
Abstract
The objective of this prospective study was to determine the prevalence of popliteal cysts and the associated intraarticular lesions in a group of 100 patients scheduled for arthroscopic surgery of the knee and to evaluate the results of arthroscopic treatment for these intraarticular lesions without removal of the cyst. One hundred patients without any knee complaints served as a control group. The diagnosis of a popliteal cyst was made on the basis of ultrasonography. The prevalence of popliteal cysts was 20% in the study group and 0% in the control group. Patients with a popliteal cyst had a significantly higher prevalence of medial meniscal tears (70% versus 19%) and of chondral lesions (85% versus 28%). Tears of the lateral meniscus, however, were more evenly distributed (20% versus 36%). Sixteen of 20 patients with a popliteal cyst were available for a follow-up examination 1 to 3 years after the arthroscopic procedure. Eleven popliteal cysts had persisted. Chondral lesions were the most relevant prognostic factor; all patients with persisting cysts had grade III or grade IV lesions. We conclude that the popliteal cyst is a secondary phenomenon and that treatment should address the underlying intraarticular lesions. In cases of osteoarthritis it may be impossible to treat the chondral lesion successfully in terms of eliminating the effusion.
In 1877, Baker 1 described the association of popliteal cysts with intraarticular lesions. Several authors have reported that 41% to 83% of joint disorders have associated popliteal cysts.2,6,17 A high recurrence rate has been observed after surgical removal of the cyst. 13 This has led to the concept that the underlying intraarticular lesions should be treated, with the expectation that surgical correction of the intraarticular disorder would abolish the cyst.
The objective of this prospective study was to determine the prevalence of popliteal cysts and underlying intraarticular lesions in a group of 100 patients and to evaluate the results of arthroscopic treatment for these intraarticular lesions without removal of the cyst.
Materials and Methods
Subjects
One hundred patients (35 women and 65 men) who were scheduled for consecutive arthroscopic knee surgery were participants in this prospective study. Their average age was 41 years (range, 20 to 76). All patients had knee pain and none had any history of trauma. There were no cases of rheumatoid arthritis in this series. One hundred patients (45 women and 55 men) who did not have any knee problems served as the control group. Their average age was 50 years (range, 18 to 78). These patients were hospitalized for surgery of the spine, shoulder, hip joint, or foot.
Ultrasonographic Examination
All patients in the study and control groups underwent ultrasonographic examination of the knee. The ultrasonography was performed by an experienced examiner with a 7.5-MHz linear scanner (Sono Diagnost 360; Philips GmbH, Hamburg, Germany). The popliteal cyst was represented by an anechoic structure on the dorsal aspect of the knee joint (Fig. 1). In most cases the connection between the cyst and posterior joint capsule could be visualized. The prevalence and dimension of any popliteal cysts were determined. Cysts were classified as small (less than 3 cm), medium (3 to 5 cm), or large (more than 5 cm).
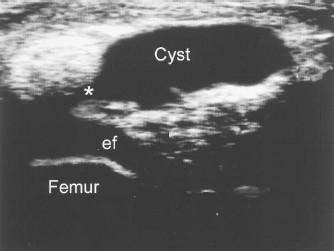
Ultrasonogram of a popliteal cyst. In this longitudinal section in the sagittal plane the cyst appears as an anechoic structure with enhancement of echogenicity behind the cyst. In most cases the connection between the cyst and the joint cavity can be visualized (asterisk). Effusion (ef) is visible as an anechoic band behind the femur.
Arthroscopy
All patients in the study underwent diagnostic arthroscopy the day after ultrasonography. The various pathologic conditions were documented. Meniscal lesions were treated by partial meniscectomy, and loose bodies were removed. Chondral lesions were classified according to Outerbridge 11 and were treated depending on the stage of the lesion. Patients with grade I lesions received no surgical treatment, patients with grade II and grade III lesions were treated with debridement, and patients with grade IV lesions were treated with the microfracturing technique. This technique, which enhances chondral resurfacing, involves the use of specially designed awls for creating multiple perforations or “microfractures” into the subchondral bone plate. In cases of pronounced localized synovitis a partial synovectomy was performed.
Follow-up
Subjective outcome was measured by using a visual analog scale that was scaled from 1 (excellent) to 10 (not satisfied). The rating was done before ultrasonography was performed so that the patients would not know whether the cyst had disappeared or persisted. All patients underwent ultrasonographic examination at follow-up at least 1 year after the operation. The prevalence and dimension of popliteal cysts were again determined.
Statistical Analysis
Statistical analysis was done using the Maentel-Haenszel test. The level of significance was set at P < 0.05.
Results
Prevalence
In the study group of 100 patients, 20 patients were found to have popliteal cysts (20%) visible on ultrasonographic examination. One cyst was graded as small, 10 cysts were graded as medium, and 9 cysts were graded as large. In the control group no popliteal cysts were detected by ultrasonography.
Intraarticular Lesions
Among the 20 patients with popliteal cysts 17 (85%) had chondral lesions and 14 (70%) had medial meniscal tears. This was significantly higher than the prevalence in patients without a popliteal cyst (22 of 80 [28%] for chondral lesions and 15 of 80 [19%] for meniscal tears; P < 0.001). In patients with popliteal cysts, grade III and grade IV lesions of the cartilage were predominant (70%, 14 of 20), whereas in patients without a popliteal cyst, only 6% (5 of 80) had grade III or grade IV lesions of the cartilage (Fig. 2). There was no significant difference between patients with popliteal cysts and those without with respect to lateral meniscal tears (20% versus 36%) and loose bodies (25% versus 11%).
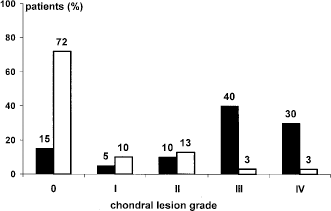
Distribution of chondral lesions. Results are given as percentages of the involved knees of each subgroup: patients with a popliteal cyst (black columns); patients without a popliteal cyst (white columns).
Follow-up
Of the 20 patients with popliteal cysts, 4 were lost to follow-up. Two of the four patients had died, and two declined to participate in follow-up because of time constraints. Thus, 16 patients were left for follow-up examination 1 to 3 years (mean, 2.1) after the procedure. In 5 of the 16 patients, the popliteal cysts had disappeared. Eleven cysts had persisted. In nine cysts the cyst length remained unchanged, whereas in two cysts the length had increased, resulting in an upgrade from medium size to large size. A decrease in length was not found.
The 11 patients with residual cysts were dissatisfied with the outcome of the arthroscopic procedure, rating their knee on the visual analog scale as 9 (2 patients) or 10 (9 patients) (mean score, 9.8), whereas patients whose cysts had disappeared rated their results as good (mean score, 2.0; visual analog scale ratings of 1 [2 patients], 2 [2 patients], and 4 [1 patient]). This difference was significant (P < 0.001). Ten of the 11 patients with persisting cysts had grade III or grade IV chondral lesions (Fig. 3). In contrast, none of the five patients whose cysts had disappeared after arthroscopic treatment had grade III or grade IV chondral lesions.
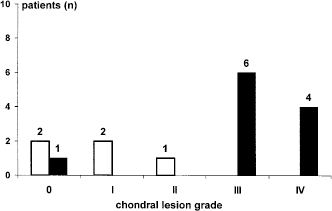
Distribution and grading of chondral lesions with respect to the evolution of the cysts after arthroscopy (white columns, cyst has disappeared; black columns, cyst has persisted). The numbers on the columns represent the number of patients.
Discussion
Rauschning and Lindgren9,14 distinguished between two types of cysts based on completely disparate etiopathologic backgrounds. The primary or idiopathic cyst has a valvular connection with the joint cavity, impeding fluid reflux from the cyst into the joint. This type seems to occur in children or young adults without causing any joint symptoms. The secondary or symptomatic cyst communicates freely with the joint cavity. In the majority of these cases, patients have articular symptoms.
Childress 3 identified medial meniscal tears, which occur predominantly in the posterior horn, as underlying pathologic lesions. In an MRI-based study, Miller et al. 10 analyzed 77 popliteal cysts with respect to associated joint abnormalities such as joint effusion, meniscal tears, and degenerative joint disease. There was only one instance of a popliteal cyst that occurred in the complete absence of any abnormality, and there were seven cases in which a popliteal cyst was associated with only one of these conditions.
Stone et al. 16 noted 238 popliteal cysts on 1760 MRI knee scans. One hundred eleven complete meniscal tears and 88 degenerative tears were also found in association with the cysts. Thus, meniscal tears were seen in 84% of knees with a finding of a popliteal cyst. The authors concluded that a tear of the posterior horn of the medial meniscus is the pathologic change most often associated with a popliteal cyst. They did not give any data concerning effusion or chondral lesions. Using arthroscopy, Sansone and De Ponti 15 noted 27 medial meniscal tears in 30 patients with popliteal cysts (90%). They performed a selective meniscectomy of the medial meniscus, and at the end of the procedure, in 27 of 30 cases, there appeared an oval opening located between the meniscal body and the posterior horn that extended to the articular capsule. Johnson et al. 8 described the entry in the cyst behind a capsular fold of the posterior wall of the medial compartment.
In our study we used ultrasonography to evaluate the prevalence of popliteal cysts. The accuracy of this method in the diagnosis of popliteal cysts has been established by a number of studies.4,5,7,12 Our data confirm the observation that in adults popliteal cysts are secondary cysts associated with an intraarticular lesion of the knee. As in previous studies, we saw a high prevalence of tears of the medial meniscus, although the number was below that reported by Stone et al. 16 and by Sansone and De Ponti. 15 Unlike those authors, we found that articular cartilage lesions were the intraarticular lesion most often associated with a popliteal cyst. We suggest that lesions of the articular cartilage have an important role in the pathogenesis of secondary popliteal cysts. In those cases without articular cartilage lesions or in which there were only low-grade lesions, the cysts disappeared after arthroscopy. In those cases with high-grade chondral lesions the cysts persisted. This fact can be explained by the hypothesis that the popliteal cyst arises from fluid distension of a communicating gastrocnemio-semimembranous bursa and that in adult patients the secondary popliteal cyst communicates freely with the joint cavity, allowing ready fluid exchange between the two cavities.
Low-grade chondral lesions and meniscal tears can be treated successfully by arthroscopic means, whereas arthroscopic surgery for high-grade chondral lesions may fail to eliminate effusion. Consequently, the cyst remains filled with effusion and cannot collapse and disappear. This hypothesis is supported by the fact that no cyst was detected in the control group and by the fact that patients with persisting cysts had a bad clinical result. The dissatisfying clinical results suggest that in these cases the arthroscopic treatment for intraarticular lesions was not successful.
Conclusions
In adults with knee symptoms the popliteal cyst itself should not be the primary target of surgical treatment. The primary focus of the arthroscopic procedure should be to correct the underlying intraarticular abnormalities, with the goal of resolving effusion. It seems that effusion has a key role in the pathogenesis of the cyst. The grade of chondral lesions has a more important effect on outcome than the presence of meniscal lesions. In cases of degenerative osteoarthritis with grade III or grade IV lesions of the articular cartilage, addressing the intraarticular lesions with arthroscopic surgery to treat the popliteal cyst may be an unrealistic goal.