
Abstract
Background: Several problems have been reported with use of allogenic grafts in anterior cruciate ligament reconstruction, including local immune response to allograft tendon within the synovial fluid, delayed maturation and ligamentization, and progressive tibial tunnel enlargement.
Hypothesis: There is a correlation between the use of allograft and tibial tunnel enlargement.
Study Design: Controlled laboratory study.
Methods: Twenty healthy adult female goats underwent allograft anterior cruciate ligament reconstruction and were followed with serial radiographs at 6-week intervals. Animals were randomly chosen for sacrifice between 18 and 36 weeks for histologic assessment.
Results: Significant radiographic increases in tunnel size were noted within the first 6 weeks of healing and remained up to 36 weeks with no further remodeling noted. Histologic analysis showed progressive ligamentization of the allografts with tendon-to-tunnel wall biologic fixation with dense connective tissue. Remodeling and incorporation of the bone plug was seen in all cases. The allograft tendon underwent early fibrous attachment within the tunnel and remodeled toward ligament histologic structure. Remodeling and incorporation of the bone plug was seen by 18 weeks.
Conclusion: Tibial tunnel enlargement, consistent with that seen in humans after allograft anterior cruciate ligament reconstruction, did not appear to affect the ultimate incorporation of the allograft on a histologic level.
Use of allograft tendon for ACL reconstruction has provided good-to-excellent clinical results,14, 15, 29, 31 particularly when autogenous patellar tendon is not available, as in cases of revision ACL surgery. 38 Use of allografts provides unlimited tissue bulk, avoids surgical trauma to the donor site, and enables more rapid return of strength with less incidence of anterior knee pain. 13 Widespread use of allograft tissue is not common despite major advances in tissue bank screening for transmittable diseases. There are still questions regarding the biologic incorporation, remodeling, and ultimate strength of allograft tissue. Several potential problems with regard to use of allogenic grafts have been reported, including local immune response to allograft tendon within the synovial fluid,2, 34, 36 delayed maturation and ligamentization,4, 5, 7, 8, 17, 23, 34, 36 and progressive tibial tunnel enlargement.6, 11
Previous animal and clinical studies of allograft tendon have failed to evaluate the fate of the tissue within the tibial tunnel, concentrating primarily on the intraarticular portion of the graft and on graft strength.1, 4, 5, 8, 14, 16, 17, 23, 29, 30, 34, 39 Clinical outcome studies comparing allograft tendon with autograft tendon have produced conflicting results.20, 28, 35, 37 Radiographic and functional outcome scores are typically equivalent for both allograft and autograft ACL reconstructions.20, 28, 35 However, one study noted that ACL allograft laxity may increase with time. 39
The current study was designed to evaluate the histologic progression of allograft tissue incorporation into a tibial tunnel and to determine whether there is a correlation between allograft use and radiographic tunnel enlargement. Tibial tunnel diameter was radiographically documented in a goat model, and ACL remodeling was histologically assessed up to 36 weeks postoperatively. The goal was to understand the mechanism of tunnel enlargement occasionally seen clinically with use of allogenic tissue.
Materials and Methods
Allograft ACL reconstruction was performed in 20 healthy, skeletally mature female goats. Goats were sacrificed at 18 (N = 8), 24 (N = 7), 30 (N = 3), and 36 (N = 2) weeks postoperatively for histologic analyses. Radiographs of all surviving goats were obtained at 0, 6, 12, 18, 24, 30, and 36 weeks for quantification of tibial bone tunnel diameter.
Surgical Technique
All surgical procedures were approved by the Institutional Animal Care and Use Committee at the University of Florida. Donor bone-patellar tendon-bone allografts were aseptically harvested from healthy goats approximately 1 to 3 months before reimplantation and stored at -70°C. The allografts were slowly thawed at room temperature in normal saline solution for reimplantation. The grafts were prepared to include a 10- to 15-mm long trapezoidal tibial bone plug and a tapered trapezoidal patellar bone plug to fit within the 6-mm tibial and femoral tunnels of the recipient goat.
Animals were anesthetized before surgery with intravenous 2% thiopental sodium at a dose of 20 to 25 mg/kg. Before endotracheal intubation, atropine (0.2 mg/kg) was administered intravenously. Anesthesia was maintained by inhalation of 2.0% to 2.5% halothane and 97.5% to 98% oxygen. The right limb was prepared with povidone-iodine antiseptic and sterilely draped. A lateral parapatellar arthrotomy was made to expose the intercondylar notch. The ACL was excised and notchplasty was performed. Guide pins were placed centrally in the ACL attachment sites and were overreamed with a 6-mm diameter cannulated reamer. The tunnel edges were chamfered and the allograft was passed in an antegrade fashion with the patellar bone plug press-fitted into the femoral tunnel. The tibial bone plug was secured in the tibial tunnel by using doubled No. 2 Ethibond suture (Ethicon, Somerville, New Jersey) passed through drill holes in the bone plug and tied over a 3.5-mm cortical screw and washer. Range of motion, graft tension, and the anterior drawer test were checked intraoperatively to assess the adequacy of the reconstruction. Intraoperative bacterial cultures were obtained, and the soft tissues were closed in layers. Postoperatively, the goats received analgesics (0.005 to 0.01 mg/kg buprenorphine hydrochloride) for pain, as needed, and were housed in individual pens. The operated limb was maintained in lateral splints, and the animals were allowed activity as tolerated until suture removal at 2 weeks and then released to pasture with unrestricted activity.
Anteroposterior and lateral radiographs of the anesthetized animals were obtained immediately after the surgical procedure (time 0) to document bone tunnel size and placement. Radiographs were repeated on sedated animals at 6-week intervals until they were sacrificed. Standardization of the radiographic technique was performed to minimize differences in magnification and to allow accurate measurement of the tibial tunnel diameters. Measurements of tunnel width were taken by a single investigator (NLH) on the AP radiographs at the subchondral plate and epiphyseal scar.
Analysis of variance with repeated measures was used to assess the effects of healing time on the radiographically determined tunnel diameter. The level of significance was set at α = 0.05, with a statistical power of greater than 70% for 0 through 24 weeks. Statistical power for assessments at 30 and 36 weeks was less than 30% because of the low sample size.
Animals were sacrificed by an overdose of pentobarbital sodium (60 mg/kg), and the operated stifle joint was harvested for histologic assessment. Eight animals were sacrificed at 18 weeks, seven at 24 weeks, three at 30 weeks, and two at 36 weeks. The tibiae were disarticulated, stripped of soft tissue, and placed in 70% alcohol for fixation and storage. Specimens were decalcified in 5% formic acid and embedded in methyl methacrylate by standard methods. 25 Thin 8-μm thick sections were cut with a Jung Polycut E microtome (Leica, Wetzlar, Germany). All sections were stained with hematoxylin and eosin for qualitative assessment of cellular response to the allograft and microscopic evaluation of the graft-tunnel interface.
Results
Radiographs of all goats were obtained every 6 weeks until sacrifice. Twenty animals had radiographs up to 18 weeks, 12 animals until 24 weeks, 5 animals until 30 weeks, and 2 animals until 36 weeks. Two goats developed medial dislocation of the patella; one required reoperation and soft tissue realignment of the extensor mechanism. There were no postoperative infections.
Radiographic Analysis
Tunnel margins were best delineated on the AP radiographic view, and this view was used for all tunnel measurements. The mean tibial tunnel diameter for all 20 goats significantly increased between the immediate postoperative period and 6 weeks after surgery for both the subchondral plate (P = 0.0001) and the epiphyseal scar (P = 0.001) analysis sites, with enlargements of 0.82 mm and 0.92 mm, respectively. No further enlargements were noted radiographically after 6 weeks. Figure 1 graphically presents the mean tibial tunnel measurements with 95% confidence intervals at the subchondral (Fig. 1A) and epiphyseal (Fig. 1B) regions throughout the 36-week period. As noted in Figure 1, tunnel diameter measurements at all time points were significantly larger than the measurement at time zero for the epiphyseal region and at all time points except 36 weeks for the subchondral region. No significant changes in tunnel diameter after 6 weeks were noted at either measurement position (P > 0.05).

Graphic representation of the radiographic measurements of tibial bone tunnel diameter over time in vivo. Measurements are subdivided into the subchondral region (A) and the epiphyseal region (B). The solid line represents the mean measurement and the dashed lines represent standard deviations. The time points of weeks postoperative indicated by a triangle are significantly different from time zero (P < 0.05).
No significant degenerative changes were noted radiographically except in the two animals that sustained medial dislocation of the patella and were observed to have degenerative changes of the patellofemoral joint. The bone plug within the tibial tunnel was difficult to delineate radiographically by the 12th postoperative week, indicating osteointegration of the allograft plug to the surrounding host bone (Fig. 2).
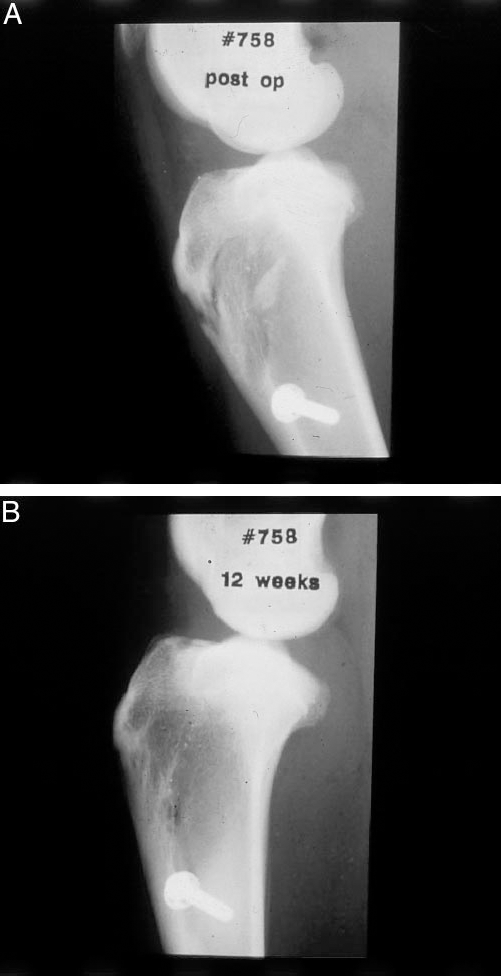
Radiographs obtained immediately after surgery (A) and at 12 weeks after surgery (B). The bone plug is clearly delineated immediately after surgery, whereas the edges of the bone plug fade within the bone tunnel by 12 weeks, indicating either resorption or osteointegration.
Gross Specimen Examination
At necropsy all stifle joints were stable to an anterior drawer force with no significant limitations in passive range of motion. There was no clinical evidence of infection, effusions, or wound healing problems. There was moderate fibrosis of the fat pad, yet no evidence of tibiofemoral arthrosis or meniscal tears. Grafts were covered with a synovial-like tissue and were intact. All grafts appeared to have maintained appropriate intrajoint tension.
Histologic Examination
Histologic evaluation of the tibial tunnel for the goats sacrificed after 18 weeks of healing showed all grafts to be revascularized and repopulated with viable cells, particularly at the periphery. Cells remained sparse in some central areas. Normal longitudinal collagen alignment was noted. A dense, cellular connective tissue interface existed between the graft and the bony tunnel wall (Fig. 3). The tunnel wall showed active remodeling, with areas of osteoclastic resorption and areas of new bone formation. A single specimen in the 18-week group exhibited inflammatory cell infiltrate within the connective tissue bundles of the graft in the tibial tunnel (Fig. 4). These inflammatory cells consisted primarily of plasma cells and macrophages consistent with an immunologic response to the allograft tissue. This inflammatory response may have indicated a transitory reactive state because the graft was healing normally in all other respects. By the 36th week, healing, remodeling, integration, and maturation of the allograft tendon was evident, with grafts intimately associated with the bone tunnel wall through dense connective tissue (Fig. 5).
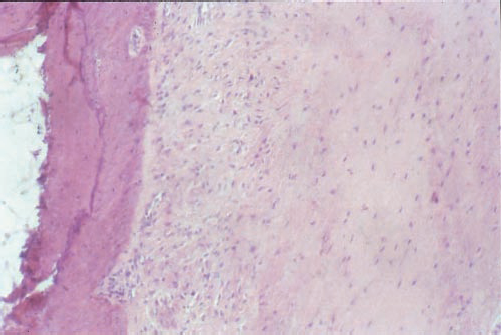
Photomicrograph obtained 18 weeks after surgery showing repopulation of the graft with host cells and signs of revascularization. Formation of fibrous tissue between the tunnel wall and the graft indicate healing and mechanical interlock. (Hematoxylin and eosin; original magnification, X100)
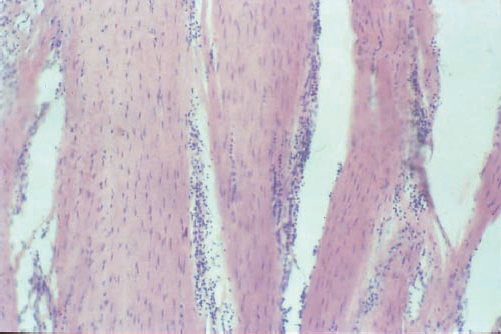
Photomicrograph obtained 18 weeks after surgery showing an inflammatory response indicated by infiltration of lymphocytes and macrophages. (Hematoxylin and eosin; original magnification, X100)
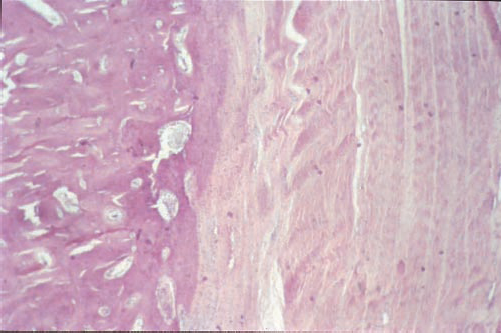
Photomicrograph obtained 36 weeks after surgery showing maturation and ligamentization of the graft tendon. A dense connective tissue association is noted between the graft and the bone tunnel. (Hematoxylin and eosin; original magnification, X100)
Histologic changes around the bone plug were consistent with the radiographic images of progressive bone resorption, remodeling, and osteointegration. Bone resorption seemed to depend on the location of the bone plug within the proximal tibia. The bone plugs located within the fatty medullary canal distal to cancellous metaphyseal bone experienced extensive resorption by 24 weeks, with residual fibrous tissue visible in the area around the fixation sutures (Fig. 6A). When the graft was located more distally, adjacent to the cortical bone of the distal-most tunnel, the bone plug integrated into the host bone with loss of distinct graft-host margins seen macroscopically (Fig. 6B). Areas around the suture holes, when identified, were surrounded with fibrous tissue. No significant inflammation was seen at the site of the bone plug, with the exception of the animal that had a presumed rejection response.
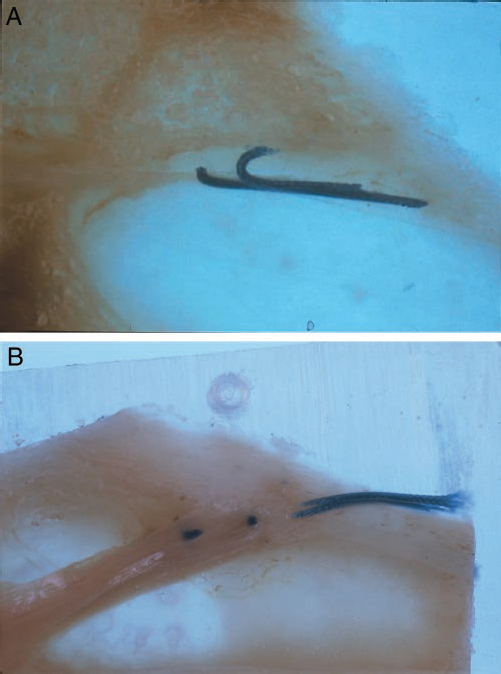
Macrosection cut through the bone tunnel in the coronal plane of two animals at 24 weeks after surgery. The location of the bone plug is identified by suture remnants. A, the location of the bone plug was adjacent to the marrow space, showing resorption of the plug with in-fill of fibrous tissue. B, the location of the bone plug was adjacent to the tibial cortex, showing osteointegration of the plug with the host bone. The joint line is on the left side of each illustration. (Magnification, x1)
Discussion
Reconstruction of the ACL has evolved over recent years to become an accepted, reliable procedure for restoration of functional knee stability. Arthroscopically assisted bone-patellar tendon-bone autograft reconstruction is widely accepted and may be considered the standard of treatment. Autologous ACL bone-patellar tendon-bone grafts have proved to have sufficient strength because of bone-to-bone healing within the tunnel and because of interference screw fixation. 24 Harvesting of autogenous patellar tendon grafts is not without potential risks, including patella fracture, patellar tendon rupture, harvest site tenderness, anterior knee pain, and patella baja.6, 27 In addition, autogenous patellar tendon use may be contraindicated in patients with previous patellar tendon injury, patellar malalignment, patella baja, or previous revision ACL procedures. These considerations have led to the use of allograft tissue for ACL reconstruction.
Allograft tissue offers the advantages of selection of unlimited graft widths, decreased surgical trauma and morbidity, rapid rehabilitation, and decreased incidence of anterior knee pain. 13 Of concern, however, is the unanswered question of the biologic behavior and long-term function of allograft tissue. 33 Good-to-excellent results have been obtained by using allografts in animal models and clinically in humans.1, 5, 14–16, 23, 29–31, 39 Allografts appear to proceed through a revascularization phase similar to that of autografts,1, 16, 23, 30 with repopulation of the graft by host cells. 18 Concern over disease transmission has declined with improved screening techniques used in tissue banking.3, 6 Immune response to allograft tissue is minimal in both animals and humans.1, 5, 14–16, 23, 29–31, 39 The major histocompatability antigens, thought to exist predominantly in the cellular component of the graft, are rendered inactive by the freezing process used to store allograft tissue.16, 22, 23 Decreased biologic activity of the healing graft34, 36 and delay in maturation of allograft tissue when compared with autografts has been reported.4, 5, 7, 8, 17, 22 Our study did identify one animal with a local immune response, yet this animal did not appear to have impaired healing or biologic activity at the graft site. The clinical significance of these findings is unclear.
Recent reports of long-term follow-up of ACL-deficient knees reconstructed with allograft have demonstrated progressive enlargement of the tibial tunnel.7, 21 In a retrospective review, Fahey and Indelicato 7 measured the tunnel diameter of patients whose knees were reconstructed with fresh-frozen allograft compared with those reconstructed with bone-patellar tendon-bone autograft. The tibial tunnel in the allograft reconstructions enlarged an average of 1.2 mm during the 1st postoperative year, which was significantly more than the enlargement seen in those patients whose knees were reconstructed using autograft (P = 0.0002). The authors also indicated that there was no difference in the laxity of the patients’ knees or in the clinical outcome based on graft type. Subjective qualitative laxity assessment and radiographic measurements of tunnel diameters in our current goat study with bone-patellar tendon-bone allograft parallel the results of Fahey and Indelicato 7 and of Linn et al. 21 Although the current goat study did show significant enlargement of the tibial tunnel with allograft bone-patellar tendon-bone ACL reconstructions, continuation of the enlargement of the tunnel diameter was not seen beyond 6 weeks after surgery. All grafts appeared to progress through the normal ligamentization process and appeared to heal solidly to the surrounding bony tunnel. The histologic character was similar to that described by Grana et al. 10 of the healing of autograft hamstring tendon within the tibial tunnel. The fate of the allograft bone plug appears to depend on the surrounding biologic environment within the tunnel. When adjacent to host bone, the allograft remodeled and incorporated; when isolated within the fatty medullary canal, it was more likely to be completely resorbed.
The mechanism of tibial tunnel enlargement after allograft ACL reconstruction remains unclear. Our data revealed no apparent correlation between the relatively normal histologic pattern of the tibial tunnel through the various stages of graft incorporation and its enlarged radiographic appearance during the first 6 weeks. Other possible explanations include an immunologic cause, a mechanical cause, or an interaction between the two. A primary immunologic cause is supported by the fact that cytokines, which are produced by immune cells, play a role in bone resorption and remodeling. 12 One of these cytokines, interleukin-1, has been associated with tibial tunnel osteolysis in ethylene oxide-sterilized grafts.19, 26, 32 The potential role of a mechanical cause of tibial tunnel enlargement is supported by observations of tibial tunnel osteolysis in patients with GORE-TEX (W.L. Gore & Associates, Flagstaff, Arizona) ACL grafts. Fukubayashi and Ikeda 9 divided tibial tunnel enlargement into types (line, cone, and cavity) and attributed the enlargement to mechanical friction. Linn et al. 21 also support a mechanical cause for tunnel enlargement by documenting enlargement at the tendinous portion of the graft, where more micromotion was present.
Cytokine production by inflammatory cells could initially retard graft healing, maturation, and incorporation, which would predispose the graft reconstruction to mechanical instability. Berg, 2 in a case report of an allograft ACL reconstruction that failed because of tibial bone plug nonunion, supports this etiologic combination of inflammation and a mechanical mechanism. Graft failure was attributed to anterior tunnel placement, poor bone plug fit, exposure to the synovial fluid environment, inadequate osteogenic stimulus from the allograft, and lack of rigid fixation. Other possible factors contributing to tibial tunnel enlargement include local tunnel bone necrosis caused by thermal injury incurred during reaming and local stress shielding secondary to interference screw fixation. These factors, however, should equally affect autografts.
In summary, allograft tendon undergoes a ligamentization process within the tibial tunnel with biologic fixation to the bony tunnel wall via a dense connective tissue interface, similar to that described in autograft hamstring tendons by Grana et al. 10 Fixation at the bone plug-host interface may not be as important as initially theorized because incorporation appeared to take place in spite of histologic and radiographic evidence of bone plug resorption. A local inflammatory response was noted in only one animal and was believed to be associated with a local immunologic response. Progressive tibial tunnel enlargement was not demonstrated radiographically within the first 36 postoperative weeks. The phenomenon of tibial tunnel enlargement observed in this study is consistent with that seen in humans after allograft ACL reconstruction but did not adversely affect the histologic incorporation of the graft.