
Abstract
Seventy patients with patellar tendon or hamstring tendon autografts for single-incision anterior cruciate ligament reconstruction were evaluated at least 2 years after surgery. All reconstructions were performed by the same surgeon, and metal interference screws were used for fixation of all grafts. No significant differences were noted between groups for Lysholm score, reduction in activity, KT-1000 arthrometer findings, quadriceps muscle size, return to sports, or ability to jump and do hard cuts and pivots. Significantly more patients in the patellar tendon group had patellofemoral pain at 6 months after surgery than did the hamstring tendon patients (48% versus 20%), and at last follow-up the incidence of patellofemoral pain was 42% and 20%, respectively. Fourteen patients in the patellar tendon group and seven in the hamstring tendon group had loss of motion (approximately 5°). Four patients (two in each group) had treatment failures and their results were not included in the clinical examination data. At 2 years' follow-up, 97% of patients with patellar tendon grafts and 100% of patients with hamstring tendon grafts rated their results as good or excellent. We found that hamstring tendon grafts performed similarly to patellar tendon grafts, although fewer patients in the hamstring tendon group had patellofemoral pain and loss of motion.
The standard method for ACL reconstruction is bone-patellar tendon-bone autograft with interference screws. The most commonly used grafts for ACL reconstruction are patellar tendon and semitendinosus and gracilis (hamstring) tendon autografts or allografts. Disadvantages of patellar tendon autografts are risk of patellar fracture, potential increase in patellofemoral pain, and retained patellar tendon weakness or rupture.2,13 Disadvantages of hamstring tendon grafts include failure to achieve immediate fixation to bone. With the recent introduction of soft tissue interference screws, hamstring tendon grafts can be immediately fixed to bone with theoretically more stiffness and less tendon length between fixation points than when fixed with post, buttons, or staples.
Quadrupled hamstring tendon grafts have been shown to be stronger than patellar tendon grafts. In a recent study, Rowden et al. 21 examined the strength of the ACL before and after reconstruction with double-looped hamstring tendon and patellar tendon in young human cadaveric knees (average age, 42 years). The intact normal ACL had 2195 N of tensile strength when tested with the knee at 60° of flexion. After reconstruction with patellar tendon graft fixed with interference screws, the strength was 416 N, and after reconstruction with hamstring tendon graft fixed with posts and buttons, the strength was 612 N.
Patellar and hamstring tendon autografts have been compared both prospectively and retrospectively. The few randomized studies that have been done show essentially no significant difference in overall outcome.1,12,18 When evaluating these studies, it is important to note that the grafts that are being compared are fixed differently. Hamstring tendon grafts are fixed using posts or buttons and patellar tendon grafts are fixed with interference screws. In only one study have the two autografts been compared with only interference screws used for fixation, but that study was not randomized. 4 The present study is a prospectively randomized study designed to compare the outcome after single-incision ACL reconstruction with autogenous patellar tendon or hamstring tendon autografts, both fixed with interference screws by the same surgeon using the same surgical technique and aggressive postoperative rehabilitation.
Materials and Methods
From June 1994 to October 1996, 82 consecutive patients undergoing primary ACL reconstruction were randomized by birth date to ACL reconstructions using autogenous bone-patellar tendon-bone or hamstring tendon autografts. Patients were excluded if there were any other ligament tears in the same knee or if they were having revision ACL reconstruction. Patellar tendon grafts were used in patients with even-number birth dates and hamstring tendon grafts for those with odd-number birth dates. A single surgeon (DMK) performed or directly supervised all of the procedures, which included a single-incision technique with a notchplasty. Interference screws were used for fixation of all grafts in both the femoral and tibial tunnels. Independent evaluation was performed with a minimum follow-up of 24 months (average, 33; range, 24 to 45).
Subjects
Of the 82 patients entered in the study, 12 were lost to follow-up, leaving 70 patients (85%) (33 patellar tendon grafts, 37 hamstring tendon grafts). Of these 70 patients, 13 were unable to come in for clinical examination and only answered a questionnaire by mail. From these questionnaires, Lysholm scores, sports activity, patient overall rating of surgery, and patellar pain data were collected. In the patellar tendon group there were 26 male patients and 7 female patients; in the hamstring tendon group there were 21 male patients and 16 female patients. In the patellar tendon group, the mean age at surgery was 32 years (range, 14 to 48), mean weight was 78.9 kg, and mean height was 170.4 cm. In the hamstring tendon group, the mean age was 30 years (range, 14 to 53), mean weight was 72.5 kg, and mean height was 168.3 cm. There were no significant differences in any of these categories. Two patients in the patellar tendon group, one with early traumatic rupture and one with atraumatic graft failure, were not included in the 2-year follow-up tests, leaving 31 patients for final outcome data. In the hamstring tendon group, 2 patients had early traumatic rupture (both had a revision before the 1-year follow-up), leaving 35 patients with 2-year follow-up data.
The majority of injuries were noncontact-type injuries that occurred during basketball, skiing, or volleyball (Table 1). All patients had surgery more than 3 weeks after injury. There was no significant difference in average time from injury to surgery (19.5 weeks for the patellar tendon group and 18.9 weeks for the hamstring tendon group; P = 0.9). In the patellar tendon group, 17 patients had surgery 3 weeks to 3 months after injury, 5 patients had surgery at 3 to 6 months after injury, and 9 patients had surgery more than 6 months after surgery (including 3 patients who had surgery more than 2 years after injury). In the hamstring tendon group, 14 patients had surgery at 3 weeks to 3 months after injury, 5 patients had surgery 3 to 6 months after injury, and 16 patients had surgery more than 6 months after injury (including 6 patients who had surgery more than 2 years after injury). There were 7 competitive athletes in the patellar tendon group and 11 competitive athletes in the hamstring tendon group. The remaining patients were recreational athletes. All but two patients in each group played cutting sports before injury.
Activity at the Time of the ACL Tear
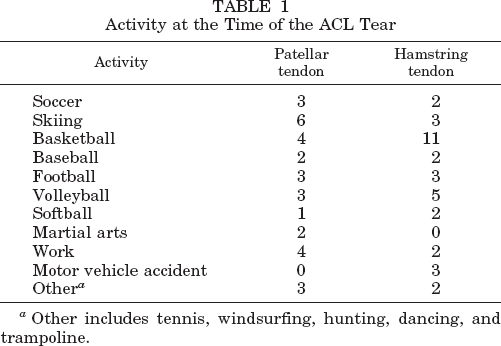
Other includes tennis, windsurfing, hunting, dancing, and trampoline.
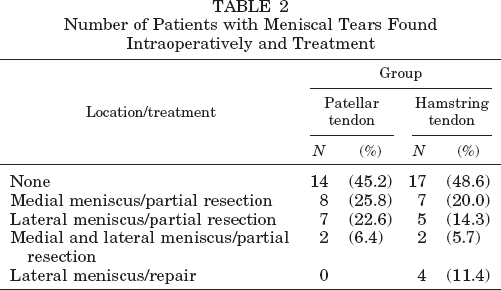
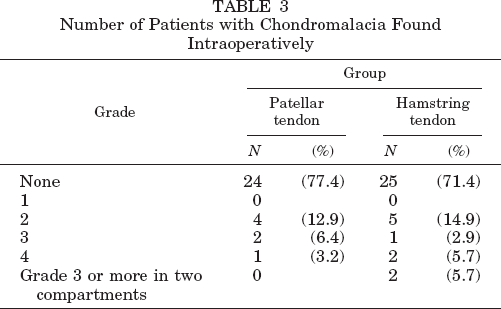
All patients reported experiencing giving way during sports before the operation. When they were examined under anesthesia, all patients had positive Lachman and pivot shift tests. In the patellar tendon group, 23 patients had a grade 2 Lachman test result and 8 patients had a grade 3 result. In the hamstring tendon group, 20 patients had a grade 2 result and 15 had a grade 3 result. Meniscal tear rates are shown in Table 2. The prevalence of chondromalacia is shown in Table 3.
Number of Patients with Meniscal Tears Found Intraoperatively and Treatment
Number of Patients with Chondromalacia Found Intraoperatively
Operative Procedure
Examination of the knee with the patient under anesthesia was followed by arthroscopic surgery through standard portals. Meniscal injuries were addressed with partial resection or repair by using an inside-out technique, and the meniscal repair sutures were tied after ACL reconstruction was complete. A tourniquet was used while the graft was obtained and during the reconstruction.
The patellar tendon autograft was harvested through a single midline incision. The middle third of the patellar tendon was dissected after the tendon width was measured. A 9-, 10-, or 11-mm central portion was removed, depending on the width of the original tendon. Bone plugs from the patella and the tibial tubercle were taken in line with the incised tendon by using a small saw. The bone plugs of the patellar tendon graft were approximately 10 mm (median, 9.8) by 25 mm.
When the hamstring tendons were used, an approximate 3-cm incision was made over the insertion of the pes anserinus at the anterior medial tibia. The hamstring tendons were harvested with a closed tendon stripper and prepared as a quadruple-strand graft.
The tibial and femoral bone tunnels were drilled to closely approximate the patellar or hamstring tendon graft, and the median value was 9.8 mm for the patellar tendon grafts and 7.84 mm for the hamstring tendon grafts. During modification and sizing of the ACL graft, a notchplasty was performed. The lateral femoral condyle and roof portion of the notch were enlarged so that the most posterior portion of the notch was easily viewed.
The tibial graft tunnel was drilled from the anteromedial tibia to the posterolateral footprint of the ACL. The guide pin entered the joint approximately 7 mm anterior to the PCL (at the level of the joint line). The femoral graft tunnel was drilled over a guide pin placed from the medial arthroscopic portal with the knee fully flexed. The graft was passed with sutures with a beath pin and pulled up into the 30-mm femoral tunnel. After the graft was in place, a round-head cannulated, noncutting, metal interference screw (DonJoy RCI, Smith & Nephew, Andover, Massachusetts) was placed from the anteromedial arthroscopic portal. The tibial interference screw was placed through the anteromedial cortex and the notch was checked for graft impingement. The grafts were not rotated. Routine closure was performed with closure of the patellar peritenon in the patellar tendon group. No bone graft was placed in the patellar defect.
Postoperative Regimen
Most patients went home within 24 hours after surgery. All patients began an accelerated rehabilitation program of range of motion exercises and weightbearing as tolerated started by the end of the 1st week, with emphasis on maintaining knee extension. Closed kinetic chain exercises with bicycling were started approximately 2 to 3 weeks postoperatively. Running was started at 2 months and clearance for return to sports was given at 5 to 6 months after surgery. The rehabilitation program did not differ between the two groups.
Follow-up
Follow-up examinations were performed at 1, 6, and 12 weeks, 6 months, and annually thereafter by an independent examiner (not the surgeon). At the 2-year follow-up, the Lysholm score, Cincinnati knee score, Lachman test result, pivot shift test result, range of motion, thigh circumference, and KT-1000 arthrometer (MEDmetric Corp., San Diego, California) measurements were obtained. Patients were asked to rate their surgical results as excellent, good, fair, or poor. They were also asked whether they had any pain around the patella, reduction in activity level, whether the reduction was due to the reconstructed knee, and whether they would have the same procedure again.
The KT-1000 arthrometer examination was performed at 89 N, 134 N, and manual maximum. A test cycle was repeated until three successive tests indicated the same excursion (within 1 mm) and the dial returned to zero, as described by Daniel et al.6,7 Mean values were reported for differences in the measurements between the operated and contralateral sides. Three patients in the patellar tendon group and three patients in the hamstring tendon group had contralateral ACL ruptures and their KT-1000 arthrometer data were excluded.
Results
Of the 82 patients randomized, 70 patients (85.3%) had 2-year follow-up results. Three of the four patients with early graft failure underwent early revision ACL reconstruction. The fourth patient, from the patellar tendon group, with an atraumatic failure, had reflex sympathetic dystrophy and refused further treatment. Although the early revision cases were not suitable for formal testing, they were recorded as treatment failures and included as poor results.
The Lysholm score is a 100-point scoring system for examining patients’ symptoms, including locking, instability, pain, swelling, and ability to climb stairs and squat. The average Lysholm score at latest follow-up was 91.2 for the patellar tendon group and 92.3 for the hamstring tendon group (P = 0.6). The Lysholm score was greater than 84 points in 27 of 31 (87%) patients in the patellar tendon group and in 33 of 35 (94.%) patients in the hamstring tendon group (Table 4). With the two patients with graft failures from each group included as poor results, 82% of patients in the patellar tendon group had good or excellent results and 89% in the hamstring tendon group had good or excellent results.
Lysholm Scores in Patients with 2-Year Follow-up Data (Tested) and in All Patients Including Those with Graft Failure (Total)
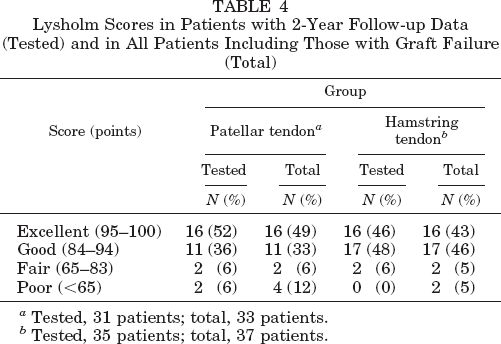
Tested, 31 patients; total, 33 patients.
Tested, 35 patients; total, 37 patients.
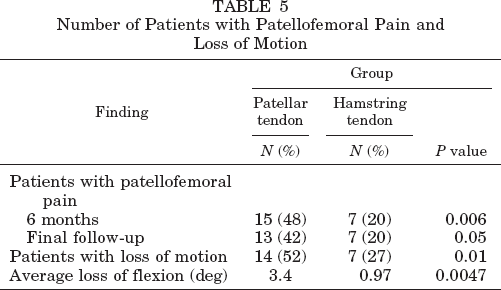
In the patellar tendon group, 14 of 27 (52%) patients had loss of motion of the reconstructed knee; the corresponding number in the hamstring tendon group was 7 of 26 (27%) (P = 0.01). Overall loss of motion averaged 3.4° in the patellar tendon group and 0.97° in the hamstring tendon group (range, 0° to 15°) (P = 0.0047). In those patients who had loss of motion, loss of flexion averaged 7.5° in the patellar tendon group and 4.8° in the hamstring tendon group. Only one patient, in the hamstring tendon group, had a loss of extension (5°) (Table 5).
Number of Patients with Patellofemoral Pain and Loss of Motion
Thigh atrophy was not significantly different between the groups. The thigh measurement side-to-side difference was less than 10 mm in 21 of 27 (78%) patients in the patellar tendon group and in 21 of 26 (81%) in the hamstring tendon group. The remaining patients had a 10- to 20-mm difference: 6 of 27 (22%) in the patellar tendon group and 5 of 26 (19%) in the hamstring tendon group.
Patients chose from four options when rating their ability to do hard cuts and pivots: normal, some limitation, limited to half normal, and limited to less than half normal. In the patellar tendon group, 19 patients rated themselves as normal, 6 as having some limitation, 1 as half normal, and 5 as less than half normal. In the hamstring tendon group, 22 patients rated themselves as normal, 8 as having some limitation, 2 as half normal, and 3 as less than half normal. All patients returned to cutting sports except four in the patellar tendon group and three in the hamstring tendon group. Overall, 45% in the patellar tendon group (13 of 31) and 37% in the hamstring tendon group (13 of 35) reduced their activities compared with their preinjury level. Four patients in the patellar tendon group (12.9%) and six in the hamstring tendon group (17.1%) stated that their reduction in activity was actually due to the reconstructed knee.
Patients were asked whether they had any pain around the patella at 6 months and at the last follow-up. At 6 months postoperatively, 15 (48%) of the patellar tendon patients had patellofemoral pain and 7 (20%) in the hamstring tendon group had pain (P = 0.006). At last follow-up, 13 (42%) in the patellar tendon group and 7 in the hamstring tendon group had patellofemoral pain (P = 0.05) (Table 5). One of the four patients in the hamstring tendon group who had a lateral meniscal repair had patellofemoral pain.
The KT-1000 arthrometer values for average side-to-side difference were 1.4 mm in the patellar tendon group and 2.4 mm in the hamstring tendon group when tested at 89 N (P = 0.08). The KT-1000 arthrometer results at 134 N were 1.8 mm in the patellar tendon group and 2.8 mm in the hamstring tendon group (P = 0.13). The manual maximum KT-1000 arthrometer results were 1.51 mm for the patellar tendon group and 2.5 mm for the hamstring tendon group (P = 0.13). The manual maximum KT-1000 arthrometer results were as follows: less than 3 mm side-to-side difference, 19 in the patellar tendon group and 10 in the hamstring tendon group; 3 to 5 mm, 2 in the patellar tendon group and 9 in the hamstring tendon group; more than 5 mm, 3 in the patellar tendon group and 3 in the hamstring tendon group. Overall, 21 of 24 (88%) patients in the patellar tendon group and 19 of 22 (86%) in the hamstring tendon group had less than 5 mm side-to-side differences on manual maximum testing, and 79% of the patellar tendon group and 45% of the hamstring tendon group had less than 3 mm differences. The six patients who had more than 5-mm side-to-side differences all rated their ability to do hard cuts, pivots, and jumping as normal or with some limitation, with most rating their ability to do these activities as normal. One of the six patients rated hard cuts and pivots as some limitation, and another patient rated jumping as some limitation. These patients were not considered to have treatment failures because of their otherwise good clinical outcomes (no complaints of instability), but their KT-1000 arthrometer scores were considered objective failures.
Preoperatively, the pivot shift test was positive in all patients. Postoperatively, the pivot shift was 1+ in five patients in the patellar tendon group and in four patients in the hamstring tendon group (pivot shift was 1+ in all six patients with KT-1000 arthrometer side-to-side difference of more than 5 mm). All remaining patients had a negative pivot shift test. The mean Lachman test before and after surgery changed from 2.3 to 0.35 in the patellar tendon group and from 2.4 to 0.4 in the hamstring tendon group. The average Lachman side-to-side difference postoperatively was 0.35 in the patellar tendon group and 0.48 in the hamstring tendon group.
The patients’ overall rating of their results was good or excellent for 30 (97%) in the patellar tendon group and for 35 (100%) in the hamstring tendon group. The four patients with graft failures were not asked to rate their surgery, but if these four are included in the poor results, the good or excellent values were 91% and 95%, respectively. In the patellar tendon group, 19 patients (61%) rated their surgery results as excellent, 11 (36%) as good, 1 (3%) as fair, and none as poor. In the hamstring tendon group, 28 patients (80%) rated their surgery results as excellent, 7 (20%) as good, and none as fair or poor. The difference in excellent ratings between the two groups was not significant (P = 0.09). All patients, except for the one with postoperative reflex sympathetic dystrophy, stated they would have the procedure again.
The two graft failures in each group occurred early, before 7 months postoperatively. Three of four failures were the result of early return to sports and traumatic rupture. In the hamstring tendon group, one patient had graft failure at 2 months after surgery while playing baseball and the other at 6 months after surgery during soccer. In the patellar tendon group, one graft failed at 6 months postoperatively while the patient was skiing. The other patient had a clinical diagnosis of reflex sympathetic dystrophy that was confirmed on bone scan and atraumatic failure of the graft. Physical examination showed a positive Lachman and pivot shift result at 6 months after surgery. The patient with atraumatic graft failure did not wish another ACL reconstruction, but the other three patients with graft failures underwent revision surgery before 1 year postoperatively.
Complications occurred only in the patellar tendon group. One was the previously mentioned reflex sympathetic dystrophy and another was a tibial interference screw infection that resolved without sequelae after removal of the screw. Arthrofibrosis occurred in one patient, who subsequently underwent manipulation under anesthesia. The final outcome was a 5° loss of flexion and no loss of extension. The Lysholm scores for the patient with the infection and the one with arthrofibrosis were both 89.
Discussion
Results of the present study showed no significant difference overall between patellar tendon and hamstring tendon grafts with respect to Lysholm score, Lachman and pivot shift test results, thigh circumference, return to sports, reduction in activity, jumping, and ability to do hard cuts and pivots. These results are consistent with those of other prospective randomized studies.1,12,18 The present study differs from other randomized studies in that soft tissue interference screws were used for the hamstring tendon graft placement and a single-incision technique was used for all procedures.
The only other study to use interference screw fixation for hamstring tendon grafts was by Corry et al. 4 In that nonrandomized study, good results were shown with both hamstring and patellar tendon grafts fixed with interference screws. The authors did exclude patients with significant meniscal tears and any chondral damage. One would expect these patients to have better symptomatic results and higher Lysholm scores than patients from the present study where more than 20% had chondral defects and more than 50% had meniscal tears; however, Corry et al. reported 86% good and excellent results based on the Lysholm scores in each group, which is very similar to our results. An important consideration in the study by Corry et al. is that graft lengthening (loosening) was not well addressed, because the KT-1000 arthrometer values were reported only for 89 N of force, which we believe is too low to differentiate loosening. Side-to-side differences under manual maximum forces can best ascertain the amount of graft loosening. 7 Their values at 89 N were 1 mm (patellar tendon graft) and 1.7 mm (hamstring tendon graft), and 91% of 64 patients with patellar tendon grafts and 79% of 79 patients with hamstring tendon grafts had less than a 3-mm side-to-side difference.
Daniel et al. 7 showed that manual maximum results are the most predictive of ACL tears. In patients with ACL-deficient knees who were not under anesthesia, the 20-pound anterior displacement difference revealed abnormal laxity in 62% of knees (33 of 53), compared with manual maximum force, which revealed abnormal laxity in 91% of knees (30 of 33). In large legs, the 20-pound (89 N) anterior pull is often not enough to produce any difference between the two knees, and manual maximum testing is often necessary to elicit a difference of 3 mm or greater, even in ACL-deficient knees. In the present study, of the five patients with patellar tendon grafts who had 3 mm or more side-to-side difference on manual maximum testing at final follow-up, only one patient had a 3-mm side-to-side difference at 89 N. The remaining four would be considered to have normal values at less than 3 mm if they were examined only at 89 N and not at manual maximum. Of the 12 patients in the hamstring tendon group with 3 mm or more side-to-side difference on manual maximum testing, 3 would have been considered to have normal values if tested only at 89 N.
Fifty-five percent of the patients with hamstring tendon grafts had 3 mm or more side-to-side difference on manual maximum testing, compared with 21% in the patellar tendon group. The two groups were almost equivalent when looking at those with more than 5-mm side-to-side difference (13% in the hamstring tendon group and 14% in the patellar tendon group). Patients with 3 to 5 mm of side-to-side difference on manual maximum testing had high Lysholm scores, and all of the patients in the hamstring tendon group rated their surgical result as good or excellent.
An important significant difference between the groups in the present study was that the hamstring tendon group had less patellofemoral pain than did the patellar tendon group at 6 months and at the most recent follow-up. In a study by Marder et al. 12 of 72 patients, the overall rate of patellofemoral pain (24%) was comparable with the rate in our study, and they found that almost twice as many patients with pain were from the patellar tendon group compared with the hamstring tendon group (11 versus 6). Other studies in which patellar tendon autografts have been compared with allografts have shown no difference in the occurrence of patellofemoral pain.14,24,28 Sachs et al. 22 found patellofemoral pain was related to flexion contracture and quadriceps muscle weakness. Both groups in this study began early range of motion exercises with emphasis on early extension, and only one patient lost extension (5°). Most patients had only mild patellofemoral pain and most had such pain only with exertion. A grading scale of patellofemoral pain would be highly useful to fully evaluate this important aspect of ACL reconstruction.
Loss of range of motion is a primary concern and may inhibit an athlete's ability to return to top performance. Loss of range of motion maybe a sequela of patellofemoral pain or may increase the risk of patellofemoral pain. We found small losses in range of motion, and in every patient (except one) the loss was in flexion rather than extension. Significantly more patients in the patellar tendon group than in the hamstring group lost motion (45% versus 17%). Shelbourne and Gray 23 recommend waiting 3 weeks after injury before ACL reconstruction to decrease the incidence of arthrofibrosis and loss of motion. Shelbourne et al.23–25 also showed an improved range of motion with an accelerated postoperative rehabilitation program. In the present study, no patient had surgery before 3 weeks after injury, and an accelerated rehabilitation program was used. In the study by Shelbourne and Gray, 23 27 of their 1057 (2.6%) patients in the accelerated program had torn their patellar tendon graft at an average of 2.5 years postoperatively. In the present study, 4 of 82 (4.9%) patients tore their ACL graft at a much earlier time (mean, 4.5 months postoperatively).
In our study there was a trend toward more patients in the hamstring tendon group than in the patellar tendon group rating their surgery result as excellent (80% versus 61%), although this difference was not significantly different. This finding may have been related to less patellofemoral pain in the hamstring tendon group and fewer patients with a loss in motion. Although the hamstring tendon group had a good end point on Lachman testing, they had higher numbers on KT-1000 arthrometer testing (not statistically significant). A potential benefit of the hamstring tendon graft is that its stiffness has been shown to be almost identical to that of the normal ACL, whereas the patellar tendon graft is about 3 to 4 times stiffer than the ACL. 16 If the graft is overtightened this can create a construct that is too stiff. A patient with an overconstrained knee may have a harder time regaining full range of motion. This lack of motion can lead to increased patellofemoral pain, as shown by Sachs et al. 22 Strength is also an important factor for return to sports. Because no difference in loss of strength has been shown in multiple studies between patellar and hamstring grafts, we did not examine strength in the present study.1,5,18
Strength of the autograft is an important consideration. Noyes et al. 16 found, in young fresh cadaveric specimens, that the central-third patellar tendon graft was the strongest graft of those tested (2900 N). The semitendinosus tendon graft strength was 1216 N but was only a single strand with a much smaller cross-sectional area than the patellar tendon. The area of the patellar tendon graft averaged 50.5 mm2 compared with the semitendinosus tendon at 14.0 mm2. Maximum stress (maximum load divided by initial cross-sectional area) was greatest in the semitendinosus and gracilis tendon and smallest in the iliotibial tract and quadriceps patellar retinaculum. The patellar tendon results were intermediate between these. Rowden et al. 21 tested graft strengths after a reconstruction of the ACL in young fresh cadavers. Double-looped hamstring tendon was stronger than the patellar tendon autograft by almost 40% (612 N versus 416 N). Stapleton et al. 27 found that fixation of the graft by the single-incision technique was 101 N stronger than fixation by the two-incision technique (694.5 versus 593.3 N). They believed this was due to the difference in graft fixation on the femur. For the single-incision technique, the interference screw is placed from an intraarticular, not extraarticular approach. They also found a wide range of strength depending on the size of the donor of the patellar tendon graft (435 to 905 N). This wide range of strength of a patellar tendon graft may help explain the large variation in pullout strengths in the literature.
Few studies of ACL reconstruction procedures have been published in which patients subjectively rated their surgical results. In the present study, all patients, except the four with graft failures and one patient in the patellar tendon group, rated their surgery as good or excellent. Noyes and Barber-Westin 15 had patients rate surgery on a scale from 1 to 10, with 5 and greater considered good, very good, or normal. Eighty percent (68 of 85) overall rated their result as good, very good, or normal. They compared early versus late ACL reconstruction, and 100% of the 30 patients with early reconstructions (<3 months between ACL tear and reconstruction) and 69% of the 55 patients with late reconstructions (>3 months) rated their outcome as 7 or greater (very good or normal). They found this to be a significant difference. Siegel and Barber-Westin 26 found after ACL reconstruction with hamstring tendon grafts that 92% of patients rated their surgery as normal or very good.
In retrospective studies comparing patellar tendon and hamstring tendon autografts, few significant differences were found overall.8,17,19 Otero and Hutcheson 19 reviewed 91 of 118 patients (55 patellar tendon grafts and 36 hamstring tendon grafts) and found no significant difference in Lysholm score, anterior knee pain, or KT-1000 arthrometer results at 2 and 3 years of follow-up. In their study, the hamstring tendon group had their leg placed in a cast for 4 weeks and 22 of the 55 patients with patellar tendon grafts had their knee immobilized for 3 weeks (the rest of the patients had early range of motion). The KT-1000 arthrometer results were higher for the patients with hamstring tendon grafts at 1 year, but not on subsequent follow-ups.
Interference screw fixation of patellar tendon grafts has been demonstrated to be superior to other fixation methods. 10 Interestingly, in vitro studies comparing the metal DonJoy RCI screw and bioabsorbable screws have found the bioabsorbable screws to be stronger.3,29 We did not find long-term healing and cutting of the hamstring tendon graft with interference screws to be clinically problematic in our study. Fixation was found to be adequate intraoperatively.
Basic science studies examining the histologic healing of soft tissue in a bone tunnel held by a screw are lacking. Rodeo et al. 20 showed that tendons (dogs) in a bone tunnel heal securely. Johnson 9 found that a semitendinosus tendon graft maintained gross and microscopic characteristics of the original tendon after ACL reconstruction with staple fixation. Lane et al. 11 examined a semitendinosus tendon autograft 4 years after an ACL reconstruction (harvested during total knee replacement) and found it to be similar to the native ACL. This study supports the concept of ligamentization of a double-looped semitendinosus tendon graft after placement into double tunnels.
Reduction in activity was found to be very high in both groups (45% in the patellar tendon group, 37% in the hamstring tendon group). Many patients had reduced activity because they no longer were in high school or college sports. Thus, they no longer were required to practice as often. Of the patients who stated the reduction in activity was due to the reconstructed knee (12.9% patellar tendon group, 17.1% hamstring tendon group), many were afraid of reinjury.
We found that hamstring tendon graft fixed with interference screws was not significantly different from patellar tendon graft for ACL reconstruction in terms of the patient's Lysholm score and ability to play cutting sports, but fewer patients with hamstring tendon grafts had patellofemoral pain. Interesting trends (not significantly different) identified in this study were that more patients in the hamstring tendon group rated their surgery as excellent (80% versus 61%), even though the KT-1000 arthrometer values were higher in this group. In the present study, 97% of the patellar tendon group and 100% of the hamstring tendon group rated their surgery as good or excellent. If patients with graft failures are included these numbers decrease to 91% and 95%, respectively. Lysholm scores were greater than 84 in 87% of the patellar tendon group and in 94% of the hamstring tendon group. These data show a very high satisfaction rate in patients with single-incision ACL reconstruction, regardless of whether the autograft was patellar or hamstring tendon.