
Abstract
The aim of this study was to assess the presence of tuberculum intercondylare tibiae tertium, also known as Parsons' knob, and to determine its prominence. Knee radiographs of 171 patients operated on for anterior cruciate ligament injury were examined. The control group included 120 sex- and age-matched patients who underwent orthopaedic examination for knee pain, in whom anterior cruciate ligament injury was ruled out. Knee radiographs revealed the presence of tuberculum intercondylare tibiae tertium in 55 (32.2%) and 16 (13.3%) patients from the study and control groups, respectively. The between-group difference was statistically significant. The authors developed their own method of tuberculum intercondylare tibiae tertium measurement using proportional coefficients based on the length of the tibial plateau to compare the values of the tuberculum intercondylare tibiae tertium. The results showed tuberculum intercondylare tibiae tertium to be not only more common but also more pronounced, especially in height, in the patients with anterior cruciate ligament lesions.
There are numerous reports in both the classic and the most current orthopaedic and sports medicine literature on the significance of ACL injury as well as the diagnostic and therapeutic procedures for treatment of such injury. Any contribution to improve either the diagnosis or the treatment, and especially the prevention, of ACL injury is welcome and useful socioeconomically. Based on our long-standing clinical experience and studies performed in a representative sample, we found that in the adult population with ACL injury, tuberculum intercondylare tibiae tertium could be radiologically identified more frequently than in a normal population without ACL injury.
In 1906, describing in detail the anatomic particularities of the tibial plateau, Parsons 6 pointed to the existence of a small bony prominence located anterior to the medial tibial prominence, medial from the anterior horn of the medial meniscus. In honor of the author, the formation was named Parsons’ knob. In 1937, Politzer and Pick 7 described the same structure using the term “tuberculum intercondylare tertium,” which was thereafter adopted in radiologic practice. It was only in 1974 that Jacobsen 3 stated that the two structures were identical but differently named anatomic formations and proposed the term “Parsons’ tubercle.”
In pronounced cases, the anteromedial fibers of the ACL and anterior horn of the medial meniscus insert onto the tuberculum intercondylare tibiae tertium. Parsons himself suggested that the occurrence of this bony eminence might be an osseous response to a permanent traction load produced by the ACL fibers. In his 1993 article, Berg 1 advocated this line of reasoning, quoting the experimental study of Noyes et al. 5 from 1974, which asserted that this bony prominence of the tibial plateau develops as a response of the body to a frequent and low force-induced, primarily traction, load on the ACL. Berg concluded that the presence of tuberculum intercondylare tibiae tertium may be of considerable clinical relevance. By identifying the junction of the ACL anteromedial fibers and the anterior horn of the medial meniscus, the tuberculum intercondylare tibiae tertium greatly facilitates orientation in ACL reconstructive procedures.
Despite the possibilities offered by MRI analysis of the ACL-anteromedial fiber junction and of tuberculum intercondylare tibiae tertium, the lateral radiographic projection of the knee should be given preference for fast and efficient diagnosis of tuberculum intercondylare tibiae tertium, as demonstrated in 1981 by Danzig et al. 2 in their radiologic studies on anatomic preparations. In a retrospective review of 30 contralateral normal lateral knee radiographs in patients who had ACL surgery, Berg 1 found that 3 patients (10%) had radiologic evidence of a Parson's knob. Jacobsen 3 examined 75 macerated specimens, and 11% had a knob that was so large that Jacobsen used the term “Parson's tubercle.”
The present study was stimulated by the authors’ observation of a higher frequency of tuberculum intercondylare tibiae tertium in patients operated on for ACL injury. The aim of the study was to determine the prevalence of this anatomic formation in patients with ACL injury compared with a control group of patients without ACL injury, and to assess the characteristics (height and length) of the tuberculum intercondylare tibiae tertium employing our own method of measurement using proportional coefficients relative to tibial size.
Materials and Methods
The study group included 171 patients operated on for ACL injury at the Department of Orthopaedic Surgery of the Zagreb University School of Medicine during the period from 1992 through 1995. There were 147 men and 24 women ranging in age from 17 to 47 years (mean, 28). The control group consisted of 120 patients, 101 men and 19 women ranging in age from 17 to 45 years (mean, 27.5) who were treated for anterior knee problems.
Lateral radiographs of the operated knee were analyzed by all three authors independently (two orthopaedic surgeons and one radiologist) and compared with those obtained in the control group of patients. There was an equal proportion of right and left knees in the study and control groups. In cases of a positive tuberculum intercondylare tibiae tertium finding, our original method of measurement, involving the use of a coordinate system with two parallel and four vertical lines, was used to measure the length of the tibial plateau and the length and height of the tubercle (Fig. 1).
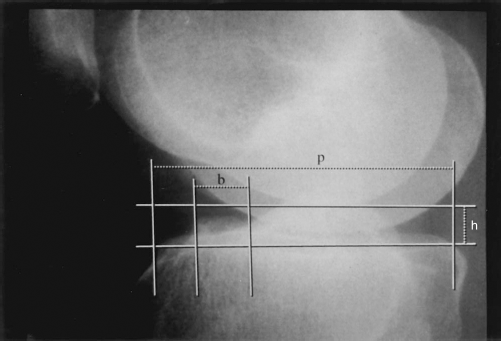
Our method of measurement by use of a coordinate system: p, length of the tibial plateau; b, length of tuberculum intercondylare tibiae tertium base; h, height of tuberculum intercondylare tibiae tertium.
Because the radiographs differed according to film dimensions and central ray dispersion, the absolute figures obtained by the measurement were not comparable. Therefore, a system of comparison of proportional values, that is, coefficients, was used. The coefficients were identical for all radiographs, and their values were independent of the film type and technique used since they determined the size of the tuberculum intercondylare tibiae tertium according to the proportionality of its height and base relative to the tibial plateau.
Three indices of proportionality were calculated: tuberculum intercondylare tibiae tertium height to base (h:b) ratio, tuberculum intercondylare tibiae tertium height to tibial plateau length (h:p) ratio, and tibial plateau length to tuberculum intercondylare tibiae tertium base (p:b) ratio. The parameters were tested by the chi-square test of proportion for single sample, the chi-square test for independent samples, the Student's t-test for independent samples, and the nonparametric Mann-Whitney test for independent samples. Statistical analysis was performed on a personal computer using SPSS software (SPSS, Inc., Chicago, Illinois).
Results
Radiologic positive findings of tuberculum intercondylare tibiae tertium were recorded in 55 (32.2%) patients from the study group and 16 (13.3%) patients from the control group. The difference between the two groups was statistically significant (P < 0.001). There was no statistically significant sex difference in positive results in either group. Testing of differences in the coefficients of proportionality in the two groups is presented in Table 1. The h:b and h:p indices showed statistically significant differences between the study and control groups, indicating that the finding of tuberculum intercondylare tibiae tertium was not only more common in patients with ACL injury but was more pronounced, that is, of a greater height and a longer base as compared with tuberculum intercondylare tibiae tertium found in the control group. Based on our studies and measurements, the shape of the tuberculum intercondylare tibiae tertium was classified into three main types: cone-shaped, dome-shaped, and plateau-shaped (Fig. 2).
Testing of Differences in the Coefficients of Proportionality in the Study and Control Groups
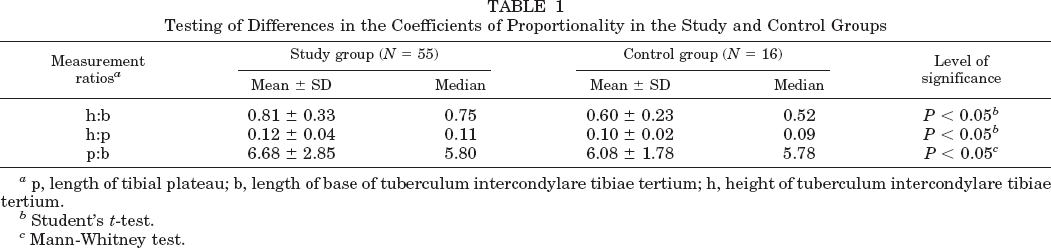
length of tibial plateau; b, length of base of tuberculum intercondylare tibiae tertium; h, height of tuberculum intercondylare tibiae tertium.
Student's t-test.
Mann-Whitney test.
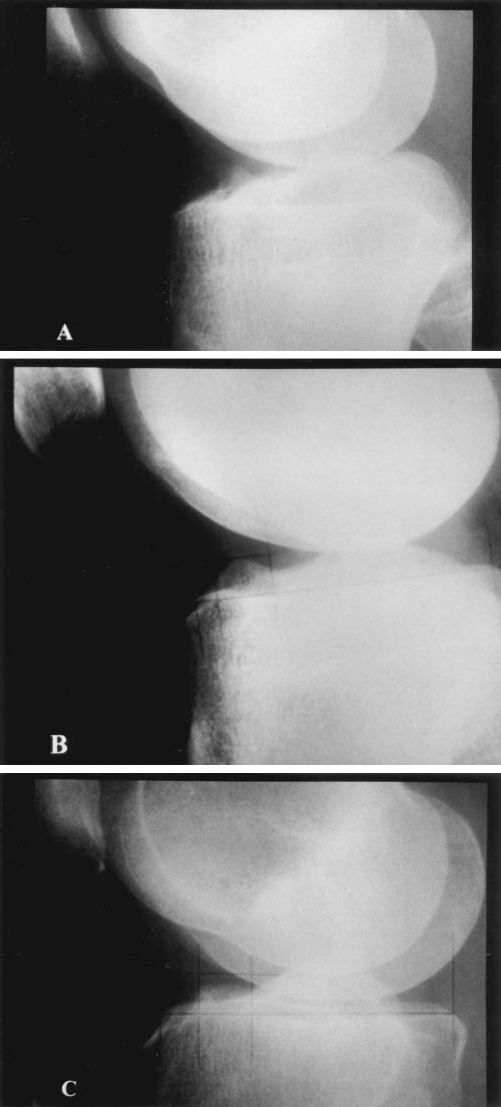
Tuberculum intercondylare tibiae tertium was classified into three main types: A, cone-shaped; B, dome-shaped; and C, plateau-shaped
Discussion
A survey of the available literature revealed no similar studies performed with a large sample size of either anatomic preparations or radiographs of the knee. The 13.3% prevalence of tuberculum intercondylare tibiae tertium recorded in our control group is consistent with the 11% and 10% reported by Jacobsen 3 and Berg, 1 respectively. This agreement additionally points to the importance of our finding that tuberculum intercondylare tibiae tertium was present in 32.2% of patients with ACL injury.
Although tuberculum intercondylare tibiae tertium has been observed by anatomists, radiologists, and clinicians, to the best of our knowledge it has not yet been related to the diagnosis of ACL lesions. Berg 1 underlined the clinical relevance of tuberculum intercondylare tibiae tertium as a point of orientation in ACL reconstructive operations. Liljedahl et al. 4 and Stallenberg et al. 8 did not include tuberculum intercondylare tibiae tertium in the extended group of radiologic signs relevant for the diagnosis of ACL lesion. We have demonstrated a statistically significantly higher prevalence of positive tuberculum intercondylare tibiae tertium findings in subjects with previous ACL injury. Thus, it appears that tuberculum intercondylare tibiae tertium is not only more common but also more pronounced, especially in height, in patients with ACL lesions than in the general population.
On the basis of our study we suggest that a positive finding of tuberculum intercondylare tibiae tertium ought to be included in the group of radiologic signs relevant for the diagnosis of ACL lesion. We also believe that further studies will support the fact that the finding of tuberculum intercondylare tibiae tertium on lateral radiographs of the knee points to a higher risk of ACL injury, whereas in cases of a previous knee lesion it raises the suspicion of a possible ACL rupture.