
Abstract
The throwing shoulder in pitchers frequently exhibits a paradox of glenohumeral joint motion, in which excessive external rotation is present at the expense of decreased internal rotation. The object of this study was to determine the role of humeral head retroversion in relation to increased glenohumeral external rotation. Glenohumeral joint range of motion and laxity along with humeral head and glenoid version of the dominant versus nondominant shoulders were studied in 25 professional pitchers and 25 nonthrowing subjects. Each subject underwent a computed tomography scan to determine bilateral humeral head and glenoid version. The throwing group demonstrated a significant increase in the dominant shoulder versus the nondominant shoulder in humeral head retroversion, glenoid retroversion, external rotation at 90°, and external rotation in the scapular plane. Internal rotation was decreased in the dominant shoulder. Total range of motion, anterior glenohumeral laxity, and posterior glenohumeral laxity were found to be equal bilaterally. The nonthrowing group demonstrated no significant difference in humeral head retroversion, glenoid retroversion, external rotation at 90° or external rotation in the scapular plane between shoulders, and no difference in internal rotation at 90°, total motion, or laxity. A comparison of the dominant shoulders of the two groups indicated that both external rotation at 90° and humeral head retroversion were significantly greater in the throwing group.
In the throwing athlete, a delicate balance of mobility and dynamic stability is required for the shoulder. Dynamic stabilization of the glenohumeral joint is accomplished through coordinated muscular activities coupled with ligament and capsular restraints. Competitive overhead throwing athletes perform at the extremes of glenohumeral motion and place tremendous repetitive stresses on their shoulders. These stresses generate humeral angular velocities of up to 7550 deg/sec and rotational torques of up to 67 N·m. 11 The importance of this delicate balance is apparent when considering that the shoulder joint must withstand these forces over the course of a season or a career. When this balance is disrupted, shoulder instability and secondary impingement may result.
Most of the interest in shoulder instability and secondary impingement has focused on the static stabilizers of the shoulder, specifically the soft tissues. Many researchers have investigated the role of excessive motion, capsular laxity, and limited shoulder flexibility as possible etiologic factors in instability and impingement.1,3,6,14,15,22,23,30 Evidence exists that the dominant shoulder in throwing athletes exhibits a unique and paradoxical glenohumeral range of motion. Specifically, there is greater external rotation and a loss of internal rotation when the dominant shoulder is compared with the nondominant shoulder.3,14,15,22,28 The implication of this altered arc of motion is that a physiologic adaptation of the dominant shoulder through repetitive microtrauma leads to selective stretching of the anterior capsule and tightening of the posterior capsule, creating a propensity for instability and secondary impingement.3,14,15,22,28
It is well known that stress reaction and adaptational processes can be found not only in soft tissues but also in osseous structures. Previous studies have revealed that adaptive changes in the osseous anatomy of the humerus occur in throwing athletes. 25 In addition, many studies have documented the importance of the skeletal anatomy of the glenohumeral joint to shoulder stability.4,13 At this time, controversy exists as to the contribution of soft tissue and osseous anatomy in the development of shoulder instability and secondary impingement.
The purpose of this study was to determine the stability, range of motion, and the version of the glenohumeral joint in a population of asymptomatic elite throwing athletes versus a nonthrowing control-matched population. Additionally, we compared the dominant with the nondominant shoulder in each subject. Our goal was to determine whether a significant osseous difference existed between groups and between bilateral shoulders and whether this difference might be a factor contributing to the motion paradox seen in elite throwing athletes.
Materials and Methods
The subject groups in this study consisted of 25 male professional baseball pitchers, all of whom started pitching before the age of 10 years, and 25 male control-matched subjects, none of whom were involved in any overhead throwing sports. All subjects in both groups were between the ages of 18 and 35 years and were seen at a professional baseball spring training camp and at the Alabama Sports Medicine and Orthopaedic Clinic, respectively. Exclusion criteria for the throwing group included a history of shoulder surgery, humeral fracture, shoulder tumor, or pitching-related shoulder pain that had required medical attention. Exclusion criteria for the control group included a history of shoulder surgery, humeral fracture, shoulder tumor, or any participation in an organized sport involving overhead shoulder motion. These sports included but were not limited to baseball, tennis, volleyball, swimming, javelin, European handball, or participation in the “throwing position” of other sports (for example, quarterback in football).
All subjects were required to provide informed consent before participation, in accordance with the policy of HealthSouth Medical Center's Institutional Review Board, which reviewed and approved this study before it began. The risk of participation in the study was explained to each subject before he signed the consent form. This study was designed in compliance with the ethical guidelines outlined by the Declaration of Helsinki.
All subjects underwent a physical examination and had their history taken by the orthopaedic staff. Glenohumeral range of motion, laxity, and humeral head and glenoid retroversion of the dominant versus nondominant shoulders were assessed in both the throwing and nonthrowing groups. One examiner assessed and documented glenohumeral range of motion using standard goniometric techniques. 2 Specific variables tested included 1) external rotation at 90° of thoracohumeral abduction and in the plane of the scapula at 45° of thoracohumeral abduction, 2) internal rotation at 90° of thoracohumeral abduction, and 3) total motion arc at 90° of thoracohumeral abduction (Fig. 1). Total motion arc was defined as external rotation minus internal rotation at 90° of thoracohumeral abduction. The starting point for the measurements of both external and internal rotation was with the subject supine, arm abducted to 90°, elbow flexed to 90°, and the arm and hand pointed vertically toward the front of the body (the ceiling in this case).
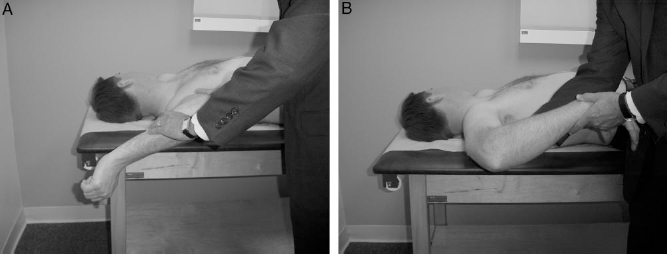
The method for measuring internal (A) and external (B) rotation.
Two experienced examiners assessed anterior and posterior laxity (Fig. 2) and checked for a sulcus sign. Anterior and posterior glenohumeral laxity was assessed according to the system proposed by Hawkins and Bokor 12 : grade I, translation of the humeral head contained within the glenoid; grade II, translation of the humeral head onto the glenoid rim with immediate relocation on removal of the anterior or posterior stress; and grade III, translation of the humeral head over the glenoid rim without relocation with removal of stress. The sulcus sign was graded from 0 to 2; with 0 equaling no sulcus sign, 1 equaling less than 5 mm of inferior translation, and 2 equaling 5 mm or more of inferior translation.

The method for measuring anterior and posterior laxity.
After giving informed consent, each subject underwent a CT scan (GE Hilite Advantage, G. E. Medical Systems, Milwaukee, Wisconsin). Computed tomographic testing was performed at St. Anthony Hospital in St. Petersburg, Florida, for the professional pitchers and at HealthSouth Medical Center in Birmingham, Alabama, for the control population under the direction of a board-certified radiologist. Computed tomographic testing was performed according to the protocol described by Hill et al. 13 During CT testing, subjects were placed in a supine position with their arms locked at the sides to prevent any rotation of the humerus during the procedure. Some patients had shoulders too broad to allow for scanning both shoulders simultaneously and, therefore, scans in these patients were performed one shoulder at a time, with the contralateral shoulder being held in an abducted position over the head.
Three to six axial cuts were imaged through the humeral head and approximately three axial cuts were imaged through the capitellum and trochlea to obtain our measurement axis. Humeral torsion was measured by noting the difference between a line parallel to the distal articular surface and a line bisecting a spherical section of the head. The measurement of the humeral head bisector was determined according to the protocol described by Hill et al. 13 Using the smallest concentric circle that conformed to the humeral head radius, we marked two points at 90° to the anterior articular margin point on the film. The line between these points served as our humeral head axis (Fig. 3).
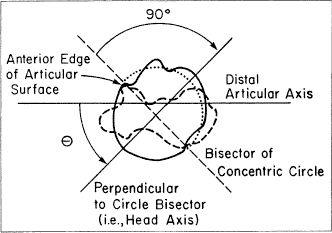
Diagram demonstrating measurement of humeral head retroversion. (Reprinted with permission from Hill JA, Tkach L, Hendrix RW: A study of glenohumeral orientation in patients with anterior recurrent shoulder dislocations using computerized axial tomography.
Glenoid version was determined as described by Hill et al. 13 As they describe it, the subspinous medial border of the scapula, extending from the intersection of the spine with the body to well distal of the glenoid, is consistently linear. In cross section, the line formed by this point and the midpoint of the transverse glenoid diameter at the level of the articular surface defines the axis of the scapula. Glenoid tilt is the angle formed by the intersection of this line and a line parallel to the glenoid articular surface. It is measured as the angular difference between the perpendicular-to-the-scapula axis and the line parallel to the glenoid articular surface (Fig. 4).

Diagram demonstrating measurement of glenoid tilt. (Reprinted with permission from Hill JA, Tkach L, Hendrix RW: A study of glenohumeral orientation in patients with anterior recurrent shoulder dislocations using computerized axial tomography.
A paired t-test was used to compare the differences in range of motion, stability, and humeral head and glenoid retroversion for the dominant versus nondominant shoulders of each subject. An independent t-test was used to compare range of motion and retroversion for the control group versus the elite throwing group. The Fisher's exact test was used to compare discrete stability measures between dominant and nondominant shoulders and between the control and throwing groups. That level of statistical significance was set at P < 0.01. All analyses were conducted using SPSS 8.0 for Windows (SPSS, Inc., Chicago, Illinois).
Results
The results indicated the following for the throwing group (Table 1): 1) humeral head retroversion was significantly increased in the dominant shoulder compared with the nondominant shoulder, 2) glenoid retroversion was significantly increased in the dominant shoulder compared with the nondominant shoulder, 3) external rotation at 90° was significantly greater in the dominant shoulder compared with the nondominant shoulder, 4) external rotation in the scapular plane was significantly increased in the dominant shoulder compared with the nondominant shoulder, and 5) internal rotation was significantly greater in the nondominant shoulder compared with the dominant shoulder. However, total range of motion and glenohumeral laxity, including anterior laxity, posterior laxity, and the sulcus sign were not significantly different between shoulders.
Comparison of Dominant and Nondominant Shoulders in the Throwing Group
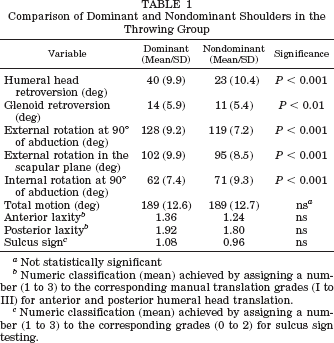
Not statistically significant
Numeric classification (mean) achieved by assigning a number (1 to 3) to the corresponding manual translation grades (I to III) for anterior and posterior humeral head translation.
Numeric classification (mean) achieved by assigning a number (1 to 3) to the corresponding grades (0 to 2) for sulcus sign testing.
Significant findings in the nonthrowing group were as follows (Table 2): 1) increased internal rotation at 90° for the nondominant shoulder compared with the dominant shoulder, and 2) increased external rotation in the scapular plane for the dominant shoulder compared with the nondominant shoulder. There were no significant differences in humeral head retroversion, glenoid retroversion, total motion, external rotation at 90° or in the scapular plane between shoulders, and internal rotation at 90°, anterior laxity, posterior laxity, or in the presence of a sulcus sign between the dominant and nondominant shoulders.
Comparison of Dominant and Nondominant Shoulders in the Nonthrowing Group
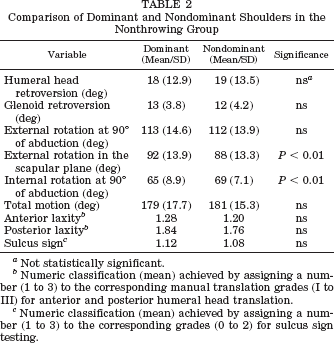
Not statistically significant.
Numeric classification (mean) achieved by assigning a number (1 to 3) to the corresponding manual translation grades (I to III) for anterior and posterior humeral head translation.
Numeric classification (mean) achieved by assigning a number (1 to 3) to the corresponding grades (0 to 2) for sulcus sign testing.
When the throwing and nonthrowing groups were compared the significant findings were as follows (Table 3): 1) humeral head retroversion in the dominant shoulder was significantly greater in the throwing group than in the nonthrowing group, 2) dominant shoulder external rotation at 90° was significantly greater in the throwing group than in the nonthrowing group, 3) nondominant shoulder external rotation at 90° was significantly greater in the throwing group than in the nonthrowing group, 4) dominant and nondominant shoulder external rotation in the scapular plane was significantly greater in the throwing group than in the nonthrowing group, and 5) total motion was greater in the dominant and nondominant shoulders for the throwing group than in the nonthrowing group.
Comparison of Shoulders between Throwing and Nonthrowing Groups
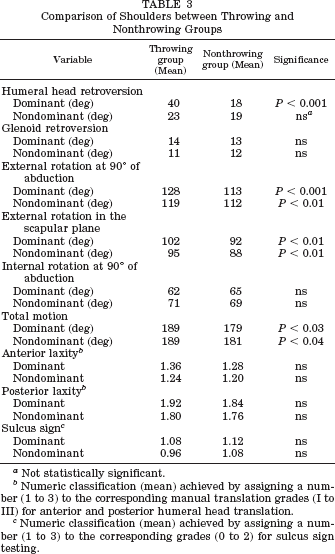
Not statistically significant.
Numeric classification (mean) achieved by assigning a number (1 to 3) to the corresponding manual translation grades (I to III) for anterior and posterior humeral head translation.
Numeric classification (mean) achieved by assigning a number (1 to 3) to the corresponding grades (0 to 2) for sulcus sign testing.
The important nonsignificant finding was that humeral head retroversion was not statistically significantly different between the nondominant shoulders of the throwing group and the nondominant shoulders of the nonthrowing group. Other nonsignificant findings included no difference between the dominant and nondominant shoulders in glenoid retroversion, anterior laxity, posterior laxity, sulcus sign, and internal rotation at 90°.
Discussion
The shoulder joint is a complex biomechanical unit with glenohumeral stability that is dependent on both soft tissue and osseous components. Numerous authors have studied the role of humeral head retroversion with respect to anterior dislocation and subluxation, posterior dislocation and subluxation, shoulder range of motion, osteoarthritis, replacement arthroplasty, and other pathologic conditions.7,19–21,24,27,29 In the throwing athlete, the shoulder performs at the extremes of glenohumeral motion. The goals of this study were to provide objective data for range of motion, laxity, and humeral head and glenoid retroversion between the dominant and nondominant shoulders of a population of elite throwing athletes and a control-matched athletic population not involved in overhead throwing sports. Our study differs from previous studies in which attempts were made to quantify humeral torsion, in that we used CT scans instead of roentgenograms.4,5,19,20,25,26 Methods of study in which roentgenograms are used introduce a small amount of error, which is difficult to quantify. 13 We believe that the use of CT scans produces a more reliable and accurate measurement of humeral head retroversion.
Our findings demonstrate that the increased external rotation and decreased internal rotation in the throwing shoulders of elite pitchers may not be primarily due to increased anterior capsular laxity and posterior capsular tightness, as has previously been postulated. 10 Instead, our data strongly suggest an important osseous contribution, specifically involving the humerus and glenoid.
Professional pitchers must be able to throw at tremendous velocities and avoid injury to remain effective. Our data show that in the throwing shoulder of pitchers there is an increase in humeral head retroversion that allows for greater external rotation and less internal rotation as compared with the nonthrowing shoulder. This anatomic finding has been described recently in the literature.5,25,32 The total motion was the same in both glenohumeral joints, which implies that the arc of motion, while the same value for each shoulder, was further externally rotated or “spun back” on the dominant side.
One of the authors (KEW) has termed this consistent range of motion between the shoulders of elite throwing athletes the “total motion concept.” 32 Namely, external rotation and internal rotation at 90° of abduction are added together to establish total motion. Clinically, we have seen the overwhelming majority of pitchers exhibit equal (within 5°) total motion when their shoulders are compared bilaterally.
Additionally, we found that glenohumeral laxity was not appreciably different side to side. This implies that the static capsular restraints of the dominant and nondominant shoulders are essentially equal. We recognize that although we found no gross difference in laxity, this does not necessarily mean that absolutely no difference exists. There was not enough statistical power in this study to address very small differences in side-to-side laxity. Additionally, one of the limitations of our study was the known interobserver and intraobserver variability with clinical examination grading in translation testing. However, our finding of equal laxity in both shoulders has also been demonstrated by Ellenbecker et al. 8 Furthermore, Bigliani et al. 3 reported that 61% of the professional pitchers in their study (44 of 72) exhibited a sulcus sign. Of those pitchers who exhibited a sulcus sign, 89% (39 of 44) had bilateral sulcus signs. These studies are in agreement with our findings that indicate laxity was equal bilaterally in most subjects.
Because there is no difference in humeral head retroversion in the nondominant shoulders of throwing and nonthrowing athletes, it is plausible that the increase in humeral head retroversion in the dominant shoulder is a developmental process. Humeral head retroversion has been shown to be subject to change during growth until maturity is reached. 18 Wolff 33 postulated that bone growth is wholly influenced by external stress. This type of unilateral growth and adaptation to external stress has been shown widely in the literature.16,17,26 Humeral torsion has also been shown to be affected by muscular forces alone.9,18 Kanematsu et al. (unpublished data, 1996) showed that muscle forces induced by excessive throwing at a young age are more powerful than previously appreciated. They reported displacements of the humeral epiphysis in Little League baseball pitchers that led to humeral neck deformity and longitudinal growth disturbance. They surmised that the bone formation was caused by repetitive mechanical stress to the proximal humeral epiphysis during growth.
In a recent study by Pieper, 25 a difference of 9.4° was observed in glenohumeral retroversion between the dominant and nondominant shoulders of 51 professional European handball players. Those players without chronic shoulder pain (N = 38) had a 14.4° difference in humeral retroversion. Those players with chronic arm pain (N = 14) had an average 5.4° decrease in humeral retroversion compared with that measured in the dominant shoulder of asymptomatic players. The author's conclusion was that those players who failed to “adapt” appropriately had a greater chance of chronic shoulder problems. Our study shows a 17.0° difference, on average, between the dominant and nondominant shoulders of asymptomatic elite pitchers. This would correspond to the 14.4° difference between the dominant and nondominant shoulders in asymptomatic European handball players previously described by Pieper.
We have postulated that baseball players, specifically pitchers, must adapt with an increase in humeral head retroversion in their dominant shoulder to reach an elite level and to have a decreased chance of injury. It is important to note that there may be a window of opportunity for this adaptation to occur before growth stops. Pitchers who are pitching before the end of skeletal growth and physeal closure may have the best chance to make this adaptation and continue on to become an elite baseball pitcher.
This developmental adaptation, humeral head retroversion, effectively “pre-positions” the dominant hand in a more externally rotated position than occurs in the contralateral, nondominant arm. Stated otherwise, the increase in glenohumeral retroversion allows for more external rotation before the shoulder is constrained by the anterior capsule and glenohumeral ligaments. 5 This may allow a competitive edge in pitching, because for the same amount of external rotation (which may relate positively to pitch velocity) the arm with more humeral head retroversion places less stress on the anterior capsulolabral structures. It may therefore be thought of as a protective adaptation that not only enhances performance but also decreases the chance of injury. A study specifically correlating humeral head retroversion to the incidence of injury and to pitch velocity is underway. This should give us more accurate information regarding the importance of pitching in the “window of adaptation.”
It is important to note that we are certainly not espousing unrestricted pitching at a young age. But we do advocate a well-monitored, age-appropriate pitching program. Our data imply that for the best chance of becoming an elite pitcher, a player might find it beneficial to pitch early in life and often, within the accepted parameters of safety. The concept of “saving my child's arm” during Little League with the intent to “pitch” the child when his arm becomes stronger, in high school or even later, may lead to unexpected results.
Another significant implication of this study involves the clinical relevance of stretching the posterior capsule to increase glenohumeral internal rotation. On the basis of this study, we believe that the loss of this internal rotation is due to an adaptive osseous change. Furthermore, stretching of the soft tissue is appropriate to maintain or increase internal rotation to help counter the tremendous eccentric forces generated during the deceleration and follow-through phases of throwing. 31 However, the clinician should approach joint mobilization techniques for the posterior capsule with caution. Our findings indicate that the posterior capsule in elite pitchers does not exhibit tightness; thus treatment techniques to increase flexibility of the posterior capsule may not be appropriate. However, stretches that target the posterior contractile tissue are appropriate and should be performed.31,32
We found an increase in humeral and glenoid retroversion in the dominant shoulders of throwing athletes compared with the nondominant shoulder, as well as an increase in external rotation at 90° and 45° of abduction and a decrease in internal rotation at 90°. Total motion and laxity were not significantly different from side to side. This study perhaps generates more questions than it answers about the complex biomechanical interplay involved in the elite throwing shoulder. Questions that remain include but are not limited to the following: 1) Does this increased external rotation provide a protective effect for the shoulder by allowing more external rotation with less stress on the anterior tissues at the glenohumeral joint, as implied in previous studies? 26 2) Does this increased external rotation have any relationship to increased pitch velocity and, if so, what is the effect? 3) Is this increased humeral head retroversion an adaptational or preexistent, inherent feature of the anatomy? 4) If this retroversion represents an adaptation to throwing at a young age, what influences affect this adaptation, and what is the time course over which this adaptation occurs? Current studies at the American Sports Medicine Institute, Birmingham, Alabama, are underway to address each of these questions with the hope that we will continue to expand our understanding of the throwing shoulder.