
Abstract
Achilles tendon disorders are among the more common maladies seen by sports medicine physicians. Understanding the anatomy and biomechanics of the Achilles tendon and contiguous structures is essential to the diagnosis and treatment of Achilles tendon overuse injuries. Posterior heel pain is multifactorial and includes paratenonitis, tendinosis, tendinosis with partial rupture, insertional tendinitis, retrocalcaneal bursitis, and subcutaneous tendo-Achillis bursitis. Each of these entities is distinct, but they often occur in combination. Although most cases of this disorder are successfully treated nonoperatively, a small subgroup of recalcitrant cases may benefit from surgical intervention. Complete ruptures in active, athletic persons should be treated operatively in most cases and result in predictably good outcomes. There may be some cases that escape early recognition and require a reconstructive procedure to salvage a potentially severe functional deficit.
Anatomy
Since the time of Homer's Iliad, the name of Agamemnon's greatest warrior, Achilles, has been attached to the triceps surae tendon. As knowledge of the specific anatomy of this tendon was crucial to Achilles’ opponents’ success, so such knowledge is equally crucial to the orthopaedic surgeon in the management of Achilles tendon-related maladies, both acute and chronic in nature.
The Achilles tendon is a confluence of the gastrocnemius and soleus muscles. The gastrocnemius muscle is composed of a medial and lateral head. The medial head arises from behind the medial supracondylar ridge and adductor tubercle on the posterior surface of the femur. The lateral head arises from the lateral surface of the lateral condyle of the femur, proximal and posterior to the lateral epicondyle. Each of these heads has additional attachments from the posterior capsule of the knee joint and from the oblique popliteal ligament. 29 The soleus muscle lies deep to the gastrocnemius muscle, arising from the posterior surface of the upper tibia along the soleal line, the posterior aspect of the proximal third of the fibula, and from the intermuscular septum.
The medial and lateral heads of the gastrocnemius muscle gradually coalesce and incorporate into a broad, robust tendon in the posterior aspect of the lower leg. This tendon gradually narrows and becomes more rounded as it extends distally. The soleus muscle forms a broad tendon about midway down the leg, in a position deep to the tendon of the gastrocnemius. This tendon glides freely deep to the gastrocnemius muscle in its more proximal extent, thereby allowing independent movement of the two muscles.
The tendinous components of these two muscles are variable. The gastrocnemius component is the longer portion, contributing 11 to 26 cm. The soleus, in contrast, is shorter, containing a tendinous component from 3 to 11 cm in length. The width of the tendon at its point of insertion into the calcaneus varies from 1.2 to 2.5 cm. 29
Approximately 5 to 6 cm proximal to the calcaneal insertion, the independent tendons of the gastrocnemius and soleus fuse to become one tendon. At about 12 to 15 cm proximal to the insertion of the tendon, at about the level the soleus muscle begins to contribute fibers to the Achilles tendon, rotation of the tendon begins. This rotation becomes more marked in the terminal 5 to 6 cm of the tendon. The tendon spirals approximately 90° with the medial fibers rotating posteriorly and the posterior fibers rotating laterally.
The tendon inserts on the posterior surface of the calcaneus distal to the posterior-superior calcaneal tuberosity. 23 Deep to the tendon, proximal to the point of insertion, between the tendon and the calcaneus, is the retrocalcaneal bursa. The posterior wall of the bursa is formed by the tendon itself. Anteriorly, the bursa is bordered by a 0.5- to 1.0-mm thick cartilaginous layer on the posterior aspect of the calcaneal tuberosity. Proximally, the bursa is bordered by a synovial lining that separates the bursa from the proximal fat pad. 97 This fat pad rests anterior to the tendon and occupies an area bordered anteriorly by the flexor hallucis longus muscle, posteriorly by the Achilles tendon, and caudally by the superior aspect of the calcaneus. Superficial to the tendon lies a subcutaneous tendo-Achillis, or retrotendo-Achillis bursa between the tendon and the overlying skin.
Snow et al. 109 evaluated the Achilles tendon insertion and its relation to the plantar fascia. They found that the neonate has a thick continuation of fibers of the tendinous insertion into the plantar fascia. This continuity gradually diminishes with age and the thick continuation of fibers of the neonate becomes solely a connection of superficial periosteal fibers in the middle-aged foot. The foot of the elderly patient appears to have separate insertions altogether, with periosteum between the Achilles tendon and the plantar fascia. This finding indicates that, in the management of heel pain, stretching regimens of the Achilles tendon and plantar fascia appear to alleviate insertional stresses rather than relieve stresses on a contiguous structure connecting the Achilles tendon and plantar fascia.
The Achilles tendon is not encased in a true synovial sheath but is encased in a paratenon made up of a single layer of cells. This paratenon anteriorly consists of fatty, mesenteric-like areolar tissue. This tissue is richly vascularized and is responsible for a significant portion of the blood supply to the tendon. 20 This supply comes through a series of transverse vincula, which function as passageways for blood vessels to reach the tendon. In addition to these mesotenal vessels, the blood supply to the tendon comes from two other sources: the musculotendinous junction and the osseous insertion. Angiographic studies have shown that the area of most tenuous blood supply is 2 to 6 cm proximal to the insertion in the calcaneus. 24 Additionally, the number of intratendinous vessels and the relative area occupied by these vessels is lowest 4 cm from the calcaneal insertion. 104
Although not classically considered part of the Achilles tendon, the plantaris muscle anatomy should be discussed because of its intimate relationship with the Achilles tendon and its frequent use in operative management of chronic Achilles tendon tears. The plantaris muscle originates from the lowest part of the lateral supracondylar ridge, the adjacent area of the posterior surface of the femur, and the knee joint capsule. The tendon of the plantaris crosses obliquely from lateral to medial in a depression in the soleus muscle. It continues its course distally between the gastrocnemius and soleus muscles, emerging on the medial side of the Achilles tendon 12 cm from the Achilles insertion to the calcaneus. Cummins et al. 29 studied 200 cadaveric specimens and noted four patterns of insertion of the plantaris tendon. The plantaris tendon inserts most commonly (47%) via a fan-shaped expansion into the medial aspect of the insertion site of the calcaneal tuberosity of the Achilles tendon. Occasionally, thin slips of fascial strands may extend from the plantaris tendon to the medial border of the Achilles tendon. In the second most frequent pattern (36.5%), the plantaris tendon inserts into the calcaneus 0.5 to 2.5 cm anterior to the medial border of the Achilles tendon. The third most common pattern (12.5%) demonstrates a broad insertion along the dorsal and medial surfaces of the Achilles tendon. In the least common finding (4%), the plantaris tendon inserts into the medial border of the Achilles tendon from 1 to 16 cm proximal to the Achilles insertion into the calcaneus. The plantaris tendon is absent in 7.05% of people as tabulated from the literature. 29
Biomechanics
The gastrocnemius muscle and soleus muscle, via the Achilles tendon, function as the chief plantar flexors of the ankle joint. In walking as well as in running and jumping activities, this musculotendinous unit provides the primary propulsive force for locomotion. Whereas the gastrocnemius muscle functions primarily as a plantar flexor at the ankle, the soleus muscle has a postural role as well, preventing the body from falling forward during standing. Contraction of this musculotendinous unit also functions to flex the knee and supinate the subtalar joint.
The gastrocnemius and soleus musculotendinous unit function during the second and third intervals of the stance phase of the gait cycle. 114 During the second interval, extending from 15% to 40% of the gait cycle, the activity in the posterior calf musculature is mainly directed at controlling the forward movement of the tibia over the planted foot. At about 34% of the gait cycle, heel rise begins. The third interval of the gait cycle extends from 40% to 62%. During this interval there is rapid plantar flexion of the ankle joint due to concentric contraction of the triceps surae muscle. 78 Komi et al. 54 performed an in vivo evaluation of the Achilles tendon force during ambulation. They demonstrated that after heel strike there is an initial silent period of force in the Achilles tendon, and that there is a rapid increase in force leading to a peak at the end of the push-off phase. This is consistent with the triceps surae muscle activity demonstrated by Mann 78 during the third interval of the stance phase of gait.
At the end of the stance phase in normal walking, muscle tension through the Achilles tendon is estimated at 250% of body weight. 99 Studies using both implanted electrodes and biomechanical force analysis have demonstrated that the Achilles tendon force during running approaches 6 to 8 times body weight, a load close to the ultimate strength of the tendon.5,24
The 90° spiral of the Achilles tendon is believed to explain some of the seeming elastic qualities of the tendon. When landing from a jump, the body will remain upright while the foot attains a plantar flexed position due to activity in the triceps surae muscle. On landing, the strain is absorbed by the Achilles tendon, which produces a recoil effect. 97
Because of the Achilles tendon's insertion into the calcaneus, the tendon can be exposed to forces secondary to subtalar motion. This is particularly notable in the hyperpronated or cavus foot and in runners who pronate. It is believed that a hyperpronated or cavus foot may lead to a greater chance of rupture of the Achilles tendon because of the diminished shock absorption associated with these malalignments. 5 James et al. 45 have implicated this functional overpronation as a causative factor in noninsertional Achilles tendinitis as well. The foot pronates during the midstance phase, leading to an internal rotation force on the tibia. With extension of the knee, an external rotation force is applied to the tibia. It is believed that during midstance with the foot pronated and the knee in extension, there are contradictory rotational forces that present themselves across the Achilles tendon and are directed toward the Achilles tendon insertion.24,45,89,104 Arndt et al. 7 demonstrated that activation of the triceps surae muscle results in a tensile force, leading to plantar flexion. They showed that an eversion moment could be created by isolated activity of the lateral head of the gastrocnemius muscle; however, all other patterns of firing of the triceps surae muscle led to an overall inversion moment. 7 This inversion moment may contribute additionally toward the increased stress across the Achilles tendon during the period of midstance with the foot pronated and the knee extended.
Achilles Tendon Overuse Injuries
The term “Achilles tendinitis” has previously been used for any pain in the posterior part of the heel. This term is misleading because it implies an inflammatory pathologic process within the tendon itself. It has been well established that there are several pathologic conditions that cause posterior heel pain.9,26,34,58,59,61–63,67,106 The literature is confusing in regard to the classification of Achilles tendon overuse injuries. For example, there are many terms given for the same type of pathologic entity denoting inflammation of the paratenon (such as tenosynovitis, tenovaginitis, peritendinitis, or paratenonitis). Furthermore, various pathologic conditions sometimes coexist (for example, paratenonitis with tendinosis), making the distinction between these various classifications somewhat vague. The authors prefer a modification of the classification as set forth by Puddu et al., 101 which is presented in Table 1.
Classification of Achilles Tendon Disorders a
According to the classification of Puddu et al. 101
With more than 10% of the American adult population participating in running today, as well as increasing participation in other running and jumping sports, posterior heel pain and Achilles tendon injuries are among the more common entities seen by sports medicine physicians.
Contributing Factors
In runners, the most common cause of Achilles tendon injuries is training errors, including sudden increase in training mileage or intensity, or both, a change of terrain (particularly hill running), an increase in interval training, or a solitary intense run. Biomechanical factors have also been shown to come into play with these injuries.17,25,28 A cavus foot as well as a flat foot with excessive pronation has been implicated. The motion of the hindfoot going from a supinated to a pronated position and then back during the running gait cycle creates a “whipping” action on the Achilles tendon, which creates shear forces across the Achilles tendon, placing particularly high eccentric stresses on the medial side of the tendon. Malalignment factors above the ankle, such as genu varum, can also contribute to increased stress on the Achilles tendon.
Paratenonitis
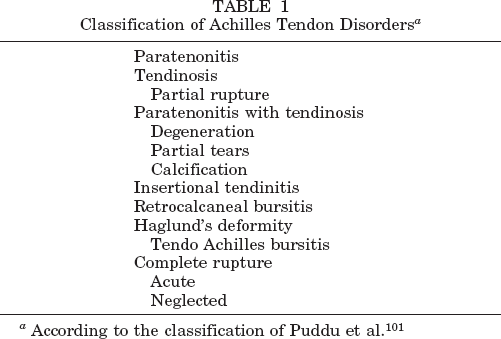
The paratenon of the Achilles tendon is composed of a single layer of cells that has a variable structure. This layer is better termed a “tenovagium” rather than tenosynovium, which implies a double-layered sheath lined by synovial cells. 25 The ventral paratenon consists of fatty mesenteric-like areolar tissue that is rich in blood vessels that nourish the tendon. Paratenonitis is accompanied by diffuse discomfort and swelling within the tendon. In acute cases, the tendon appears “sausage-like” because of its diffusely swollen, edematous condition, and crepitation is often noted (Fig. 1). 62 This is commonly encountered acutely in marathon runners. Usually there is palpable tenderness on both sides of the tendon, but the medial side is more commonly involved than the lateral side. In some cases, tender nodules form within the paratenon, representing localized hypertrophy and connective tissue proliferation. The involved area may either be over a segment of several centimeters or it can involve the entire tendon sheath from the insertion to the muscle. Paratenonitis may result from abnormal biomechanics, but it can occasionally occur because of extrinsic pressure causing friction between the Achilles tendon and its adjacent sheath, often from poor-fitting shoes, although this is more likely to cause subcutaneous tendo-Achillis bursitis. Although symptoms are typically aggravated by activity and relieved by rest, runners often complain of stiffness and pain at the beginning of their run and then are able to “run through” the discomfort. However, if left untreated, symptoms may increase to the point that running is no longer possible.

Acute paratenonitis: note the diffuse, circumferential swelling involving the entire tendon sheath, from the insertion up to the musculotendinous junction. Crepitus will be noted on palpation with ankle movement as well.
Tendinosis
Although painful areas of the Achilles tendon are commonly called “Achilles tendinitis,” this term is actually a misnomer. Histologically, these areas of the tendon are characterized by a degenerative noninflammatory process that is best termed “tendinosis.” 25 These areas in the tendon consist of mucinoid or fatty degeneration with a disorganized collagen structure. These degenerative changes in the tendon seem to be related to the normal aging process and will usually eventually be present in all persons to some degree. 113 These changes do not necessarily progress to clinical symptoms. Interestingly, these histologic changes may be seen in young patients as well. The symptoms of Achilles tendinosis may be secondary to microtrauma or failure of this degenerative tissue, leading to partial tears and subsequent symptoms. Kannus and Jozsa 50 have demonstrated the degenerative changes that are found in ruptured tendons soon after their spontaneous failure. Tendons that are subjected to high eccentric or stretching stresses, such as the Achilles tendon, seem to be most susceptible. Therefore, abnormalities within the tendon itself that lead to symptoms should best be termed Achilles tendinosis. Puddu et al. 101 have documented histologically that long-standing degeneration can exist in the absence of clinical symptoms but may become symptomatic with heavy training, leading to localized pain, tenderness, and thickening in the tendon. The onset of symptoms is usually gradual, but well localized to an area within the mid-third of the tendon. A nodule develops within the tendon and is more commonly seen on the medial side, where the tendon experiences its highest eccentric and shear stresses. This area is also the most hypovascular zone of the tendon. In many cases, the onset of symptoms is related to a partial rupture or series of microruptures in the area of degeneration. 69 A history of transient sharp pain or repeated episodes of sharp pain within the tendon while running should alert the physician to the possible presence of a partial rupture. These patients will have a localized medial thickening of the tendon (Fig. 2). The pain is usually exacerbated by loaded dorsiflexion of the foot, and there is often limited dorsiflexion. 105 In rare cases, heterotopic ossification can occur within the tendon itself. 70 In the authors’ experience, middle-aged men who suddenly increase their activity level or resume strenuous activity after a long period of inactivity seem to be most susceptible to developing micro or partial ruptures within an area of preexisting tendinosis. If the degenerative process is extensive, leading to repetitive partial ruptures, the tendon may actually elongate and not function well in continuity with a paradoxical increase in passive dorsiflexion. 90 Åström and Rausing 10 studied a series of 342 operative cases of tendinosis (81% were male patients). A partial rupture was found in 23%, tendinosis in 49%, and no macroscopic abnormalities in 28% of the tendons. They found that the lesion was more common in the distal part of the tendon; predisposing factors were physically active lifestyle, age slightly below middle-age, and, particularly, local steroid injection before surgery.
Tendinosis with chronic partial rupture. An asymmetrical, nodular thickening of the tendon, more commonly seen on the medial (tension) side of the Achilles tendon.
Retrocalcaneal Bursitis
Retrocalcaneal bursitis is a distinct entity hallmarked by pain that is anterior to the Achilles tendon and just superior to its insertion on the os calcis. The retrocalcaneal bursa, which lies between the anterior aspect of the tendon and posterior aspect of the os calcis, becomes inflamed, hypertrophied, and adherent to the underlying tendon. This may be associated with a prominence of the posterosuperior angle of the os calcis. Patients with retrocalcaneal bursitis will have a positive two-finger squeeze test. Pain is elicited by applying pressure both medially and laterally with two fingers just superior and anterior to the Achilles insertion at about the level of the posterosuperior angle. This entity should be distinguished from inflammation of the subcutaneous tendo-Achillis bursa lying between the posterior aspect of the tendon and the skin that occurs secondary to an abrasive heel counter or high-heeled shoes. When this entity is bilateral, the clinician should always exclude the possibility of a systemic inflammatory disease. There is an association of retrocalcaneal bursitis with rheumatoid arthritis seen in up to 10% of patients with this disease. 120
Many studies have been made of the morphologic variations of the posterior calcaneal seen in association with retrocalcaneal bursitis. The three most common variations in the shape of the superior tuberosity of the calcaneus are hyperconcave, normal, and hypoconcave. Although prominence of the posterior tuberosity has been associated with retrocalcaneal bursitis, it is well known that it is not uncommon to find retrocalcaneal bursitis in runners without any associated calcaneal deformity. Compression of the bursa between the calcaneus and the Achilles tendon occurs every time the ankle is dorsiflexed, and in a runner the repetitions are countless, particularly with uphill running where ankle dorsiflexion is increased. Thus, it is not surprising that long-distance runners who use uphill running as a training method frequently develop this clinical entity. Other biomechanical abnormalities that are associated with the development of retrocalcaneal bursitis include rearfoot varus and a rigid plantar flexed first ray.
The retrocalcaneal bursa is a significant structure that is horseshoe-shaped and 4 mm in width and 8 mm in depth. 99 Its anterior surface is composed of fibrocartilage and its posterior boundary blends in with the paratenon. It contains 1 to 2 mm of bursal fluid. In some cases, the fluid in the bursa can actually become ballottable. There is usually some element of contiguous inflammation in the sheath or at the Achilles tendon insertion. The pain is typically aggravated by dorsiflexion of the ankle.
Haglund's Deformity
Prominence of the posterosuperior lateral aspect of the calcaneus causing irritation of the bursa (both the retrocalcaneal and the adventitial bursa), particularly from a poor-fitting shoe, has been termed “Haglund's deformity.” 107 This entity often goes hand-in-hand with retrocalcaneal bursitis and frequently there is an element of insertional tendinitis as well. The term “pump bumps” has also been used to describe this condition. Often this pump bump is asymptomatic, but it may become symptomatic from a poor-fitting shoe or an irritating heel counter. This tender prominence is typically present on the lateral side of the Achilles tendon insertion, not directly on its central portion. Although this is more commonly found in women who wear high-heeled shoes, in the athletic population it is sometimes found in hockey players who wear a rigid heel counter that causes irritation. The patient population that has this superolateral bone prominence tends to be younger than the patients with retrocalcaneal bursitis. These patients likewise often have an element of retrocalcaneal bursitis, tendo-Achillis bursitis, as well as insertional tendinitis. Multiple studies have attempted to delineate Haglund's deformity radiographically by looking at the height, length, and the angular relationships of the calcaneus. In our experience, none of these views have been very helpful or reliable in making a diagnosis or planning treatment, and the authors cannot recommend one particular radiographic view as being consistently helpful in demonstrating this bony prominence.
Numerous biomechanical risk factors have been associated with Haglund's deformity, including a high-arched cavus foot, rearfoot varus, rearfoot equinus, and trauma to the apophysis in childhood.28,45,55 It is important in these cases to look for associated retrocalcaneal bursitis, as well as insertional Achilles tendinitis.
Insertional Tendinitis
Patients with insertional tendinitis have a true inflammatory reaction within the tendon. These patients have direct tenderness over the Achilles tendon insertion, often associated with calcification or spurring within or in juxtaposition to the tendon just above its insertion on the superior aspect of the calcaneus. It must be emphasized, however, that the Achilles tendon does not actually attach to these spurs since it is contiguous with the whole posterior wall of the calcaneus. There is a high association of insertional tendinitis with retrocalcaneal bursitis or Haglund's deformity. The athlete typically complains of pain directly at the insertion of the Achilles tendon that is initially worse after exercise but may eventually become constant. As in other conditions with the Achilles tendon, it is frequently aggravated by hill running and interval training. Training errors are also common in this group when there is a sudden increase in mileage and improper stretching techniques. Insertional tendinitis is also seen in heel runners. Running on hard surfaces also tends to aggravate the pain.
On physical examination, the tenderness is localized at the Achilles tendon insertion. Insertional tendinitis is frequently aggravated by passive dorsiflexion. Loss of passive dorsiflexion is common in this group. 105 Radiographs frequently demonstrate calcification or ossification coming off the superior portion of the calcaneus and the upper part of the insertion of the Achilles tendon. These changes, however, are often seen incidentally as part of the normal aging process, and clinical correlation is paramount before assuming that the patient's symptoms are secondary to these abnormalities shown on radiographs. Often, these radiographic changes can be seen bilaterally, although the patient's clinical complaints may be only for one side. Patients with insertional tendinitis are usually older than patients with paratenonitis or Haglund's deformity.
Imaging
Plain radiographs are only occasionally of any value in determining treatment for any of these predominantly soft tissue injuries. In rare cases of long-standing tendinosis with or without partial rupture, ossification may be seen within the tendon. Plain radiographs are more helpful in evaluating patients with retrocalcaneal bursitis, Haglund's deformity, and insertional tendinitis, not only to delineate the morphologic characteristics of the posterosuperior aspect of the calcaneus, but also to look for any ossification or osteophytes at the Achilles tendon insertion.
The two imaging techniques that best demonstrate abnormalities within the Achilles tendon are ultrasonography and MRI. 86 Sonography seems to play a larger role in European countries, particularly in Scandinavia, whereas MRI appears to be the test of choice for most clinicians in the United States. These imaging techniques seem to be most helpful in delineating abnormalities within the Achilles tendon itself, as well as imaging of the retrocalcaneal bursa. Ultrasonography is much less expensive than MRI and also allows for dynamic examination. It is, however, very examiner-dependent, and reliability appears to correlate with the experience of the examiner. Kälebo et al. 49 compared sonographic findings in 37 patients who subsequently underwent surgery for Achilles tendon disorders. In particular, they looked at the reliability of diagnosing partial ruptures of the Achilles tendon and found that ultrasound had a sensitivity of 0.94, a specificity of 1.00, and an accuracy of 0.95. Paavola et al. 96 found that ultrasonography was reliable in delineating focal lesions within the Achilles tendon, but they concluded that it was inaccurate for differentiating partial rupture from a focal area of tendinosis. They did note, however, that ultrasonography was not completely reliable for diagnosing paratenonitis and tendinitis unassociated with a lesion within the tendon itself. For diagnosing retrocalcaneal bursitis, they found ultrasonography to be accurate in six of eight cases.
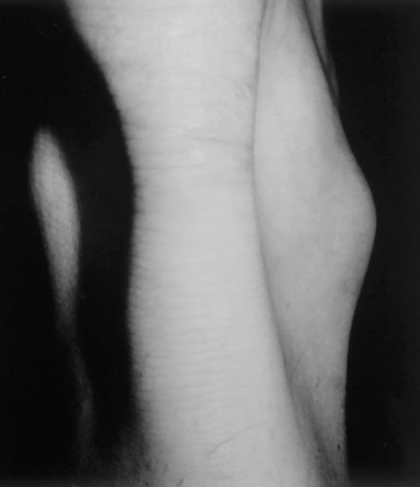
Magnetic resonance imaging has been shown to be extremely helpful in the preoperative evaluation of Achilles tendon overuse injuries. This modality is extremely sensitive to pathologic changes that occur within the tendon as a result of tendinosis, partial rupture, or both. Particularly in smaller areas of intrasubstance degeneration that are not clinically palpable, MRI can help localize foci that require exploration and debridement. Marcus et al. 80 noted an excellent correlation between MRI and pathologic findings at the time of surgery, which has also been our experience. 106 Magnetic resonance imaging is extremely sensitive to pathologic changes within the tendon (Fig. 3). Again, clinical correlation is paramount, as areas of increased signal seen on MRI may in some cases represent incidental areas of asymptomatic degeneration similar to those seen in the menisci or the supraspinatus muscle that may not be clinically significant. Our examination protocol includes 2-mm slices taken in both T1- and T2-weighted images in the axial and sagittal planes.
Axial MR image of the midsubstance of the Achilles tendon in a patient with tendinosis. Note the areas of high signal within the tendon (arrow).
In patients with paratenonitis, even in chronic cases with significant thickening and fibrosis of the paratenon, MRI has not been reliable in demonstrating pathologic changes within the sheath, and we have found that surgical correlation is poor in these circumstances. 106 In these cases, MRI is only helpful in ruling out abnormalities within the tendon itself. Retrocalcaneal bursitis demonstrates a high signal within the retrocalcaneal bursa and is best seen on T2-weighted images (Fig. 4). It is also helpful for delineating contiguous changes within the tendon and tendon insertion itself in juxtaposition to the bursa. Magnetic resonance imaging is also helpful in demonstrating any degenerative and inflammatory changes within the tendon insertion in patients with insertional tendinitis. Again, as in all diagnostic studies, correlation of positive MRI findings with clinical symptoms is paramount.

Retrocalcaneal bursitis. Sagittal MR image demonstrating high signal within the retrocalcaneal space associated with an osteophyte and prominence of the posterior superior angle of the calcaneus (arrow).
Conservative Management
Most cases of Achilles tendon overuse injuries and posterior heel pain are successfully managed nonoperatively. Training errors are the most common cause of Achilles tendon overuse injuries. 57 Rest or modification of activities should always be part of the initial treatment. The decision whether to recommend complete cessation of any running or athletic activities versus modifying the running program should be individualized and based on the severity of the problem and the duration of symptoms. A cross-training program that includes stationary bicycling, water therapy, and aqua jogging will usually allow the athlete to remain fit while allowing symptoms to resolve. As the symptoms improve, progression to machines that replicate cross-country skiing and stair-climbing can be used as a transitional step before resuming running activities.
In milder cases of Achilles tendon overuse injuries, a decrease in weekly mileage can be recommended as initial treatment. We usually recommend cutting back to 25% of the usual mileage level and then increasing by about 10% per week, depending on symptoms. A temporary cessation of interval training and hill workouts should also be recommended, as these are particularly stressful on the Achilles tendon. In a runner training on a hard or banked running surface, the recommendation should be to train on a flat, softer surface. A quarter- to half-inch heel pad built into the running shoe may also be useful in reducing stress on the tendon. In acute cases, particularly when there is an inflammatory component involved, such as in paratenonitis or retrocalcaneal bursitis, a course of oral antiinflammatory medication may prove useful.
In addition to nonsteroidal antiinflammatory medications, ice massage in acute cases and contrast treatments in subacute and chronic cases can be helpful. A course of physical therapy, combining modalities with stretching and strengthening exercises, is usually beneficial. In severe cases, the use of ultrasound sometimes with the delivery of topical steroids, known as phonophoresis, can be useful. We have found that most patients with chronic symptoms have limited passive dorsiflexion. 105 Gentle stretching exercises done in a passive, static manner are most helpful. In acute cases, it is important for the athlete not to “overstretch” and thereby increase symptoms. Stretching should be performed before and after exercise with the knee extended as well as flexed, as well as with the guidance of the physical therapist. In some cases, a night splint for a period of 6 to 8 weeks in a dorsiflexed position is helpful to maintain and enhance passive dorsiflexion.
Biomechanical and alignment problems are frequently associated with Achilles tendon overuse injuries. If there is a foot alignment problem, orthoses that place the hindfoot in a neutral position are appropriate. Excessive pronation may place abnormal stresses on the tendon, producing a whipping action on the tendon during the running stride. 28 In a study on the effectiveness of orthotic shoe inserts in the long-distance runner, Gross et al. 38 looked at 347 long-distance runners who had used or were using orthotic shoe inserts for symptomatic relief of lower extremity complaints. More than 18% of these patients had a diagnosis of Achilles tendinitis. Almost 75% of these patients had either a complete cure or great improvement as a result of the orthotic shoe insert. Any minor leg-length discrepancy should also be corrected by orthotic inserts. These orthotic devices seem to be most successful in patients who have either excessive pronation or leg-length discrepancy or both. In our experience, a full-length, flexible or a semirigid, as opposed to a rigid, orthotic device seems to work the best. Most runners or athletes will continue to use the orthoses after symptoms have resolved. The use of a shock-absorbing insole can also be helpful, particularly if the runner is running on hard surfaces.
After addressing training errors, alignment problems, and flexibility issues, a program of strengthening should be initiated, as most of these patients will have some calf muscle weakness. Aggressive strengthening performed before acute symptoms have resolved may exacerbate the problem, and so should be appropriately timed. Electrical stimulation and isometric exercises are initially recommended, gradually progressing to isotonic and then eccentric strengthening. In a study evaluating the effectiveness of heavy-load eccentric calf muscle strengthening for the treatment of chronic Achilles tendinosis, Alfredson et al. 4 prospectively studied the results of eccentric strengthening in 15 athletes who had a diagnosis of chronic Achilles tendinosis with a long duration of symptoms, despite conventional nonsurgical management. They compared this group with a group of 15 athletes with the same diagnosis of the same duration who had been treated with conventional measures. Before the exercise program, most of the patients had significantly lower calf strength on the injured compared with the noninjured side. After 12 weeks of increasing-load eccentric calf muscle-strengthening exercises, all 15 patients were back to their preinjury running levels with full running activities. Of the other 15 athletes treated with conventional measures, only one had resolution of symptoms. Our policy is to include an eccentric strengthening program as the final phase of rehabilitation before resumption of running or athletic activities.
In subacute or chronic cases of refractory paratenonitis, occasionally “brisement” (distention of the paratenon-tendon interface) can be useful. This is particularly useful if there is audible crepitus and “squeaking” with ambulation that has not improved. Johnston et al. 46 have recommended the use of 5 ml of 0.25% bupivacaine, with a permanent resolution of symptoms and disappearance of crepitus in three of nine patients. Jones 47 recommended the use of 15 ml of local anesthetic injected into the subparatenon space. Brisement can also be performed with saline and, if available, ultrasound guidance can be helpful to ensure proper placement of the needle. A corticosteroid solution should not be used for this procedure.
The authors, as well as others, have found that the use of injectable steroids is contraindicated as it may lead to tendon rupture; however, we have found that in refractory cases of retrocalcaneal bursitis, a one-time steroid injection directly into the retrocalcaneal bursa is sometimes helpful. Extreme care must be taken not to inject any steroid solution into the tendon, and it is important that only one injection be used. In an occasional case, one may be able to aspirate bursal fluid from the bursa itself before injection of corticosteroid. Although the use of steroid injection in refractory cases before resorting to surgery can be tempting, multiple studies have delineated the deleterious effects of injecting the corticosteroid solution into the Achilles tendon. Åström and Westlin 11 studied a group of patients who had a partial rupture and a history of chronic Achilles tendon symptoms. In a logistic regression analysis, only preoperative steroid injections in men were predictive of a partial rupture. Furthermore, in highly competitive athletes who have been known to use anabolic steroids, either oral or injectable, it has been reported that the use of anabolic steroids produces a stiffer tendon that absorbs lower loads before failure and fails with less elongation. 43
Surgical Management
Although nonoperative management of Achilles tendon overuse injuries is usually successful in getting patients back to activity, there will be a small group of patients who continue to be symptomatic, despite the measures previously outlined. In particular, competitive and serious recreational runners who would like to continue running may seek a surgical solution after other measures have failed. Preoperative planning and exact delineation of the cause of the symptoms is crucial. Often these entities occur in combination (for example, paratenonitis with tendinosis, or retrocalcaneal bursitis with insertional tendinitis). In our initial review of 45 surgical cases, we found 7 patients (15%) actually had a combination of retrocalcaneal bursitis along with more proximal paratenonitis or tendinosis, or both. 105
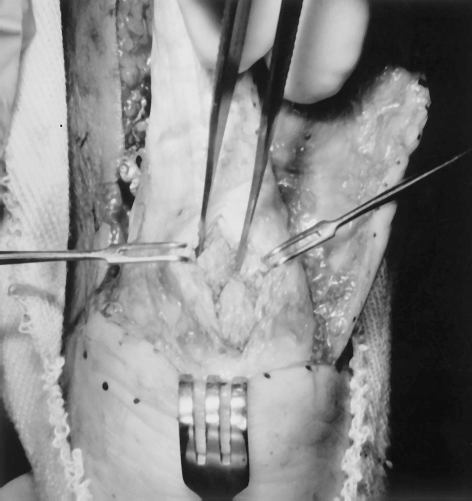
In our surgical treatment method, we use a longitudinal approach made 1 cm medial to the Achilles tendon to avoid the sural nerve. The length of the incision varies according to the extent and site of primary abnormality. In most cases of paratenonitis or tendinosis, the incision spans from the musculotendinous junction to just above the insertion. In cases of retrocalcaneal bursitis, where exposure of the retrocalcaneal bursa and the posterior aspect of the calcaneus is necessary, it is essential to have exposure from both sides. Our original approach was to perform a skin incision that continued transversely from medial to lateral below the Achilles insertion in a J-shaped fashion. Subsequently, we have converted to a more conventional double-incision technique, making a smaller longitudinal lateral incision on the lateral side of the retrocalcaneal bursa and carefully avoiding the sural nerve. This second incision should leave a skin bridge of at least 4 cm; we have not had problems with skin necrosis using this technique. Dissection should be carried directly down to the Achilles paratenon, and a full-thickness flap should also be created by dissecting between the Achilles tendon and the paratenon, and not above this layer. This is paramount to preserve blood supply to the skin flap, particularly in older patients. In cases of chronic paratenonitis, the tendon sheath is usually found to be hyperemic, thickened, and adherent to the underlying tendon (Fig. 5). By sharp dissection, the involved tissue is freed from the underlying tissue and excised. We are careful not to excise the anterior portion of the paratenon or disturb the anterior fatty tissue for fear of jeopardizing the blood supply to the tendon. A complete circular dissection could also potentially lead to extensive postoperative fibrosis.

Chronic paratenonitis. The paratenon is markedly thickened and fibrotic, requiring sharp dissection off the tendon. Care should be taken not to disturb the anterior soft tissues.
In cases of tendinosis or partial rupture, or both, often the thickened area of the abnormality is obvious. In more central or subtle cases, the tendon should be carefully inspected and palpated for areas of thickening, defects, or softening. This is where preoperative MRI can be very helpful in delineating areas of tendon degeneration or rupture that are not clinically palpable (Fig. 6). If there is no clinically palpable defect or nodule within the tendon and a well-done MRI does not demonstrate any echogenic signal changes within the tendon, an exploratory splitting incision within the tendon is usually not warranted.

Clinical case of tendinosis. A longitudinal splitting incision has been made, revealing extensive diffuse mucinoid degeneration within the tendon.
In those patients where the tendon substance is involved, a longitudinal splitting incision is made within the tendon at the site of the abnormality. The foci of symptomatic degeneration should be completely excised. Histologically, this will usually represent areas of mucinoid degeneration. The abnormal scar tissue has a different consistency, usually harder and nodular, and appears disorganized in reference to the surrounding normal tendon. All abnormal tissue should be excised.
Maffulli 73 recommends exploration by three to five longitudinal tenotomies with excision of the abnormal tissue. In another study by Maffulli et al., 75 they described a percutaneous technique using a No. 11 blade inserted parallel to the long axis of the tendon fibers in marked symptomatic areas and then plantar flexing and dorsiflexing the foot, creating a 3- to 4-cm area of tenolysis obtained through this percutaneous incision. This is repeated four to five times in the surrounding quadrants of the tendon.
When a longitudinal splitting incision is made in the tendon, care should be taken to use a minimal amount of suture in closing the tenotomy. The use of excessive synthetic absorbable sutures can initiate an extensive fibrotic reaction in the tendon, creating fibrosis and thickening. 106 Maffulli et al. 75 recommend not closing the longitudinal tenotomies at all.
In cases of extensive tendinosis or partial rupture, or both, the decision as to when to perform a reinforcement of the tendon remains controversial. In our retrospective long-term study, 106 the area of partial rupture did not require reinforcement in most cases. In fact, many of the patients with these symptoms will have marked thickening of the tendon so that after debridement the tendon may have a more normal diameter in comparison with the contralateral, unaffected side. Based on our clinical experience, we have developed an algorithm for surgical management of tendinosis or partial ruptures of the Achilles tendon. In cases of moderate deficiency (20% to 40%), we would reinforce the tendon with either a turn-down flap or a plantaris patch. In cases where there is 50% to 75% involvement of the tendon, augmentation is necessary. This can be either in the form of a direct augmentation with the use of autograft (such as semitendinosus or gracilis tendon graft) or, more recently, we have used allograft tendon with less morbidity and equally good results.
If more than 75% of the tendon is involved and there is very little normal substance left, autogenous tendon transfer or reconstruction with the use of allograft is indicated. Mann et al. 79 reported on seven patients in whom they performed a transfer of the flexor digitorum communis tendon for chronic rupture of the Achilles tendon. They believe there is an advantage in using this tendon instead of the peroneus brevis because it brought in a richer vascular supply, allowing retention of plantar flexion as well as a more biomechanically correct insertion into the calcaneus. They believe the use of the peroneus brevis muscle changes the balance between the invertor and evertor muscles. In their study, however, all patients had gross incontinuity of the tendon, and most patients were in their 6th and 7th decades of life.
Hansen 40 has recommended the use of the flexor hallucis longus muscle for treating prerupture syndrome of the Achilles tendon. He recommends splitting the Achilles tendon and inserting the muscle belly of the flexor hallucis longus muscle to improve the blood supply to the Achilles tendon. We believe that this procedure helps correct the vascular insufficiency in the tendon. Concerns must be raised about the transfer of the flexor hallucis longus muscle in an athlete, particularly in a runner, as there is an effect on the flexion strength of the first interphalangeal joint. The biomechanical imbalance created by this procedure, although relatively minor, could potentially have a significant impact in an athletic person.
In most of our patients, the involvement was well below 50% of the diameter of the tendon, and the biomechanical implications of a more major surgical procedure with tendon transfer may seriously jeopardize the patients’ return to athletics and running. However, if the majority of the tendon is involved, tendon augmentation or transfer should be used. These patients have usually already been forced to a lower activity level, being functionally disabled, even with activities of daily living. At the present time, we more commonly perform tendon augmentation using tibialis or semitendinosus tendon allograft rather than tendon transfer.
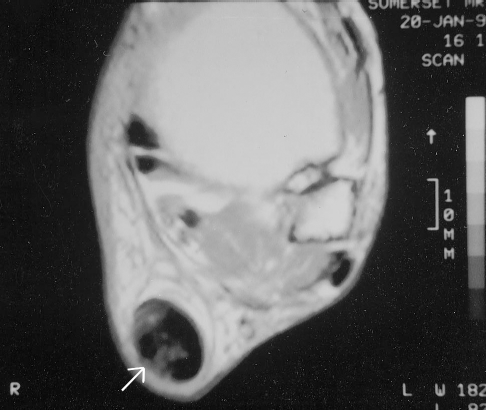
In patients with retrocalcaneal bursitis, the retrocalcaneal bursa should be completely excised. Again, it cannot be overemphasized that exposure is essential from both sides of the tendon, and a second longitudinal lateral incision is necessary. The bursa is usually found to be hyperemic, thickened, and in some cases filled with fibrinous loose bodies and bursal fluid. In most patients, the bursa was found to be scarred and adherent to the anterior surface of the Achilles tendon (Fig. 7). After excision of the retrocalcaneal bursa, the posterior superior angle of the os calcis should be generously excised using a 0.5-inch flat osteotome. The ostectomy should be started just superior to the insertion of the Achilles tendon fibers on the os calcis and performed in approximately a 40° to 50° angle to the long axis of the tendon, up to the posterior-superior surface of the os calcis (Fig. 8). It is critical to expose the area between the anterior surface of the tendon and the posterior os calcis as distally as possible. Since the Achilles tendon has an extensive insertion all the way down to the inferior aspect of the calcaneus, this does not jeopardize the Achilles tendon insertion. Most failures of this procedure are related to an inadequate ostectomy. 106

Chronic retrocalcaneal bursitis. The bursa is markedly thickened and adherent to the tendon.
Ostectomy for retrocalcaneal bursitis. A wide, thin osteotome is used to perform a generous ostectomy of the posterior superior angle of the calcaneus starting right at the insertion and angled at approximately 45°.
The edges should be carefully smoothed to remove any sharp ridges and the ankle should be brought through a complete range of motion to ensure that there is no longer any impingement of the os calcis on the anterior surface of the Achilles tendon. Enough bone should be removed so that there is clearance the size of one finger between the posterior aspect of the os calcis and the anterior aspect of the Achilles tendon with dorsiflexion of the foot. Some authors have described the use of a lateral incision only, as the primary prominence of the posterior superior os calcis is located laterally.89,90 Although some authors, such as Keck and Kelly, 52 have described simple excision of the retrocalcaneal bursa without ostectomy in patients without a bone prominence, most authors, including us, advocate a generous ostectomy in all cases of retrocalcaneal bursitis. A ridge of bone is often left at the distal insertion site that must be carefully removed with a rongeur, curette, and rasp so that no irritating prominence remains above the distal insertion. Most cases of failure referred to us were secondary to an inadequate ostectomy, often performed through a single incision.
In cases of Haglund's deformity, the ostectomy should be more generous on the lateral than on the medial side, and the primary incision should be lateral. In addition, the superficial adventitial bursa needs to be removed as well, taking care not to devascularize the skin flap. This pump bump condition is not frequently seen in athletes and usually can be treated conservatively. Hockey players are the one group of athletic patients in which we have most frequently found this condition. The rigid heel counter of the skate is the causative factor.
Insertional tendinitis is usually seen in older athletes. We tend to treat these patients conservatively for a longer period, even resorting to a period of immobilization in a short-leg walking cast, and, in most cases, symptoms will resolve. Often, a “fish hook” osteophyte is seen with or without ossification of the distal Achilles tendon. In some cases, this osteophyte may actually fracture and cause pain. Again, it is important to be certain that this is actually contributing to the pain, as it is often seen as an incidental radiographic finding. Local inflammation secondary to this osteophyte also occurs in conjunction with degeneration and erosion of the central portion of the Achilles tendon in this area, which contributes to the pain as well. If surgery is necessary, the soft tissues must be handled very carefully, particularly in an older population. Although Baxter and Thigpen 12 recommended a central longitudinal incision, most authors, including us, prefer a longitudinal incision either placed medially or laterally, or in some cases, in both positions. A small splitting incision is made within the tendon at the insertion and any spurs and areas of degeneration are debrided (Fig. 9). Involvement of the retrocalcaneal bursa and some prominence of the posterior os calcis is common in these patients, and these entities should be addressed as well. Complete detachment of the tendon, debridement, and reattachment should be avoided. Again, excessive suture material in closing the splitting incision within the tendon should also be avoided.
Insertional tendinitis with loose osteophyte exposed through a midline longitudinal splitting incision at the insertion.
Postoperative Regimen
In cases of paratenonitis only, range of motion exercises are instituted immediately to prevent scarring and fibrosis. A removable boot walker is used, but the patient is allowed to remove the boot for gentle range of motion exercises. Weightbearing is usually limited for the first 2 to 3 weeks to control soft tissue swelling and to aid wound healing. In those cases where there is a small area of tendinosis, a boot walker will be used for approximately 4 to 6 weeks and range of motion is begun after good wound healing is present. Weightbearing is also limited for the first 4 to 6 weeks. Where there is an extensive area of tendinosis requiring augmentation or tendon transfer, patients are treated with a complete rupture regimen. Patients are initially placed in a short-leg cast in a relaxed plantar flexed position and serial casting is performed at weekly intervals for the first 3 to 4 weeks postoperatively to bring the patients up to a neutral position. They are then placed in a boot walker, at which time range of motion exercises are begun, avoiding aggressive dorsiflexion for the first 8 weeks postoperatively. In cases of retrocalcaneal bursitis, range of motion can be begun immediately and a boot walker is used for 2 weeks with protected weightbearing, and then weightbearing is resumed with the walker being replaced with a heel lift. Patients with insertional tendinitis tend to be older, and wound healing is a major concern. Therefore, we recommend placing patients in a boot walker for 4 to 6 weeks and keeping them nonweightbearing during this time. When good wound healing is evident after the first 2 weeks, range of motion exercises are begun.
Early emphasis in the postoperative treatment regimen should be on regaining passive dorsiflexion. This is achieved with passive stretching, both in the nonweightbearing and weightbearing positions with the knee extended as well as flexed. A graduated program of swimming and stationary bicycling, along with isometric, isotonic, and eccentric strengthening in the later stages is prescribed. Light jogging is usually permitted between 2 and 3 months postoperatively, unless there was extensive tendon involvement, in which case we discourage any running until at least 4 to 5 months postoperatively. Initially, a softer running surface such as a track is recommended. Mileage is gradually increased, and the patient is initially discouraged from doing hill workouts or interval training. Return to a competitive level usually is not until 5 to 6 months postoperatively, and may be longer in cases of extensive tendon involvement.
Alfredson et al. 2 performed a prospective study of 13 patients with chronic Achilles tendinitis who underwent surgical treatment. The authors were interested in return of calf muscle strength. They concluded that 6 months of postoperative rehabilitation for chronic Achilles tendinitis was not enough for patients to recover concentric and eccentric plantar flexion muscle strength compared with the noninjured side. However, in their series, the patients were immobilized in a cast for 6 weeks postoperatively. In a further study, the same authors 3 prospectively looked at the calf muscle strength in patients who were immobilized in a cast for only 2 weeks, followed by an aggressive rehabilitation program. Again, they found that the concentric strength as well as the eccentric strength return is very slow, taking up to 1 year, and even at that point there was still concentric strength deficit. We counsel patients, particularly if they have extensive tendon involvement, that any running activities may not be possible for 6 months, and complete recovery may take up to 1 year.
Results
In our initial surgical series 105 we reviewed 45 surgical cases in 37 patients. Overall, there were 87% satisfactory results. Interestingly, 92% of the patients with involvement of the paratenon or tendon, or both, had a satisfactory outcome, as compared with only 71% of patients with retrocalcaneal bursitis. In this early study, it was apparent that many of these patients had had an inadequate ostectomy. In our subsequent study, looking at 79 cases in 66 patients, 80% of whom were competitive or serious recreational runners, overall there were 79% satisfactory and 21% unsatisfactory results. 106 The percentage of satisfactory results in the paratenonitis group was best (87%), and the percentage in the tendinosis group was the worst (67%). Satisfactory results were found in 75% of patients with retrocalcaneal bursitis and in 86% of patients with insertional tendinitis. Furthermore, in 7 of the 45 cases (16%) with longer than 5-year follow-up and initially satisfactory results, patients’ results deteriorated with time and reoperation was required. This scenario was most commonly seen in the older male runner with tendinosis who, despite adequate debridement at the time of the initial operation and a period of symptomatic relief, had slow recurrence of the degenerative process within the tendon and the development of symptomatic tendinosis. We were able to obtain 2-year follow-up in five of the seven cases after revision surgery, with only three of the five patients able to return to long-distance running.
In a larger series, Nelen et al. 91 treated 170 patients surgically and had follow-up on 143 tendons in 91 patients, only in those patients with paratenonitis or tendinosis, or both. In 50 patients with tendon involvement, they resected the diseased tendon only with a side-to-side repair of the tendon. In the other 24 cases of tendinosis, reinforcement was performed with a turn-down flap. They reported a satisfactory surgical outcome in 82 of 92 cases (89%) of paratenonitis. A satisfactory outcome was obtained in 19 of 26 patients (73%) with debridement and side-to-side repair, and in 21 of 24 cases (87%) with a turn-down flap in cases where there was extensive debridement. Johnston et al. 46 reported on 17 patients who underwent surgery, all of whom were able to return to unrestricted activity after an average of 31 weeks of rehabilitation. Maffulli et al. 75 reported on the surgical outcome of 14 athletes with central degeneration and tendinosis who underwent surgery. Only 5 of these patients (36%) had an excellent or good result, despite reexploration in 6 of the 14 patients. The average duration of symptoms, however, from onset of symptoms to surgery was 87 months. It was their conclusion that surgery in this condition should be performed at an earlier stage. It is our policy that, if symptoms have been recalcitrant to conservative measures for at least 6 months and there is actual tendon involvement, and if the patient is a surgical candidate, surgery should be performed at that time. It is well known that any intrinsic tendon healing that occurs after tendon injury will be relatively complete by 6 months.
Complications include skin necrosis, infection, extensive fibrosis in and about the tendon, and permanent loss of motion or strength, or both. Complications can be avoided by meticulous handling of the soft tissues, avoiding extensive use of suture material in or about the tendon, performing an adequate ostectomy in cases of retrocalcaneal bursitis, and instituting range of motion exercise at an early stage of rehabilitation. Rolf and Movin 103 reported a complication rate of 13% in 58 patients treated surgically. These included two superficial and two deep infections, two deep vein thromboses of the lower leg, one total rupture and one hypertrophic scar. Although a satisfactory surgical outcome can be achieved in most cases, patients with extensive tendinosis, particularly older male runners, should be warned of the high rate of recurrence as well as a possibility that they may not return to a strenuous running program. In most cases, however, surgery does offer a solution in well-selected cases. 64
Achilles Tendon Ruptures
Diagnosis
Since Ambrose Pare 98 first described Achilles tendon rupture in 1575, there is evidence that the incidence of Achilles tendon rupture is increasing in western society.48,67,82 This may be associated with an increase in athletic participation in a predominantly sedentary, white collar population. Leppilahti et al. 67 suggest that the incidence may have increased from 2 in 100,000 in 1986 to 12 in 100,000 in 1994.
Typically, Achilles tendon rupture occurs most commonly in men in their 4th and 5th decades, with an average age of between 30 and 40 in many studies; such ruptures account for 40% of all operated tendon ruptures.21,22,41,43,48,53 Rupture in association with racquet or ball sports or other athletic activity has been noted in 75% to 80% of cases.16,21,33,48,67,82,93,111,112 Möller et al. 82 have commented that the age distribution is bimodal, with a maximum incidence of sports injuries in the 4th decade of life followed by a second but lower peak of other injuries in the 8th decade. Achilles tendon ruptures are less commonly seen in women. The male-to-female ratio has been reported by most authors in the range of 5:1 to 6:1.13,16,21,43,44,53,67,81 Additional risk factors for rupture include prodromal symptoms seen in 15% to 20% of patients with ruptures, 110 a history of previous corticosteroid injection, 76 gout, 13 and treatment with flouroquinolone antibiotics.81,84,85 Several authors have noted a greater incidence of left-sided ruptures and an association with type O blood group.21,41,48,67 In a recent study, an association between high longitudinal arches with less pronation of the ankle and less varus of the forefoot was noted. 66 The authors hypothesized that an underpronating foot and ankle, which are linked with poor shock absorption, increases stress on the Achilles tendon, placing a torsional force on the tendon in midstance and push-off that may cause an ischemic “wringing out” at or near the avascular zone.
The mechanism leading to rupture is not fully understood; however, the interplay of intrinsic pathologic changes within the tendon and extrinsic factors combine to result in acute musculotendinous injury. Intrinsic factors include pathologic degenerative changes in the region of the rupture as found in more than 50% of 292 patients in the study of Jósza et al. 48 ; corresponding rupture typically occurs in the hypovascular region of the tendon 4 to 6 cm proximal to its insertion. Recurrent microtrauma to this region with subsequent inability to heal has been proposed as the cause. Against this are the relative paucity of prodromal symptoms, suggesting a silent degenerative process, and conflicting histologic data, failing to show an association between degenerative change and rupture. 43 Corticosteroids, oral or injectable, have been implicated in collagen necrosis, and flouroquinolone antibiotics have been suggested to be toxic to tenocytes and to inhibit matrix formation.76,81,85
The role of extrinsic factors in Achilles tendon rupture is also significant. Acceleration/deceleration mechanisms have been noted in up to 90% of sports-related injuries. 110 Inglis et al. 43 proposed a malfunction of the normal protective inhibitory neuromuscular pathway of the musculotendinous unit in the fatigued or poorly trained athlete, a theory that is supported by data suggesting that rupture typically occurs 30 minutes or more into the athletic endeavor. Biomechanical factors may also contribute, as noted by Åström and Rausing 10 and Leppilahti et al. 66 Clearly, the cause is multifactorial, with a complex interplay of contributing factors.
The clinical history of Achilles tendon rupture is frequently typical, with the athlete describing an audible snap and sudden pain, as if being kicked or hit from behind. Many clinical tests have been described to detect acute rupture.74,94,108,117 A recent study attempted to validate several of these tests and found that the calf squeeze test described by Thompson 117 and Simmonds 108 was the most reliable, with a 93% sensitivity. 73 The palpable gap test was the least sensitive, with a value of 73% with the patient awake, improving to 81% under anesthesia. All tests had a high negative predictive value, and we have found a combination of these two tests to be highly reliable. Imaging is generally not indicated except when tendinous avulsion is suspected, which, in our experience, is uncommon. Magnetic resonance imaging and ultrasound are sensitive and specific; however, they do not influence surgical planning in acute cases and, in our opinion, are not warranted except perhaps in the rare case when clinical findings are equivocal. Perhaps somewhat surprisingly, a reported 20% of ruptures are missed by primary treating physicians. 43
Treatment Options
There has been much debate over the relative merits of operative versus nonoperative management of acute Achilles tendon ruptures. A lack of defined universally accepted outcome measures, a multitude of different reparative techniques, and a similarly diverse range of postoperative immobilization and rehabilitation protocols have made comparison of results difficult.
In the early 20th century, closed treatment was widely accepted as the standard of care; however, the increasing functional demands of the athletic population and improved surgical technique have caused operative treatment to gain popularity in recent times. Patient selection remains the most important factor decision. Operative treatment, particularly with early functional rehabilitation, seems to confer better functional outcome with accurate restoration of tendon length and a lower rerupture rate.13,16,21,32,44,124 Against this are the reported complication rates associated with open treatment and the acceptable functional results of closed treatment in the less-demanding athletic population.21,37,43,65
Nistor, 93 in a randomized prospective trial of 105 patients, noted 2 deep infections and 2 reruptures complicating operative treatment versus 5 reruptures in the closed treatment group. After evaluation of subjective and objective plantar flexion strength and power using functional tests and a dynamometer, the author concluded that operative surgical treatment conferred no great advantages and that closed treatment was therefore preferable. Of note, only nine patients in this series participated in competitive sports.
Beskin et al. 13 evaluated 42 patients who underwent primary repair using a number of techniques including direct repair, plantaris tendon augmentation, and peroneus tendon augmentation. No reruptures were noted, with a 7% minor wound complication rate. Better results were noted in the three-bundle technique, but rehabilitation was not uniform and, in the latter group, consisted of early functional treatment.
Augmented repair has also been described. This may be performed with local tissue, such as a fascial turn-down from the proximal tendon, plantaris muscle, peroneus brevis muscle, or with synthetic material.32,68,71,116 Fernández-Fairén and Gimeno 32 reviewed the results of repair augmented with a polyethylene terephthalate mesh synthetic graft that permitted immediate mobilization with weightbearing in the 3rd week. Twenty patients were high-level amateur athletes and nine were professional athletes. Average flexion strength was 96% of the normal side, as measured with a dynamometer.
Gerdes et al. 36 studied the efficacy of repair using a fascial turn-down technique. Biomechanical cadaveric studies were performed and strength was compared with two interrupted Kessler sutures, revealing a 35% increase in strength to failure. In a small series of seven patients, immediate postoperative weightbearing was allowed in a cast for 6 weeks. Five patients had excellent results at 1 year and one had a good result; all athletes returned to their previous levels of activity. Plantar flexion strength measured 94% of the contralateral limb.
Cetti et al. 21 reviewed 111 patients in a nonrandomized prospective study in 1993. There were 10 major complications (9%; 4% with deep infection) in the operatively treated group and 18 (16%) (8 were reruptures) in the nonoperative group. Repair was performed with an end-to-end Bunnell suture, and cast immobilization with nonweightbearing was implemented postoperatively. Although hospitalization was longer in the operative group, return to work was 2 weeks earlier. Perhaps more importantly, 63 patients (57%) returned to sports at the same level, versus 32 (29%) in the nonoperative group. The authors also reviewed the literature on 4083 Achilles tendon ruptures treated operatively and noted a difference in rerupture rate after operative and nonoperative treatment (1.4% to 13.4%) and also a lower overall rate of complications (3.5% to 18.1%). Simple end-to-end repair without flaps or augmentation had a trend toward a lower rerupture rate (0.65%) and decreased wound complications. Various methods have been used to objectively evaluate functional recovery, and in those studies in which a dynamometer was used, mean plantar flexion strength after surgery was 87%, versus 78% with nonoperative treatment. Similarly, return to sports at preinjury levels was 62% versus 51%.
Inglis et al. 43 studied 79 patients, 48 of whom were treated operatively and 31 nonoperatively. Complications in the former group included two superficial infections, no reruptures, and only two dissatisfied patients. This contrasts with the results in the nonoperative group where, although immobilization ranged from 5 to 9 weeks in short- and long-leg casts, there were 9 reruptures and only 9 of 23 patients were satisfied. Strength/power/endurance measured objectively were 101/88/91 versus 73/62/64, all significantly less in the nonoperative group. Furthermore, in 17 cases that were operated later in the study, endurance was 20% less. The authors noted that their complication rate had decreased with surgeon experience, and in 1981 they reported on a series of 159 patients with a complication rate of 12.5%. 44 Kellam et al. 53 reported a rerupture rate of 3% and an incisional complication rate of 13%, with 92% of the patients returning to previous levels of participation. Wills et al. 124 reviewed complications in the literature and noted a trend toward a decreasing operative wound complication rate with time. Arner and Lindholm, 8 in their 1959 series, reported a 30% complication rate, whereas in a recent study of repair using several techniques in 101 patients, of whom 91 were athletes, a complication rate of 6.9% was noted. The authors also described a standardized scoring protocol for evaluation of outcome.
Percutaneous repair was first described by Ma and Griffith 72 in 1977 in an attempt to avoid the potential wound complications of open repair while obtaining the advantages of operative apposition of the tendon ends and restoration of tendon length. FitzGibbons et al. 33 reported on the follow-up of 14 patients after percutaneous repair, noting two sural nerve injuries and no other significant complications; however, a 13% loss of power was seen on isokinetic testing at 180 deg/sec. Subjectively, satisfactory results were noted in recreational athletes, with all of them returning to preinjury activity levels.
Bradley and Tibone 16 reported on a series of 12 percutaneous repairs and compared these with a series of 15 patients treated with an open technique using a gastrocnemius muscle flap as described by Lindholm. 68 Two reruptures (13%) occurred in the percutaneous group, but otherwise no differences were noted in subjective or objective outcome as measured isokinetically. No complications were noted and the authors concluded that percutaneous repair should be reserved for the recreational athlete. Ma and Griffith, 72 in their original series of 18 patients, had no wound complications, but they reported a rerupture rate of 12%; plantar flexion power, assessed objectively, ranged from 72% to 94% of the contralateral limb. Hockenbury and Johns 42 suggested that percutaneous repair may not be strong enough to allow an aggressive rehabilitation program. In a cadaveric study, they performed biomechanical studies on five specimens with a percutaneous technique and compared the results with those after a direct end-to-end Bunnell suture technique. They found a 60% incidence of sural nerve entrapment and 50% relative strength in the percutaneous group. In our opinion, the difficulty in accurately restoring musculotendinous length by closed means does not significantly outweigh the reduced incidence of wound necrosis and potential sural nerve injury in the athletic population. In a further attempt to avoid the reported 25% wound complication rate associated with open repair, Esemenli et al. 31 described a combined open and percutaneous technique using a modification of the fascial turn-down technique, avoiding an open incision directly over the site of repair. The follow-up was 2 years, but there were only three cases with no reported reruptures.
The biomechanical strength of several repair techniques has been evaluated in cadaveric models. 123 In an analysis comparing Bunnell suture with modified Kessler and interlocking suture, investigators found the interlocking suture to be significantly stronger. 42 In a further biomechanical evaluation of the percutaneous technique, the authors demonstrated significant gapping at the repair site in addition to a high rate of sural nerve entrapment and concluded that percutaneous repair did not provide sufficient initial strength to allow aggressive rehabilitation. Mortensen and Saether 83 compared a continuous six-strand suture technique with the Mason and Bunnell techniques and found significantly greater tensile strength and gapping resistance. Our concerns with the more complex suture techniques previously described, as well as the three-bundle technique described by Beskin et al., 13 is the bulkiness of these repairs, with higher wound complication rates noted in some clinical series and the potential for devascularization of the tendon with multiple complex grasping sutures.
We believe that surgical repair is indicated in the athletic population primarily to restore functional length of the musculotendinous unit. Closed and percutaneous methods are not incompatible with this dictum; however, achievement of these ends without open means is far less predictable. For this reason, we advocate repair using a simple modified Kessler suture with No. 5 nonabsorbable and a running epitendinous 2.0 absorbable suture, avoiding any knot placement or bulky suture material directly beneath the incision. We prefer a medial incision with the patient prone and we routinely use a tourniquet. The contralateral limb is free-draped to allow a comparison of resting tension with the normal limb. Careful handling of soft tissues is mandatory for success, and we attempt to close the paratenon over the repair after release of the tourniquet. Appropriate intraoperative tensioning of the repair is essential and is performed with the knee flexed to 90°. In this position, the gently plantar flexed foot should return to neutral after release. A comparison with tension on the contralateral side is always helpful.
Various augmentation techniques have been described, including local gastrocnemius muscle fascial augmentation as described by Lindholm, 68 peroneus brevis muscle transfer as described by Teuffer, 116 and plantaris muscle augmentation as described by Lynn. 71 In addition, reconstructive techniques using flexor digitorum longus and flexor hallucis longus muscles have been described.79,121,122 Although these may offer a biomechanical advantage in terms of permitting a more aggressive rehabilitation program, we do not believe that they are required in acute cases if an adequate primary repair can be obtained without the potential for greater wound complications, as noted by Cetti et al., 21 and potential donor site morbidity.
Before the 20th century, treatment of Achilles tendon rupture was primarily nonoperative; however, with the work of Arner and Lindholm, 8 surgery became increasingly popular. However, the significant complication rate associated with operative treatment in the 1960s and 1970s led Lea and Smith 60 to review 56 patients treated nonoperatively with casting. They recommend this treatment for all patients with acute rupture, citing experimental evidence of tendon regeneration when sectioned. The authors also argued that rerupture could be avoided by casting for 8 weeks rather than 6 weeks. Fourteen patients had greater than 6° of increased dorsiflexion and none were professional or college athletes. No consensus exists concerning the duration of cast treatment, weightbearing, or the length of cast (that is, above the knee versus below the knee), although the cadaveric studies of Davis et al. 30 suggest that short-leg cast immobilization is sufficient.
We recommend closed treatment only for those patients with limited functional goals and also for those patients with concurrent medical conditions that preclude adequate wound healing, such as arteriosclerosis, diabetes, limb edema, or dermatologic problems. In these patients, we prefer immobilization in a short-leg cast with the foot in equinus for 4 weeks, followed by a walking cast or boot walker in neutral plantar flexion, permitting a gradual increase in weightbearing to 8 weeks and then adding a 2.5-cm heel rise to the shoe for the following 4 weeks.
Rehabilitation
The postinjury rehabilitation of Achilles tendon ruptures, whether treated operatively or nonoperatively, remains controversial. Traditionally, treatment has consisted of cast immobilization for a period of 6 to 8 weeks with immobilization of the ankle initially in equinus, with subsequent return of the foot to neutral plantar flexion over the following 3 to 4 weeks. Some authors have advocated treatment in a long-leg cast; however, this is not supported by the biomechanical cadaveric studies of Davis et al., 30 who demonstrated minimal tension in the tendo-Achillis with the ankle in 25° of plantar flexion, irrespective of knee position.
Experimental work in animals has confirmed that the benefits of loading the healing musculotendinous unit are improved vascularity, decreased collagen cross-linkage, and increased size and number of collagen fibrils. In addition, appropriate loading has been shown to improve fiber orientation, with corresponding enhanced biomechanical properties when compared with immobilization.87,111 The detrimental effects of immobilization have been well documented. Häggmark and Eriksson 39 demonstrated gross morphologic wasting and histologic changes in the soleus muscle with atrophy of type 1 fibers in athletes immobilized for 6 weeks. Neumann et al. 92 demonstrated kinematic and neuromuscular alterations in gait 12 months after surgery for tendo-Achillis rupture, with subsequent immobilization for an average of 9 weeks. Other potential complications of immobilization include arthrofibrosis, adhesions, venous thromboembolism, and pressure necrosis from casts or splints.
Given this experimental evidence for the advantages of early mobilization, practitioners have subsequently applied these principles clinically. Clearly, the main concerns with early mobilization are the potential for increasing the incidence of wound complication and early rerupture, which might outweigh any potential long-term benefits. As such, the initial strength of the surgical repair must be sufficient to withstand an aggressive rehabilitation program.
Early reports describing limited range of motion with restricted weightbearing were favorable.22,111,118 More recent protocols have advocated progressively earlier weightbearing in functional orthoses.77,112 Using these regimens, return of objectively measured strength, range of motion, and power have been to within 97% of the contralateral limb at 12 months with return to previous levels of sporting activity. This compares favorably with previous immobilization techniques resulting in, at very best, a 10% strength deficit. No reruptures were noted in the series of Mandelbaum et al. 77 and Speck and Klaue, 112 and there was a single partial rerupture in a noncompliant patient in the series of 13 patients treated surgically by Troop et al., 118 with a postoperative regimen that incorporated early weightbearing in a functional orthosis. Buchgraber and Pässler 18 retrospectively compared 48 patients who underwent either cast immobilization or early functional treatment that included full weightbearing after surgical repair with a percutaneous technique; they found fewer functional deficits, increased range of motion, and no increased rerupture rate in the functionally treated group. In a recent clinical study, Aoki et al. 6 reviewed the results of 22 ruptures in athletes using a Kirschmayer core suture and cross-stitch epitenon suture. Clinical results were assessed with MRI findings, which have been shown to accurately depict tendon healing in this context. 51 Initially, early active motion and partial weightbearing were commenced, with full weightbearing at 16 days and return to sport at an average of 13 weeks. No reruptures were reported. Although no biomechanical testing and no formal strength testing were performed, the authors suggested that the increased strength of this technique might permit a more active and functional early rehabilitation program with early weightbearing.
Our preference is to initially place the affected foot in an equinus position that minimizes tension on the soft tissues. At 5 to 7 days, provided the wound is healing well, we progress with serial casting over the next 3 weeks, gradually bringing the foot up to neutral plantar flexion, maintaining some tension on the repair. At that point, a boot walker with a heel lift, which is gradually decreased in size, is used and progressive weightbearing is allowed. The boot is discontinued at 8 weeks. Light jogging is permitted at 3 months if the patient has regained full dorsiflexion. Full return to running and jumping sports is permitted between 4 and 6 months, assuming adequate strength gains have been made.
Chronic (Neglected) Rupture
Chronic ruptures have traditionally been defined as ruptures in which more than 4 weeks have passed since the initial acute injury. 121 This is not an arbitrary period, but defines the period beyond which significant retraction and shortening of the gastrocnemius-soleus musculotendinous unit occurs. Primary end-to-end repair of the Achilles tendon becomes very difficult to achieve when there is the essential problem of a shortened musculotendinous unit with its deleterious biomechanical effects.15,19,35,121 Chronic rupture may result from a number of causes. First, acute rupture may be missed in 20% to 25% of cases.8,43 Alternatively, the patient may be seen late, although this is an uncommon scenario in the athletic population where a deficit in plantar flexion strength functionally manifests itself early, with symptoms such as inability to perform a heel rise or difficulty climbing stairs. Rerupture after previous closed or surgical treatment manifests the same technical problems with respect to operative treatment as does repeated partial rupture with chronic elongation of the musculotendinous unit. Several authors have reported poor results from nonoperative treatment in active patients with a neglected rupture and with significant functional disability, although it has been widely shown in animal studies that the tendo-Achillis will reconstitute by means of fibroblastic invasion of interposed hematoma.43,88 It is well recognized that nonoperative treatment is unable to restore precisely the optimal functional length of the musculotendinous unit, with subsequent deleterious consequences for the athletic population.
Many operative reconstructive options have been described; however, the basic tenets of reconstruction are restoration of optimal length and reconstruction of the gap with appropriately strong tissue that may be obtained from a number of sources.6,8,14,68,79,116,119 These options are 1) direct repair (rarely possible) 100 ; 2) augmentation with or use of local autogenous tissue such as those used with the various turndown techniques,8,16 proximal V-Y advancement, 1 or plantaris muscle augmentation 71 ; 3) local tendon transfer, including use of peroneus brevis,116,119 flexor hallucis longus, 122 or flexor digitorum longus muscle 79 ; 4) the use of free tissue transfer for reconstruction, including both autograft and allograft; and 5) techniques using synthetic materials such as carbon fiber and Marlex mesh (C. R. Bard, Murray Hill, New Jersey) or Dacron. 95
Determination of the appropriate technique is ultimately made at the time of surgery, when factors such as mobility of the proximal complex and gap size, as well as quality of the local tissue can be fully assessed. Clinical examination and ultrasound or MRI may be helpful in preoperative planning. Myerson 88 has provided a useful algorithm for treatment based on the size of the intraoperative gap. Certainly, techniques that involve the use of local tissue for augmentation are useful for small gaps of only 2 to 5 cm. Our practice is to attempt end-to-end apposition if the gap is small (<1 cm) and proximal mobility permits. We routinely excise the interposed fibrous scar, although there is evidence that this may not be necessary or even helpful. We then augment the repair with local tissue, such as the plantaris muscle, if intact, and weave this through the repair. When this tissue is not available, we have used a single proximal turn-down flap of fascia and, more recently, we have used semitendinosus muscle allograft. For larger defects, of around 5 cm, we prefer the use of proximal V-Y advancement in combination with allograft or autograft (usually semitendinosus muscle) tissue augmentation. Good results have been reported from V-Y advancement, but the flap mobilization must be meticulous. We reserve tendon transfer for the large defects and, although none of the various options are ideal, our preference is for the peroneus transfer originally described by Teuffer 116 and modified by Turco and Spinella. 119 As a second choice, we would favor the use of flexor digitorum longus muscle, as described by Mann et al., 79 because this seems to be less detrimental to plantar flexion power than the transfer of flexor hallucis longus muscle described by Wapner et al., 122 although biomechanically the flexor hallucis longus muscle transfer is perhaps the most appropriate. The use of a posterior compartment fasciotomy to allow direct apposition of the flexor hallucis longus muscle belly to the Achilles tendon is also attractive, and good results have been reported with the use of this technique.121,122 In addition, it functions as a muscle transfer primarily and a tenodesis secondarily.
Synthetic materials, including Marlex and carbon fiber, have also been used for reconstruction of large defects, with mixed results. We have no direct experience with this but are concerned about the potential problems with wound healing, in addition to the long-term durability.
The use of free tendon transfer has a role in reconstruction, and there have been several reports of successful use of autogenous patellar tendon and allograft tendo-Achillis in patients with insertional rupture, often after previous corticosteroid injection, or in those with calcaneal bone loss (for example, a patient who has undergone previous resection of a Haglund's deformity). Circumstances requiring such reconstruction are fortunately exceedingly rare.
Technically, surgical principles identical to those of primary repair apply. Full-thickness flaps should be raised to the paratenon and subsequently these should be handled atraumatically. Appropriate length is judged intraoperatively in the manner described for primary repair. Similarly, we prefer to keep the repair low profile under the wound and avoid placing suture material directly beneath the skin. A higher rate of complications has been noted in this group and, accordingly, we are more conservative in our rehabilitation program, depending on the integrity of the repair. The long-term results are mixed, with reports of return to activity and loss of plantar flexion strength being variably reported as 30% to 50% of contralateral limbs. 122
The Future
The role of growth factors in musculoskeletal repair and regeneration is well recognized. There have been several recent reports on the use of such factors to enhance Achilles tendon healing in animal models. Kurtz et al. 56 studied the effects of insulin-like growth factor on Achilles tendon healing in a rat model and demonstrated an antiinflammatory mechanism as well as a significantly smaller functional deficit and more rapid time to recovery in the insulin-like growth factor-I group. Young et al. 125 looked at the effect of delivering marrow-derived, mesenchymal stem-cell seeded collagen implants to a 1-cm tendon gap model in rabbits. Significantly greater structural and material properties were noted in the treatment group, and the collagen appeared to have a greater cross-sectional area and better alignment than in controls. Aspenberg and Forslund 9 transected Achilles tendons in rats and implanted GDF (growth differentiation factor) 5 and 6 growth and differentiation factors on collagen sponges and compared these with a control group of collagen sponges alone. The rats were sacrificed at 2 weeks and the tensile strength of the regenerated tendon was found to be increased by both proteins in a dose-dependent manner.
Low-energy photostimulation at certain wavelengths can also enhance tissue repair by releasing growth factors from fibroblasts. In an animal model, Reddy et al. 102 found a 26% increase in collagen concentration after daily treatment with a helium-neon laser. Combined with current techniques of surgical repair and optimal functional rehabilitation programs, these innovations offer the real prospect of returning athletes with Achilles tendon injuries to their preinjury levels of sports sooner and with fewer functional deficits.