arthroscopic procedure in the reconstruction group was 13 weeks (range, 11 to 15). In the four injury patients, the arthroscopic procedure and the nodule dissection were performed within 10.5 weeks (range, 9 to 13) after injury.
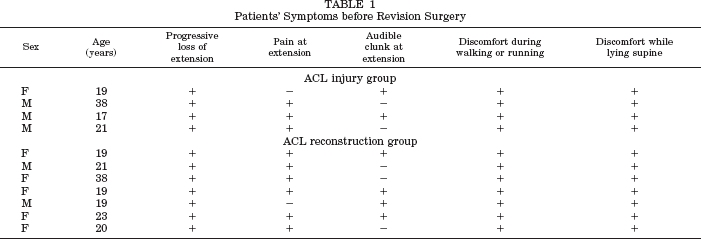
All of the patients in both groups reported progressive loss of extension and discomfort when lying supine and while walking or running (Table 1). Of the injury group, 75% felt discomfort or pain at extension, as did 86% of the reconstruction group; 50% of the injury group and 57% of the reconstruction group reported an audible clunk at extension. The average extension deficit in the knee was 11° (range, 5° to 15°) in the injury group and 11.5° (range, 5° to 20°) in the reconstruction group. Physical findings before revision surgery are listed in Table 2. The radiographs of patients in the injury group were normal, and an analysis of the radiographs made after reconstruction showed a good position of the tibial and femoral tunnels in all seven cases in the reconstruction group. The indication for a revision operation in all cases in both groups was a progressive extension deficit.
Patients’ Symptoms before Revision Surgery
Patients’ Physical Findings before Revision Surgery
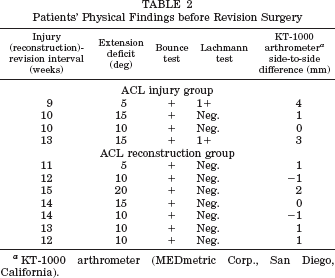
KT-1000 arthrometer (MEDmetric Corp., San Diego, California).
The consistent arthroscopic finding was a white nodular polypoid fibroelastic tumor with a focal bluish transparency resembling a blue eye, varying in size from 5 × 8 mm to 15 × 20 mm. In all the patients, the pedunculated nodule adhered to the anterolateral aspect of the graft or original ACL (Fig. 1). In all of the injury patients, the majority of the ligament was intact. In two (29%) of the patients in the ACL reconstruction group, the fibrous nodule was associated with diffuse fibrous proliferation in the anterior part of the joint. We found no arthroscopically detectable graft impingement in the reconstruction group.
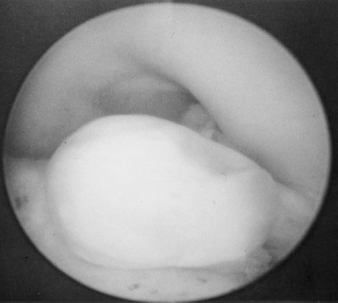
Arthroscopic view of the cyclops nodule in the intercondylar notch of the femur occurring after partial rupture of the ACL.
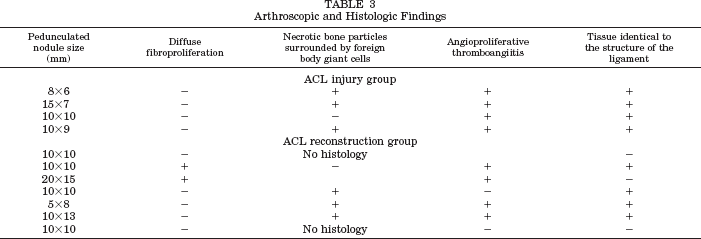
Histologic specimens were available from 9 of 11 patients (82%), all of whom had similar findings (Table 3). The histologic studies in both groups showed proliferation of dense fibroelastic connective tissue, partially covered with a monolayer of flat cells resembling synoviocytes. The connective tissue was identical in structure to the graft or ligament. In cross section, dark brown hemorrhagic areas were seen in the middle of the fibrous proliferation, with the nutritive vessel stem running to the periphery of the tumor. In three of the injury patients and in three of the reconstruction patients, we found focally disseminated regions of tiny amorphous particles of necrotic bone surrounded by foreign body multinuclear giant cells (Fig. 2 and Table 3). Areas of extravasated erythrocytes surrounded the newly formed nutritive vessels as a consequence of thromboangiitis. Angioproliferative thromboangiitis was seen in all patients after ACL injury and in four patients of the ACL reconstruction group. The affected vessels that were still free of thrombosis showed extreme dilatation and extravasation of erythrocytes and macroscopically resembled a blue eye. The rest of the affected vessels were dilated and totally or partially obliterated by organized thrombi or parietal thrombosis with deposition of fibrin into the lumen and destroyed vessel walls. Except for the nutritive vessels visible in cross section, no other newly formed vessels were seen.
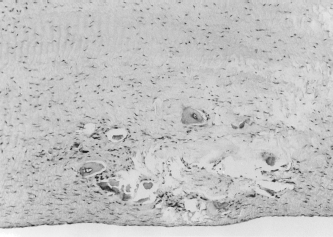
Histologic picture of a cyclops lesion after partial rupture of the ACL. Particles of necrotic bone were surrounded by foreign body giant cells.
Arthroscopic and Histologic Findings
After removal of the nodule, full range of motion was restored in all but two patients. Six months after removal of the nodule, the patients of both groups had no pain at terminal extension. During the final follow-up examination, on average 26 months (range, 8 to 32) after the operation, only the two patients in the reconstruction group who had diffuse disorganized hypertrophic tissue in the anterior part of the joint had an extension deficit of 5°. None of the patients reported pain at terminal extension or instability, and all were able to resume their previous activities. No significant differences in the clinical findings, arthroscopic appearance, histologic picture, or treatment outcome were found between the two groups.
Discussion
Jackson and Schaefer 11 described the cyclops syndrome lesion as a mass of dense fibrous connective tissue rich in newly formed vessels, with the presence of cartilage, newly formed bone tissue, and necrotic lamellar bone. In their opinion, the nodule was caused by bone and cartilage residues remaining in the joint after tunnel drilling. Chassaing (unpublished data, 1994) observed a decline in the incidence of the cyclops syndrome after he introduced thorough debridement of the paratenon and infrapatellar fat pad residues from the bone-patellar tendon-bone graft. Marzo et al. 15 suggested that the irritating stimulus due to the contact between the graft and the intercondylar notch might induce an inflammatory response with the production of granulation tissue. Delcogliano et al., 3 finding no cartilaginous tissue or necrotic bone lamellae within the lesion, concluded that microtrauma and micromotion between the bone rim of the tibial tunnel and the graft might be responsible for the formation of granulation tissue and the resulting nodule. Finally, Delincé et al. 4 proposed a multifactorial cause based on the histologic findings.
The histologic findings in our group of patients who developed the syndrome after ACL reconstruction were similar to those observed by other authors, and they support the multifactorial origin theory. However, the same symptoms, along with similar arthroscopic and histologic findings, also occurred in our acute injury group. Therefore, surgical reconstruction of the ACL is not the only condition in which the cyclops syndrome develops. In three of the four patients with acute ACL injuries, histologic studies revealed regions containing particles of necrotic bone close to the tumor periphery. These findings suggest that partial avulsion of the proximal bony insertion of the ligament, resulting in the presence of small bone particles, may have contributed to the development of the lesion. In the patient in whom no necrotic bone particles were found, trauma to the ligament fibers, along with the reparative inflammatory process and the fibroproliferative reaction of the vital tissue, may have been responsible for the onset of the localized form of fibrous proliferation. In the four patients with cyclops lesion formation after a partial ACL tear, there was no possible impingement, 15 no microtrauma, and no micromotion between the bone rim of the tibial tunnel and the graft that could be responsible for the formation of granulation tissue and the resulting nodule. 3 In addition, there was no possibility of bone and cartilage residues remaining in the joint after tunnel drilling 11 ; therefore, in our opinion, injury to the ligament and the reparative processes occurring as a reaction of the vital tissue are the main triggering factors for the process of cyclops nodule formation. Other factors may promote the process, but they are not indispensable.
It is clear from the results of our series and from those of other reports that the cyclops syndrome, as a localized form of fibrous proliferation, carries a favorable prognosis (Refs. 3, 4, 6–9, 11–17; V. Chassaing, unpublished data, 1994). No recurrence was observed after dissection of the nodule when this was the only cause for the loss of extension. Almost all such patients in our series regained full range of knee motion after the operation. Recurrence from other causes of arthrofibrosis is common. In cases where impingement or misplacement of the graft combined with hypertrophy of the graft are the possible causes of diminished knee extension, the motion is never restored to normal by resection of the fibrous proliferative mass alone.
Conclusions
On the basis of the results of this study and of others reported in the literature, we believe that damage to the ligament is responsible for the development of a cyclops nodule after ACL injury or reconstruction. Other factors may promote fibrous nodule formation, but they are not indispensable. The cyclops syndrome is a condition in which a solitary nodule is responsible for the gradual postoperative or posttraumatic loss of extension. The condition is associated with typical symptoms and a very good prognosis. A clear distinction should be made between the cyclops syndrome and other causes of loss of extension in which the prognosis is uncertain. A fibrous nodule should be suspected in cases of progressive loss of extension after ACL reconstruction as well as after ACL injury, and we suggest that the condition be called cyclops syndrome in both cases.