
Abstract
Athletes at risk for valgus extension overload are also at risk for tears of the anterior bundle of the ulnar collateral ligament. Some athletes develop ligament tears after procedures for valgus extension overload such as posteromedial olecranon osteotomy. The amount of posteromedial olecranon that can be resected before ulnar collateral ligament strain, and risk of injury, increases is unknown. We dissected and mounted five fresh-frozen human cadaveric elbows to allow strain gauge monitoring of the ulnar collateral ligament with varying valgus stress, elbow flexion angle, and medial osteotomy. The average strain to failure was 11.96% ± 6.51%, corresponding to a load of 347.71 ± 46.42 N. The maximum tensile force recorded at failure was 416.24 N. Three-way repeated-measures analysis of variance revealed no significant change in strain with change in the amount of osteotomy for a given applied load and angle of flexion. On the basis of these data, we conclude that the effect of medial olecranon osteotomy on ulnar collateral ligament strain may be small. Small sample size, elderly specimens, and the variables inherent in the experimental setup and mathematical modeling make it difficult to extrapolate these results to in vivo behavior of the anterior ulnar collateral ligament. Further work is needed before definitive guidelines for olecranon osteotomy can be formulated.
Valgus extension overload is a well-described entity in high-level throwing athletes.2,3,13,16 In cases where nonoperative management has failed, surgical treatment has been recommended, either arthroscopically or open in conjunction with other procedures around the elbow.2,13,16 Posteromedial decompression includes excision of osteophytes with or without resection of additional posteromedial bone from the proximal olecranon. Resection of varying amounts of the proximal olecranon has been shown to influence the stability of the elbow (at 0° and 90° of flexion) to valgus/varus loads, distraction/compression forces, and internal/external rotation. 1
The medial ulnar collateral ligament is a primary stabilizer to valgus stress between 20° and 120° of elbow flexion.4,14 The ulnar collateral ligament may account for up to 54% of the resistance to valgus loads at 90° of flexion. 11 Distraction is also largely (78%) resisted by the ulnar collateral ligament at 90° of flexion. 11 Distraction forces do occur at the elbow during the deceleration phase of overhand throwing, 7 but with the elbow extended these forces are largely (85%) resisted by the anterior capsule. 11 Internal rotation (pronation) torque about the elbow during throwing is thought to be fairly small. 6
The anterior oblique bundle of the ulnar collateral ligament is the most important contributor to valgus stability. Acute or attritional tears of the anterior oblique bundle have been documented to be severely debilitating for overhand throwing athletes.3,4,10 In a selective-cutting study, maximal valgus instability was present between 60° and 70° of flexion after transection of the anterior oblique bundle of the ulnar collateral ligament. 14 Cutting the capsule and posterior oblique bundle did not significantly destabilize the elbow to valgus stress from 0° to 140°. 14
The same group of athletes who are at risk for tears of the anterior ulnar collateral ligament are also at risk for valgus extension overload. It is not known whether the resection of posteromedial bone commonly performed for valgus extension overload puts these athletes at greater risk for rupture of their anterior ulnar collateral ligament. Theoretically, decreasing the secondary stabilizing action of the ulnohumeral articulation by resecting portions of the proximal medial olecranon should result in an even greater proportion of the applied valgus stress being absorbed by the anterior ulnar collateral ligament.
In this study, we investigated the effects of varying amounts of posteromedial olecranon osteotomy on ulnar collateral ligament stress in a cadaveric specimen. The hypothesis was that there would be an increase in anterior ulnar collateral ligament stress with increasing amounts of bone resection in olecranon osteotomy. The goal was to formulate recommendations for the maximum amount of bone resection in medial olecranon osteotomy for cases of valgus extension overload in throwing athletes.
Materials and Methods
Five fresh-frozen cadaveric elbow specimens (midhumerus through distal radius and ulna; all elderly specimens with estimated age of 60 years or older) were stripped of all soft tissue except for the following: anterior, posterior, and transverse ulnar collateral ligament bundles; anterior capsule; lateral ulnar collateral ligament; radial collateral ligament; annular ligament; and accessory collateral ligament. The triceps muscle insertion and posterior capsule were removed to allow access to the olecranon posteriorly. The forearms of the specimens were rigidly fixed in neutral pronation/supination by cross-pinning the distal radioulnar joint with Steinmann pins. This construct was then encased in methyl methacrylate cement. The cement encasement allowed for incorporation of an attachment point (wire loop) for the weights used to apply stress to the specimen.
The specimens were rigidly clamped with the epicondylar axis perpendicular to the horizontal plane, medial side up. A full flexion/extension arc was possible. A goniometer was used to directly determine the angle of flexion between the humerus and ulna. Measurements were made directly from the specimens, rather than from a radiograph, by a single observer (EJHH). The accuracy of angle measurement reflects the level of accuracy possible with a hand-held goniometer and was thought to be within the range of ±2°. Steinmann pins were drilled into the work surface below the specimen to act as guides to prevent changes in the selected angle of flexion during testing (Fig. 1). Care was taken to ensure that the guides were smooth and did not interfere with the deflection of the specimen. A differential variable reluctance transducer (DVRT, Microstrain, Inc., Burlington, Vermont) was inserted into the anterior portion of the anterior bundle of the ulnar collateral ligament of each specimen to allow direct monitoring of percent strain during testing.
The specimens were tested with valgus loads only. We used positions correlating to peak varus torques and falling within the typical total range of elbow flexion/extension during baseball pitching (18° ± 5° to 100° ± 13°). 8 Specifically, this included positions of elbow flexion around the position of maximum varus torque during pitching (95° ± 14°) 7 and the position of maximum valgus instability with an incompetent anterior bundle of the ulnar collateral ligament (70°) 14 noted by other investigators. Increments of 10° from 50° to 100° were used (six different positions in all).
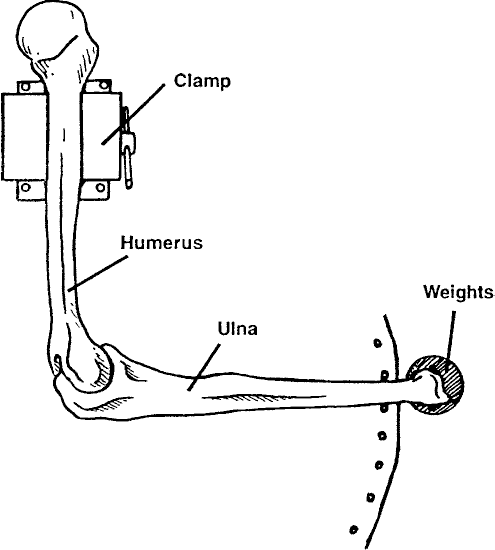
Overhead view of test setup. The proximal end of the humerus was clamped, while elbow flexion was constrained by a pair of Steinmann pins. (In the figure shown, the pins are constraining the elbow at 90° of flexion.)
The specimens were first tested in the intact state (no medial olecranon resection). Each position of flexion (50° to 100°) was tested. Sequential osteotomies were then done, extending from a point along the medial margin of the greater sigmoid notch corresponding to the junction between the middle and posterior thirds of the posterior oblique bundle of the ulnar collateral ligament (the probable furthest extent of arthroscopic visualization of this ligament bundle 15 ) proximally along a plane parallel to the sagittal plane of the olecranon. The insertion of the posterior ulnar collateral ligament was protected during the osteotomies, even though previous work has indicated that the posterior ulnar collateral ligament does not contribute significantly to valgus stability in the positions tested. 14 The osteotomy did not approach the insertion of the anterior bundle of the ulnar collateral ligament; thus, this structure was never jeopardized by the osteotomy. The osteotomy pattern was chosen to be measurable, reproducible, and to approximate the osteotomy that has been described for valgus extension overload 16 without extending anteriorly to what could be done through an arthroscope.
Testing was repeated after each incremental resection of the medial olecranon (2-mm increments), up to 8 mm of resection. A final osteotomy of 5 mm of the proximal olecranon tip was then performed and testing was completed (Fig. 2). This last osteotomy represented a worst-case scenario of bone resection. All specimens were then strained to failure at 90° of flexion after this biplanar osteotomy. The incremental osteotomies were created by measurement and resection of bone using an osteotome, under direct vision. The strain gauge was left in place while each new osteotomy was performed (gauge was repositioned before the first osteotomy on the first specimen only).
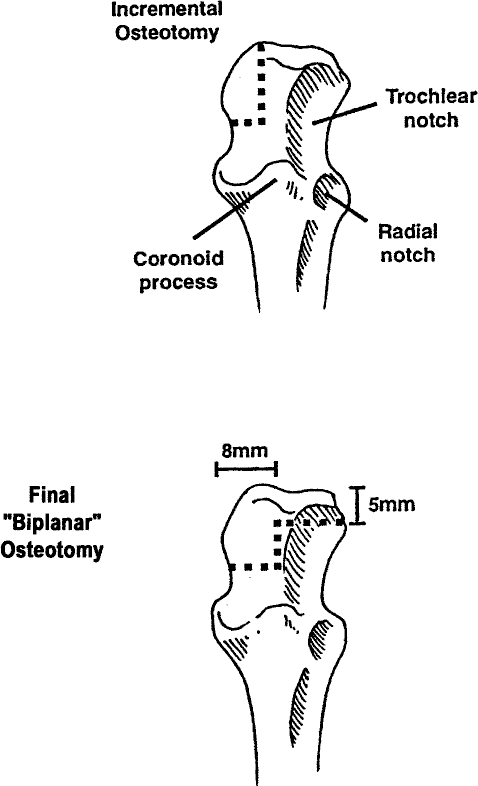
Lateral view of the distal end of a right ulna. Osteotomy was performed along the dotted line for the incremental osteotomies (top figure) and final “biplanar” osteotomy (bottom figure).
Because static strain behavior with change in load was to be studied, without constraint by any predetermined load amounts, a commonly available set of traction weights was used to apply convenient load increments. Weights of 0 N (no weight), 8.55 N, 17.45 N, and 26.35 N were applied to each specimen. These weights were suspended from a wire loop in the forearm located an average of 22.3 cm from the center of the radiocapitellar joint, which was in turn an average of 3.8 cm from the ulnar collateral ligament (Fig. 3). Corresponding average torques on the ulnar collateral ligament for the weights were 0.0 N·m, 1.90 N·m, 3.29 N·m, and 5.88 N·m, respectively (actual measurements for each specimen used in tabulating data). The loads chosen were selected to be safely below the maximum torque to failure previously computed in cadaveric elbows (32.1 ± 9.6 N·m). 5 Only static loads were used, because the addition of a fourth variable (load rate) to the existing three (flexion angle, load, and amount of osteotomy) might complicate the stability and relevance of data from this initial study. The amount of force applied distally to produce failure of the ulnar collateral ligament varied between specimens.
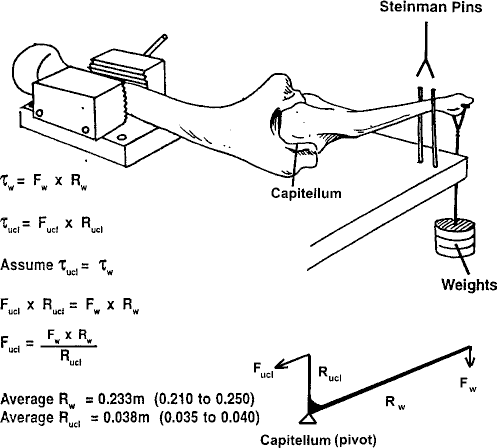
Side view of test setup. Elbow stability was maintained by equilibrium between valgus torque (τw) and varus torque (τucl). Fw, force exerted by the weight at attachment point to forearm; Rw, effective lever arm distance from the force applied to the forearm (Fw) to the fulcrum (radiocapitaller joint); Fucl, force exerted on the ulnar collateral ligament; Rucl, effective lever arm from the ulnar collateral ligament to the fulcrum (radiocapitellar joint).
Percent strain for each osteotomy was determined at each angle and at each applied force. Voltages read from the strain gauge were used in a formula derived from a calibration curve, [(volts – 0.0027)/1.588] + 9.2, to arrive at millimeters of displacement. Displacement values were then used to calculate the percent strain relative to the resting position at 50° of flexion with no osteotomy and no added force. A three-way repeated-measures analysis of variance was used to identify significant differences (P < 0.05) in ulnar collateral ligament strain for various levels of osteotomy, various valgus loads, and various elbow flexion angles. When significant differences were found with a three-way analysis of variance, a Student-Newman-Keuls test was used to isolate the specific significant differences.
Finally, strain to failure at 90° was observed for each specimen by increasing the applied force in multiples of 1 pound (4.44 N) until the anterior bundle failed. The 90° position was chosen because it is closest to the position of peak valgus stress during overhand throwing and also was noted to demonstrate high strains during this current study.
Results
After tabulating the data for each of the specimens, we calculated the mean values for percent strain versus osteotomy level at each applied force level for each angle of flexion (Table 1). For the different levels of osteotomy, no statistically significant changes in strain were found (Table 1). The greatest differences in ulnar collateral ligament strain were seen when the elbow was flexed 50°.
Percent Strain a Values (Mean ± SD) in the Ulnar Collateral Ligament at Increasing Levels of Osteotomy for Each Applied Force at Each Flexion Angle
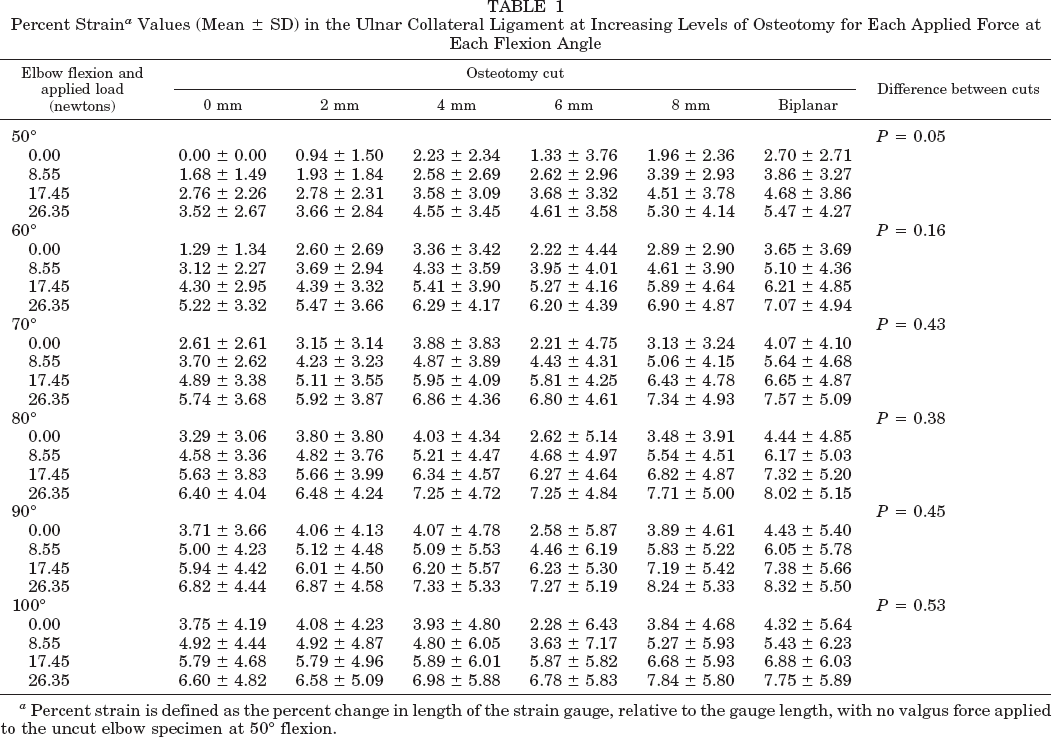
Percent strain is defined as the percent change in length of the strain gauge, relative to the gauge length, with no valgus force applied to the uncut elbow specimen at 50° flexion.
Ulnar collateral ligament strain did increase significantly with increased applied load, as expected. There were also statistically significant differences among levels of elbow flexion. In the intact state (no medial olecranon resection) significant differences were found between 50° and each of the other positions. At 2 mm of resection, the 50° position was once again significantly different from each of the other positions. At 4 mm, strain at 50° was significantly different from strain at 80° and at 90° of flexion. At 8 mm of resection, the only significant difference was between 50° and 90°. No significant differences in strain between angles were found at 6 mm of resection or at biplanar osteotomy.
Percent strain to failure and load to failure for each specimen are shown in Table 2. Load to failure is expressed as both the valgus torque applied to the elbow and the corresponding tensile force on the ulnar collateral ligament. To calculate the ulnar collateral ligament tensile force, the moment arm distance between the ulnar collateral ligament and the center of the radiocapitellar joint of the elbow was measured directly and used.
Ulnar Collateral Ligament Percent Strain a and Load to Failure
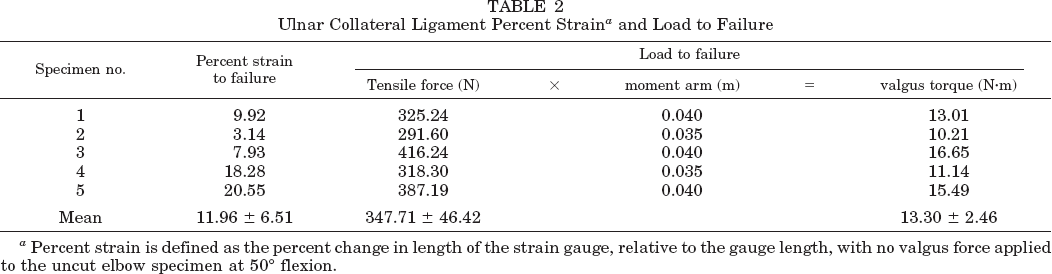
Percent strain is defined as the percent change in length of the strain gauge, relative to the gauge length, with no valgus force applied to the uncut elbow specimen at 50° flexion.
Discussion
Previous investigators have examined the biomechanics of the ulnar collateral ligament in vivo by indirectly determining the forces produced across the medial side of the elbow during throwing.6–9 Others have examined stress-strain relationships in cadaveric specimens, with experiments including loading intact elbows or isolated ligament specimens to failure.1,11,12,14 An et al. 1 examined the effect of removing portions of the proximal olecranon on the stability of the elbow to various loads, including a valgus stress at 0° and 90°. They employed a mathematical stiffness method to determine the effect of sequential resection of quarters of the olecranon with regard to deflection of their specimen at 0° and 90°. Their study did not specifically address what strain was produced in the anterior bundle of the ulnar collateral ligament, nor did it simulate the osteotomy that might be performed for valgus extension overload and posteromedial osteophytes. Additional work by the same authors did determine stress-strain behavior of the anterior bundle of the ulnar collateral ligament as an isolated specimen. 12 Of note, they observed a strain to failure of close to 30%, which is considerably higher than that noted in this study. We are not aware of any other studies that have addressed the strain to failure of the anterior bundle of the ulnar collateral ligament as an isolated entity.
In this study we sought to determine by direct measurement (strain gauge) the behavior of the anterior bundle of the ulnar collateral ligament in various positions of flexion, with various loads, after medial olecranon osteotomy simulating that which might be done for valgus extension overload. 16 We also then went beyond the osteotomy amount that would normally be done clinically to simulate a worst-case scenario. At the levels of valgus load applied in this study, there were no statistically significant increases in strain with increasing osteotomy, up to 8 mm, at any given degree of flexion selected. Although the mean values for some load/angle/osteotomy combinations may appear to differ noticeably, the relatively high standard deviations excluded the possibility of achieving significance. A larger sample size might help clarify some of the observed data trends.
Interestingly, a decrease in mean strain was seen between 4 and 6 mm of osteotomy for most applied loads and angles (Table 1). This paradoxical decrease in mean strain may be due to the large negative strains recorded for two of our specimens. These negative strains are potentially related to the position sensitivity of the data derived from a strain gauge in the ulnar collateral ligament. The anterior third of the anterior bundle of the ulnar collateral ligament was uniformly chosen for the placement of the strain gauge. This location can exhibit some relaxation with flexion, especially when not under load. 12 It is also possible for some of the data to be operator-dependent, since a reasonable amount of relaxation time must be allowed before recording the voltage across the strain gauge. However, although different assistants helped with various specimens, one of the principal investigators (EJHH) was always present. Another possibility is that the geometry of the ulnohumeral articulation was altered in such a way by the osteotomy that other structures were absorbing the load in cases in which negative strains occurred. It is also possible that the strain gauge pin separation distance changed slightly during some of the osteotomies.
It is difficult to extrapolate the results of this study to the baseball pitcher in vivo. Further work should be done before definitive recommendations regarding medial olecranon osteotomy can be made. Careful control of strain gauge placement and adequate relaxation time are probably important for the experimental design used in our study. If possible, higher and more dynamic loads (closer to those relevant to pitching) should be used. More rapid application of load and recording of strain at the instant of peak stress might also give data more directly applicable to the in vivo behavior of the ulnar collateral ligament. It should be pointed out that the maximum stress at the anterior ulnar collateral ligament calculated for this study was 416.24 N (16.65 N·m), which was significantly lower than the stress seen at failure by Dillman et al. 5 and also significantly lower than the 64 N·m varus torque that occurs during baseball pitching. 7 In our model, all dynamic or static restraints other than the deep ligament complexes were absent. We also eliminated motion in pronation and supination.
Three of the five elbows used in this study appeared to be from elderly female donors, and the other two appeared to be from older male donors. These factors may also decrease the relevance of the strain to failure seen in this study when compared with a young, athletic population. A larger sample size with younger specimens might be helpful in determining the clinical relevance of this type of study. There did appear to be a progression of increased strain with increasing load and increasing levels of osteotomy; however, it was not completely linear. On the basis of our results in this study, it appears that resecting a portion of the medial olecranon and the olecranon tip probably does not put the anterior bundle of the ulnar collateral ligament in jeopardy at moderate levels of quasistatic valgus stress.
This study cannot be considered to provide a definitive answer to the question, “Does medial olecranon osteotomy/debridement for valgus extension overload put the anterior bundle of the ulnar collateral ligament at risk in a throwing athlete?” However, it also does not give any indications for abandoning a procedure that has an established track record in treating athletes with valgus extension overload.