
Abstract
Background: A number of clinical conditions of the patellofemoral joint have been correlated with abnormal patellofemoral radiographic measurements.
Hypothesis: An abnormal anteroposterior patellar-tilt angle may be a contributing factor to pathologic conditions of the knee.
Study Design: Prospective nonrandomized clinical trial.
Methods: The anteroposterior patellar-tilt angle was measured in cadaveric knees to determine the best knee position. The radiographs of normal subjects and patients with patellar tendinitis or patellofemoral pain syndrome were examined for differences in patellar-tilt angle.
Results: Cadaveric measurements demonstrated highest intertester and intratester reliability at 30° of knee flexion and neutral femoral rotation. Intratester measurements on normal subjects exhibited high reliability, with a mean anteroposterior tilt angle of 30.8° ± 6.7°. In the patellofemoral pain group the mean anteroposterior tilt angle was 29.1° ± 8.5°; however, for patients with patellar tendinitis, it was 25.6° ± 7.0°, significantly lower than in the normal population. Furthermore, there was no difference between the angles of involved and uninvolved knees of patients with unilateral patellar tendinitis.
Conclusion: The anteroposterior patellar-tilt angle is a clinically reliable measurement of patellar tilt in the sagittal plane that can be used to study patellofemoral tilt in a variety of clinical situations. The results of this study demonstrate that patients with patellar tendinitis have abnormal patellar tilt in the sagittal plane.
The use of radiographic imaging of the patellofemoral joint has been well described in the literature.1, 2, 13, 15, 20, 24 Routine knee radiographs, including standing AP, axial, and lateral views can provide valuable information on patients with pathologic conditions of the patellofemoral joint.7, 11, 26 A radiographic view taken in the sagittal plane (lateral view) can reveal considerable information about the patella. Patellar size, height, and thickness can be reliably determined from a sagittal view. 26 General shape and morphologic structure of the patella can be evaluated to determine whether there is arthrosis or subchondral sclerosis. In addition, evidence of calcification in the patellar tendon can be determined from the sagittal view. 13 Axial views of the patellofemoral joint can provide useful information on patellofemoral tracking and congruence. Knowledge ofpatellofemoral mechanics in the sagittal plane may lead to a greater understanding of normal and pathologic patellofemoral function. However, no measurement technique has been described to determine anteroposterior (AP) patellofemoral tilt in the sagittal plane.
We define a new radiographic measurement called the AP patellar-tilt angle to determine AP patellofemoral tilt in the sagittal plane. This angle is obtained from a lateral radiograph and is created by the intersection of a line drawn along the anterior cortex of the distal femoral diaphysis and a line drawn along the central longitudinal ridge of the articular surface of the patella. It has been hypothesized that abnormal patellar tilt may be a contributing factor to patellar tendinitis, infrapatellar contracture syndrome, or Hoffa's fat pad syndrome.9, 25, 27, 28 Surprisingly, there is a lack of evidence in the literature to support these associations.
The purposes of this study were 1) to establish the reliability of the AP patellar-tilt angle and the effect of knee flexion angle and femoral rotation on the AP patellar-tilt angle in a cadaveric model, 2) to identify the normal range for the AP patellar-tilt angle in humans, 3) to determine the intratester and intertester measurement reliability, and 4) to determine whether there are differences in AP patellar-tilt angle between asymptomatic subjects and patients with patellofemoral pain syndrome and patellar tendinitis.
Materials and Methods
Measurement Technique
Palpating the superior and inferior poles of the patella and determining the relationship between the surrounding landmarks can clinically identify patellar tilt in the sagittal plane.7, 18, 23 This measurement may also be obtained from a lateral radiograph of the knee. To provide such a quantitative measurement, we proposed using two lines that normally meet to form an angle called the AP patellar-tilt angle (Fig. 1). The first of these lines (A-A1) joins two points along the anterior cortex of the distal femoral diaphysis. The second (B-B1) is a line drawn along the central longitudinal ridge of the articular surface of the patella. The selection of the points of reference on the patella for the second line (B-B1) can be complicated by the fact that the contours of the articular surface of patellae vary. When incongruity of the articular side of the patella exists, the patellar line is drawn along the two most posterior extensions of the posterior patellar surface. This selection of landmarks is consistent with the established work of Blackburne and Peel, 4 who demonstrated excellent reliability with use of these landmarks to measure patellar height. The intersection of lines A-A1 and B-B1 forms an angle that we refer to as the AP patellar-tilt angle (Fig. 2). This angle constitutes an objective measurement for the interpretation of lateral radiographs.
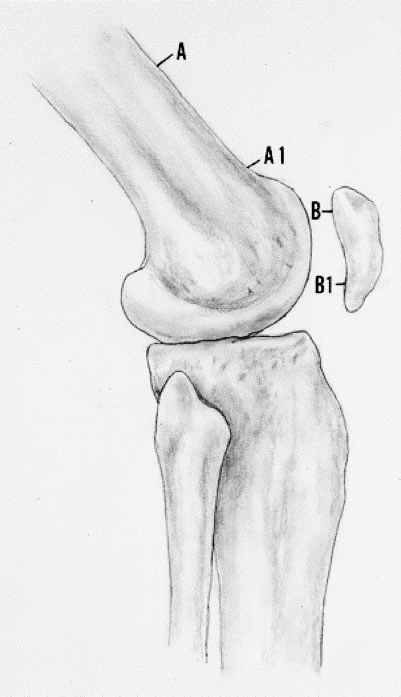
The points selected for measurement of the AP patellar-tilt angle. Line A-A1 passes along the anterior cortex of the distal femoral diaphysis. Line B-B1 passes along the central longitudinal ridge of the articular surface of the patella.
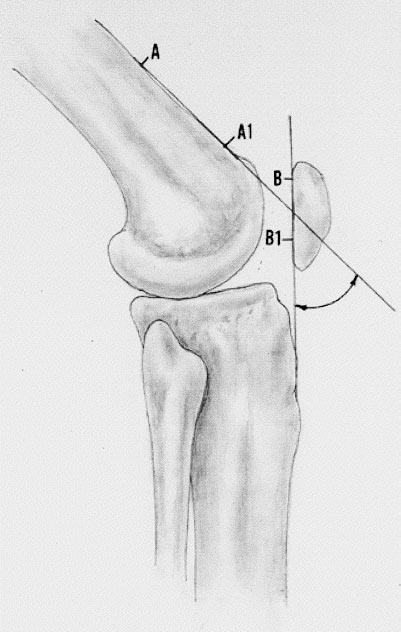
The AP patellar-tilt angle is formed by the intersection of lines A-A1 and B-B1
Part I: Measurement Validation
Radiographs were obtained of five fresh-frozen knee specimens from different cadavers to establish AP patellar-tilt angle reliability and the effect of knee flexion angle and femoral rotation. The specimens were thawed for 18 hours and the skin was then resected. The remaining muscle-tendon units were left entirely intact. A Steinmann pin was secured to the anterior femoral cortex, perpendicular to the long axis of the femur, 20 cm above the joint line. Bunnell's sutures of No. 5 Ethibond (Ethicon, Inc., Somerville, New Jersey) were securely placed through the distal 10 cm of each of the quadriceps muscles and sutured to the Steinmann pin to maintain quadriceps muscle tension throughout testing. A bubble inclinometer (Baseline Inclinometer, Irvington, New York) was fastened with a Kirschner wire to the anterior femoral cortex, proximal to the Steinmann pin.
Each specimen was then independently positioned on a standard Merchant table at three knee flexion angles (30°, 45°, and 60°) and at three different degrees of femoral rotation (-10°, 0°, and +10°). Measurements of the knee flexion angle were confirmed by goniometric measurement. Femoral rotation was determined by the inclinometer fastened to the anterior femoral cortex. Radiographs were obtained at each combination of knee flexion and femoral rotation angle, for a total of nine trials for each specimen.
A trial consisted of a single standard lateral radiograph taken 45 cm perpendicular to the knee with the beam directed at the center of the knee. 26 The AP patellar-tilt angle was then independently measured by two investigators for intertester reliability and then repeated by one of the investigators for intratester reliability. These investigators were blinded to prior measurements. The results were recorded and used to determine intratester and intertester reproducibility as well as to determine the knee position that provided the most reproducible results.
Part II: Normal Value Assessment
The specific measurement position for obtaining the AP patellar-tilt angle was established on the basis of the results of Part I. With use of this technique, radiographs were made of 58 normal knees of subjects who were undergoing evaluation of their contralateral knee for meniscal lesions. The internal review board of our institution approved this project, and each subject gave informed consent. The mean age of the sample group was 40 ± 14 years. Inclusion criteria consisted of no previous or current pathologic conditions of the knee, normal results of a clinical examination, and no radiographic evidence of arthritis. The lateral radiographs were used to establish normative values for the AP patellar-tilt angle. Measurement of the AP patellar-tilt angle was repeated three times by one investigator to establish intratester reliability. A different investigator made an additional measurement to establish intertester reliability. All markings were erased from the radiographs after AP patellar-tilt angles were calculated, and repeated measurements by the same investigator were separated by 1 week. The investigators were blinded to the identity of the subjects.
In addition to the lateral radiograph, weightbearing AP, axial, and 45° flexed posteroanterior radiographs were obtained. Axial views were taken as described by Merchant et al., 24 with the knee flexed at 30°. Posteroanterior views were taken as described by Ghelman and Hodge. 11 The lateral radiographs were obtained with the normal knee resting on a standard Merchant table and flexed at 30° (see “Results,” Part I). The radiographic knee flexion angle was measured and repeated if the angle was not exactly 30°. The x-ray tube was positioned 45 cm from the knee and was directed perpendicular to the center of the knee. Proper flexion angle of the knee was confirmed clinically with goniometric measurement of the knee and radiographically by measuring the radiographic tibiofemoral angle. Positioning the limb in neutral femoral rotation 2 and instructing the patients to relax their quadriceps muscles further standardized the radiographs. 19 All radiographs were performed by one of two experienced radiographic technicians. Congruence angle 24 and the lateral patellofemoral angle of Laurin 20 were measured from the axial radiographs, and the modified Insall-Salvati ratio3, 15 and the AP patellar-tilt angle were measured from the lateral radiograph. These common radiographic measurements were made to verify a normal patellofemoral joint.
Part III: Correlation with Pathologic Conditions
Lateral radiographs were obtained of 83 knees (61 patients) that met the inclusion criteria of the presence of one of two isolated pathologic conditions of the knee (patellar tendinitis or patellofemoral pain). There were 5 patients with bilateral patellar tendinitis, 14 patients with unilateral patellar tendinitis, 17 patients with bilateral patellofemoral pain syndrome, and 25 patients with unilateral patellofemoral pain syndrome. Only patients with symptoms of anterior knee pain and tenderness on palpation of the patellar tendon or the inferior pole of the patella or both were included among the group with patellar tendinitis. Patients with knee effusions, radiographic evidence of arthritis, or pain and tenderness in other areas were excluded from this group. 32 All patients categorized as having patellofemoral pain syndrome had pain originating in the patellofemoral joint and lasting for at least 6 months. Patellofemoral pain was defined as tenderness along the medial or lateral retinaculum, pain on compression of the patella against the underlying femur, or tenderness along the medial facet of the patella. 25 Patients with a history of patellar dislocation or patellar instability were excluded. Bilateral AP patellar-tilt angles and modified Insall-Salvati ratios were calculated from the lateral radiographs of all patients.
Data Analysis
Part I: The effects of knee flexion angle and femoral rotation on the AP patellar-tilt angle were examined by repeated-measures analysis of variance. Intra- and intertester reliability were assessed by Pearson product moment correlation coefficients. Part II: Intratester reliability for the normative data was assessed by intraclass correlation coefficient (1,3). Intertester reliability was assessed by the Pearson product moment correlation coefficient. Part III: Paired t-tests were used to compare the AP patellar-tilt angles of the involved with the uninvolved knees. An analysis of variance was used to compare the means of the three groups with a post hoc analysis if significant differences were found.
Results
Part I: Measurement Validation
Anteroposterior patellar-tilt angle measurements increased with increasing knee flexion (P < 0.01). At 0° of femoral rotation and 30°, 45°, and 60° of knee flexion, the mean (±SD) AP patellar-tilt angles measured 34° ± 8°, 41° ± 7°, and 45° ± 1°, respectively. Alteration of femoral rotation failed to have a significant effect on the AP patellar-tilt angle. At 30° of knee flexion, the mean AP patellar-tilt angle was 35° ± 8° with 10° of internal rotation, 34° ± 8° with neutral rotation, and 35° ± 8° with 10° of external rotation (P = 0.73). The correlation coefficients for interobserver and intraobserver reliability at 30° of knee flexion and in neutral rotation were 0.99 and 1.0, respectively; at 45° of flexion, 0.99 and 0.99, respectively; and at 60° of flexion, 0.87 and 0.94, respectively. Given the comparable reliability of the different knee flexion angles, the position of 30° was chosen on the basis of the common use of this angle for other radiographic measurements. 26
Part II: Normal Value Assessment
The mean knee flexion angle during the radiographic measurements was 31.5° ± 4.6°. The mean AP patellar-tilt angle for the study group was 30.8° ± 6.7°. The 95% confidence interval was 17.4° to 44.2°. Assessment of inter- and intraobserver reliability revealed correlation coefficients of 0.989 and 0.990, respectively (P < 0.001).
Mean values and 95% confidence intervals for the subjects’ modified Insall-Salvati ratios were 1.3 ± 0.2 and 0.9 to 1.7, respectively. For the congruence angle, these values were -2.5° ± 10.2° and -22.8° to 17.8°, respectively. Fifty of the subjects had a laterally opening patellofemoral angle of Laurin, seven a medially opening angle, and one had a parallel joint (no angle). The absolute means and 95% confidence intervals of these angles were 7.4° ± 6.4° and -5.4° to 20.2°, respectively.
The intraclass correlation coefficient for intraobserver reliability for AP patellar-tilt angle was 0.97; 93% of repeated measurements were within 3° of the initial measurement. The mean AP patellar-tilt angles were 32° ± 7° and 33° ± 7° for the two observers (P = 0.36), with an interobserver Pearson product moment correlation coefficient of 0.59 (P < 0.001).
Part III: Correlation with Pathologic Conditions
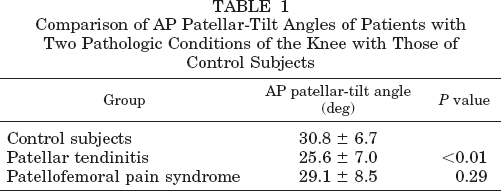
The AP patellar-tilt angle was lower in the patellar tendinitis patients compared with that of the control group (P < 0.01), but it was not different between patients with patellofemoral pain syndrome and control subjects (Table 1). However, the AP patellar-tilt angle was not different between the involved and uninvolved sides in the 14 patients with unilateral patellar tendinitis or the 25 patients with unilateral patellofemoral pain syndrome. The modified Insall-Salvati ratio was not different between the knees with tendinitis and the contralateral knees (P = 0.24). Patella alta (modified Insall-Salvati ratio >0.2) was found in two knees with tendinitis and one contralateral knee. None of the control subjects had patella alta.
Comparison of AP Patellar-Tilt Angles of Patients with Two Pathologic Conditions of the Knee with Those of Control Subjects
Discussion
Accurate radiographic and clinical measurements, which enable objective description of patellar position in both the coronal and axial planes, are frequently used in clinical practice and investigational studies.11, 21, 26 Patellar malalignment has been implicated as a frequent cause of patellofemoral dysfunction.2, 4, 7–11, 15, 19, 20, 24 Patellar kinematics are defined by six degrees of motion: 1) lateral or medial coronal translation, 2) superior or inferior coronal translation, 3) sagittal translation, 4) axial rotation, 5) coronal rotation, and 6) sagittal rotation.8, 15, 18 Isolated sagittal translation without tilt is altered by changes in patellofemoral articular competency and is therefore affected primarily by arthritis of the joint. For purposes of this study, knees with radiographic evidence of patellofemoral arthritis were excluded; therefore a discussion of isolated sagittal translation is not warranted. Abnormalities in all other degrees of motion, except for sagittal rotation, have been noted to contribute to patellofemoral dysfunction and are defined radiographically or clinically or both.
Merchant et al. 24 described the congruence angle. Since their initial report, numerous authors have validated the use of this angle for quantifying lateral and medial patellar translation in the coronal plane (patellar subluxation).12, 29, 31 Insall and Salvati 15 described a ratio of the length of the patellar tendon to that of the patella to enable objective definition of superior and inferior coronal translation (patellar height). Likewise, other authors have described similar ratios that define superior and inferior coronal translation of the patella.4, 5, 13 Laurin et al. 19 described the lateral patellofemoral angle, a measurement since shown to be a useful means of quantifying axial plane rotation (patellar tilt).9, 11, 29 Overlapping structures have precluded the description of a radiographic measurement that objectively describes coronal patellar rotation. However, a clinical measurement, the “A angle” as described by Arno, 1 has been used to define this patellar motion.
The results of the current study confirm excellent intratester reliability for measurement of the radiographic AP patellar tilt in the sagittal plane. In the cadaveric model, the AP patellar-tilt angle was unaffected by femoral rotation and was highly reliable when the knee was flexed at 30°. These findings confirm the reproducibility of the measurement with a radiographic position commonly used in the clinical setting. 26 It is well known that limitations are inherent in cadaveric studies in general and this portion of the study in particular. We did not attempt to re-create the tension of live thigh musculature with this model, and therefore, the measured AP patellar-tilt angles in the initial part of this study may have differed from those expected in living specimens. However, these differences were not pertinent during this portion of the study. The goal was not to quantify the normal angle, but rather to confirm the reliability of the measurement and examine whether the measurement was affected by femoral rotation and knee flexion. In Part II of the study, the reliability of the AP patellar-tilt angle was confirmed, and the normal range with normal resting tension in the quadriceps muscles was defined. The range for this angle in the normal population was 30.8° ± 6.7°. Establishment of the normal range enables comparisons with groups of patients with pathologic conditions. This normal range can be used in a way similar to that of the values described by Merchant et al. 24 and Laurin et al. 20
The mean AP patellar-tilt angle of patients with isolated patellofemoral pain syndrome did not differ significantly from that of the normal population, whereas the angle in both the ipsilateral and contralateral knees of patients with patellar tendinitis did. Patellar tendinitis is a soft tissue injury, and patellofemoral pain syndrome is associated with bony congruence and alignment. Therefore, when one considers the likely causes and the symptoms used to define the two conditions, these findings are understandable. Patellofemoral pain syndrome is defined as anterior knee pain localized to the medial or lateral articular patellar surfaces (or facets) or pain within the medial or lateral retinacula or both. It has been hypothesized to result directly from retinacular stress, synovial irritation, articular injury, or a combination of these factors. 8 Among the proposed causes of this disorder are malalignment, including both medial and lateral coronal translation (subluxation), and excessive coronal rotation (tilt).14, 23, 26 For the purposes of this investigation, we chose to define isolated patellofemoral pain syndrome as anterior knee pain without tenderness along the distal tip of the patella or radiographic evidence of arthritis. Patients with distal patellar tip tenderness were excluded, so as to allow direct comparison with patients who had patellar tendinitis. Patients with arthritis were excluded because of concern that osteophytes would affect mobility of the patella and therefore alter the AP patellar-tilt angle. By limiting the definition of patellofemoral pain syndrome to knees with either medial or lateral parapatellar symptoms and excluding those with distal patellar symptoms, the malalignment responsible for patellofemoral pain syndrome would be expected to be coronal plane malalignment (either subluxation or tilt) and not sagittal malalignment. Similar conclusions have been made by other authors.8, 20, 24 Therefore, it is not surprising that the AP patellar-tilt angle in those patients with isolated patellofemoral pain syndrome did not differ from that of the normal population.
Patellar tendinitis is defined as anterior knee pain localized to the inferior pole of the patella, the patellar tendon, or, less frequently, the tibial tubercle.6, 30, 33 Histologic studies have revealed, among other findings, local disruption of collagen fibers and mucoid degeneration, consistent with overuse or increased strain in the affected patellar tendon region.6, 16, 32 In this study, we noted a reduced AP patellar-tilt angle in both the affected and unaffected limbs of those patients with clinical patellar tendinitis. As the AP patellar-tilt angle decreases, the force acting on the patellar tendon and therefore the strain within the tendon would be expected to increase, assuming that all other variables remain constant. 17 Clinical and biomechanical studies have suggested that activities producing greater quadriceps muscle forces predispose a person to the development of patellar tendinitis.17, 30 The results of this study indicate that a reduced AP patellar-tilt angle may also be a predisposing factor for the development of patellar tendinitis.
It is possible that altered patellofemoral mechanics, prolonged quadriceps muscle inhibition, or a reduced activity level due to longstanding patellar discomfort might have led to the reduced AP patellar-tilt angle that was observed. However, this would not explain a normal AP patellar-tilt angle in patients with isolated patellofemoral pain syndrome, nor would it explain significantly reduced AP patellar-tilt angles in the contralateral knees of those patients with patellar tendinitis. Rather, the findings suggest a predisposition to the development of patellar tendinitis in persons with a reduced AP patellar-tilt angle. Symptoms may then manifest themselves when such a person participates in at-risk activities. 30
The reason why patellar tendinitis developed in only one limb if both limbs have similar AP patellar-tilt angles is unclear. The developmental causes of patellar tendinitis and of patellofemoral pain syndrome are multiple. A reduced AP patellar-tilt angle is only one of a number of factors that may lead to patellar tendinitis. Richards et al. 30 observed that asymmetry in ground reaction force patterns, external tibial torsional moments, and large knee angles predicted who would develop patellar tendinitis. In an MRI study of subjects with patellar tendinitis, the authors identified a significant thickening of the patellar tendon. 16 This study did not compare the involved knee with the uninvolved knee. Therefore, it is possible that patellar tendon thickness may be a predisposing factor, although there are no studies that clearly demonstrate that thickening is a predisposing factor for patellar tendinitis. Ferretti et al. 6 found that of 18 knees with patellar tendinitis, 10 had normal knee extensor mechanisms, and the remaining 8 had a normal Q angle but had vastus medialis obliquus dysplasia. In only two cases was there evidence of patella alta, which is similar to the results of the present study.
We suggest that of the numerous factors responsible for patellar tendinitis, reduced AP patellar-tilt angle is important. Considering the relatively large overlap of the data from the normal subjects compared with that of subjects with pathologic conditions, as evidenced by the small difference between the means and the large standard deviation, this measurement may be of limited clinical use. However, the findings do suggest that a reduced AP patellar-tilt angle is an etiologic factor for patellar tendinitis. The measurement could be used in future research to prospectively assess the risk for developing patellar tendinitis. Further study is necessary to corroborate our findings, to identify the significance of sagittal malalignment in other processes of the knee, and to determine whether it can be affected by clinical intervention to alter the course of such disorders.
Summary
We described the AP patellar-tilt angle, an easily measured radiographic angle that has been found to be reproducible. The average AP patellar-tilt angle in the normal population was 30.8° ± 6.7°. A significantly reduced AP patellar-tilt angle was identified in the knees of patients with patellar tendinitis. This decrease in AP patellar tilt may place excessive stress on the patellar tendon and predispose an athlete to the development of patellar tendinitis in at-risk subjects.