
Abstract
Background: Medial collateral ligament insufficiency of the elbow with resultant valgus instability in throwing athletes is typically treated with free tendon graft reconstruction as described by Jobe.
Hypothesis: Improved results could be obtained with the use of the docking technique.
Study Design: Uncontrolled retrospective review.
Methods: The study group consisted of 36 athletes who had symptomatic insufficiency of the medial collateral ligament confirmed by magnetic resonance imaging and by surgical findings. Average follow-up was 3.3 years. Key elements of the docking technique included a muscle-splitting approach without routine transposition of the ulnar nerve, routine arthroscopic assessment, treatment of associated lesions, and docking the two ends of the tendon graft into a single humeral tunnel.
Results: Thirty-three of 36 patients (92%) returned to or exceeded their previous level of competition for at least 1 year, meeting the Conway-Jobe classification criteria of “excellent.” All 22 professional or collegiate athletes returned to or exceeded their previous competition level.
Conclusions: The docking technique allowed simplified graft tensioning and improved graft fixation.
The medial collateral ligament (MCL) of the elbow is a frequent site of serious injury in the athlete performing overhead arm motions, particularly the competitive baseball pitcher.2, 5, 13, 15, 16, 21, 30, 32, 34, 35 The baseball pitch generates a large valgus force at the elbow (estimated at 290 N) that peaks during the late cocking and early acceleration phases of the throwing motion.4–6, 8, 10, 11, 23, 36 The anterior bundle of the MCL is clearly the primary restraint to valgus stress within this range of motion14, 19, 20, 26, 27, 31 and must withstand repetitive loads that are estimated to approach the tensile strength of the ligament.6, 10 The ultimate tensile strength of the MCL in resisting valgus torque has been reported to be 33 N·m.2, 10 The static torque on the MCL during pitching has been estimated at 32 N·m. 6 Resulting microtrauma combined with incomplete recovery can lead to inflammation and attenuation of the ligament.2, 5, 15, 31, 32 Injury or attenuation of the MCL leads to abnormal valgus rotation of the elbow, 3 which affects the mechanics of the highly con-strained articulation of the posterior elbow and results in bony impingement at the superomedial corner of the olecranon and the corresponding fossa.5, 18, 28 Such impingement can lead to chondral lesions and eventually to reactive changes such as osteophytic spurs, which in turn add to the impingement process (Refs. 1, 2, 18; N. M. Breazeale et al., unpublished data, 1999). This pathologic process has been termed “valgus extension overload.”2, 18, 28
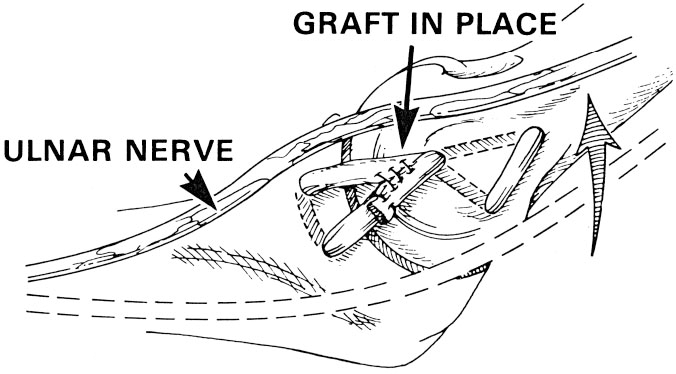
Surgical treatment of the torn MCL in a throwing athlete has been performed for the past 2 decades. Dr. Frank Jobe was the first to describe a reconstructive technique that included a free tendon graft placed in bone tunnels in the humerus and ulna. 15 The Jobe procedure was originally performed by sectioning the flexor pronator muscle origin to expose the MCL and transposing the ulnar nerve. Three holes were drilled in the medial epicondyle; the tendon graft was pulled through the resulting bony tunnels in a figure-of-8 fashion and sutured to itself under appropriate tension (Fig. 1). 15
Our early experience with the Jobe procedure raised several areas of concern. These included the strength of the suture fixation of the free tendon graft, adequate tensioning of the graft at the time of final fixation, and the potential for complications resulting from the detachment of the flexor origin and the three large drill holes in the medial epicondyle. We were concerned about the routine transposition of the ulnar nerve and the resulting high rate of ulnar nerve-related complications.5, 15 We were also concerned about the ability of the surgeon to recognize and treat concurrent intraarticular pathologic conditions. These concerns ultimately led to several modifications of the Jobe procedure, which we named the “docking technique” and which are outlined in this report. The goals of the docking technique modifications are 1) to perform a tendon graft reconstruction of the MCL through a muscle-splitting “safe-zone” approach; 2) to avoid obligatory transposition of the ulnar nerve; 3) to routinely arthroscopically assess and treat intraarticular pathologic conditions, particularly in the posteromedial compartment of the elbow joint; 4) to place the tendon graft in bone tunnels; 5) to reduce the number of humeral drill holes from three, as has previously been described,5, 15 to a single hole in the hope of reducing the invasiveness of the procedure as well as the possible complication of an epicondylar fracture; and 6) to simplify graft tensioning and improve fixation methods.
The purpose of this study was to describe the docking technique modifications and to evaluate the preliminary results of the first 36 patients to be treated with this technique.
Materials and Methods
From October, 1995, through February, 1999, 36 consecutive athletes with diagnosed MCL insufficiency were treated with surgical reconstruction by the senior author (DWA). The indication for reconstruction was medial elbow pain caused by incompetence of the MCL that prevented the athlete from throwing or performing at his or her normal level. The docking technique modification of the Jobe procedure was performed in each patient. The results were retrospectively reviewed and form the basis of this investigation.
The mean age of the patients at the time of the reconstruction was 23 years (range, 15 to 57). All but one of the patients were men, and all but three were between 15 and 28 years of age. The study group included three athletes who were not baseball players: one lacrosse player, one tennis player, and one golfer. This subgroup included the two oldest patients, a 54-year-old competitive golfer and a 57-year-old nationally ranked Masters tennis player. Of the 33 baseball players in the study group, 27 were pitchers: 9 professional baseball pitchers (4 major league and 5 minor league), 12 collegiate pitchers, and 6 high school pitchers. The six nonpitchers included one major league, one minor league, one recreational, and three high school baseball players.
The diagnosis of MCL insufficiency was based on the history, physical examination, MRI examination, and arthroscopic valgus stress testing. Diagnostic criteria included a history of medial elbow pain with throwing or overhead activity that was reproduced with valgus stress testing or was associated with clinically apparent medial elbow laxity, or both; MRI findings clearly consistent with MCL injury (Fig. 2); and negative examination findings for medial epicondylitis. Two patients were exceptions to these criteria. Both patients had clinical and MRI findings consistent with concurrent MCL insufficiency and severe medial epicondylitis and underwent concurrent flexor pronator tendon debridement at the time of MCL reconstruction.

A, complete MCL tear in a 26-year-old male professional baseball pitcher who had marked tenderness over the distal insertion of the MCL after leaving play because of elbow pain. The coronal gradient-echo MR image (repetition time, 56 ms; echo time, 20 ms; flip angle, 10°) shows abnormal signal intensity and morphologic structure of the ulnar insertion (black arrow) of the MCL with a complete tear. Soft tissue edema is present. Note the normal synovial reflection (white arrow) at the humeral insertion of the MCL. B and C, complete tear of the MCL in a 19-year-old male baseball pitcher with a history of chronic elbow pain and prior injury. Coronal images through anterior (B) and posterior (C) aspects of the elbow show a chronic pattern of MCL disruption with regeneration. Note the thickening of the anterior aspect of the MCL (arrow in B) and thinning of the posterior aspect (arrow in C). There is a large posteromedial spur (asterisk in B). (Reprinted with permission of the American Journal of Roentgenology [Garry et al. 12 ])
All patients underwent at least one MRI scan of the involved elbow, and scans were interpreted by the same musculoskeletal radiologist. In each patient, the MRI scan showed recognizable patterns of acute or chronic injury of the MCL (Fig. 2).12, 24, 25 In addition to the previously discussed diagnostic criteria, the presence of MCL insufficiency was confirmed at surgery, before reconstruction, with examination under anesthesia, arthroscopic examination (see “Operative Technique”), or, in some cases, open inspection of the ligament.
The mean length of time between the onset of symptoms and reconstruction of the ligament was 24.5 months (range, 0.5 to 60). Five of the patients (14%) had had previous surgery on the ipsilateral elbow, at a mean of 18 months (range, 6 to 60) before this operation. In one patient, a previous MCL reconstruction with suture anchor fixation was unsuccessful. Other previous operations included transposition of the ulnar nerve in one patient, arthroscopic removal of a loose body from the elbow in three, diagnostic arthroscopy in two, and debridement of osteophytes around the elbow in two. In the majority of patients, prior treatment had consisted of prolonged therapy for presumed medial epicondylitis. Only one patient had previously received cortisone injections about the medial elbow.
Final follow-up was achieved in each case by telephone interview. The athlete's postsurgical level of competition was obtained, from the completion of rehabilitation to the time of final follow-up. A successful result was defined as a return to the preinjury level of competition for at least 1 year, as described by Conway et al. 5 This outcome measure is the primary measure used in all reported series of MCL reconstructions of the elbow. It inherently controls for subjective bias of performance by measuring only the level of competition achieved and the time the athlete was able to compete at this level. This outcome measure is discussed further in the “Discussion” section.
Operative Technique
Each patient was examined preoperatively for the presence of a palmaris longus tendon, our preferred source of tendon graft. For patients in whom a palmaris tendon was lacking or insufficient, an ipsilateral gracilis tendon or toe extensor tendon was used. Trimming of the gracilis tendon graft was sometimes necessary to allow a proper fit in the bone tunnels. In addition, each patient was examined preoperatively for findings of ulnar nerve irritability, instability, or neuropathy. Electromyography was not routinely performed in the setting of a normal neurologic examination. Our indications for ulnar nerve transposition included positive examination findings with a history of preoperative symptoms attributable to the ulnar nerve.
We generally performed the procedure with axillary block anesthesia. After the block was in effect, a tourniquet was placed on the upper arm. The patient remained supine on the operating table while the hand and arm were prepared and draped in the usual fashion. With use of a McConnell arm holder (McConnell Orthopedic Manufacturing Company, Greenville, Texas), the humerus and forearm were placed in a position with the forearm across the patient's chest (Fig. 3). This position allowed the arthroscopy to be performed with the elbow in a position that mimicked the prone position.

Supine patient positioning for elbow arthroscopy with the McConnell arm holder.
The arthroscope was introduced through a lateral portal into the anterior compartment. A diagnostic arthroscopic examination was performed of the anterior compartment to evaluate the articular surfaces and the synovium and identify any loose bodies. An arthroscopic stress test for the MCL could be performed at this time.9, 33 With the elbow at 90° of flexion, the forearm was pronated and valgus stress was applied. In the normal elbow, a maximum of 1 to 2 mm of medial opening will be observed. If the MCL is incompetent, greater than 3 mm of opening between the coronoid and the medial humerus will be observed.9, 33 This pathologic opening was observed in all 36 patients.
The arthroscope was then removed, leaving the cannula in place, and the gravity inflow tube was introduced through it. After the joint was distended, a posterolateral portal was created and the arthroscope was inserted into the posterior compartment. The olecranon and humeral fossae were evaluated for spurs or loose bodies. The medial humeral condyle was evaluated for articular injury. Finally, the posterior radiocapitellar joint was evaluated by advancing the arthroscope down the lateral gutter. If an operative procedure was necessary, such as a spur removal, a transtriceps portal was created through the center of the tendon at the level of the olecranon tip. The most common pathologic condition encountered was a fragmented spur on the medial border of the olecranon, which was debrided with a suction shaver to normal bony architecture. In addition, loose bodies could be present in or about the radiocapitellar joint. If present, a new portal through the anconeus muscle was usually necessary for removal.
Once the arthroscopic procedure was completed, the arm was released from the arm holder and placed on the hand table below. The ipsilateral palmaris longus tendon was harvested through a 1-cm incision placed in the distal wrist crease. Rather than performing multiple incisions, we used a tendon stripper specially made for harvesting the palmaris longus tendon. At the time of harvest, we placed a No. 1 braided nonabsorbable suture using a No. 1 Ethibond Excel OS-2 needle (Ethicon, Inc., Somerville, New Jersey) in a Krakow fashion in one end of the tendon. After harvest, the tendon was placed in a moist sponge on the back table.
The arm was exsanguinated to expose the MCL and the tourniquet was inflated. An incision was created from the distal third of the intramuscular septum across the medial epicondyle to a point 2 cm beyond the sublime tubercle of the ulna. While exposing the fascia of the flexor pronator muscle, we were careful to identify and preserve the antebrachial cutaneous branch of the median nerve, which frequently crossed the operative field. The fascia of the flexor carpi ulnaris muscle was incised longitudinally and bluntly split to expose the underlying ligament (Fig. 4). Once the ligament had been exposed, a deep, blunt, self-retaining retractor was placed to maintain exposure (Fig. 5A). The anterior bundle of the MCL was incised longitudinally to expose the joint. At this point, MCL laxity was confirmed by observing the separation of the joint surfaces by 3 mm or more with valgus stress (Fig. 5B).
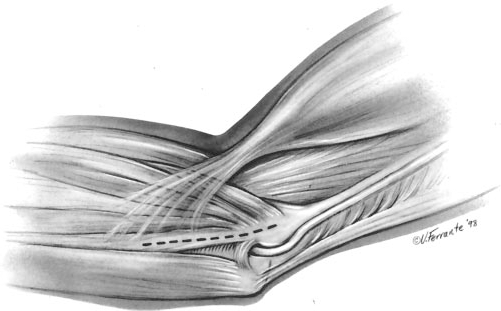
Muscle-splitting incision through the flexor carpi ulnaris muscle. (Reprinted with permission of Hospital for Special Surgery, New York, New York.)
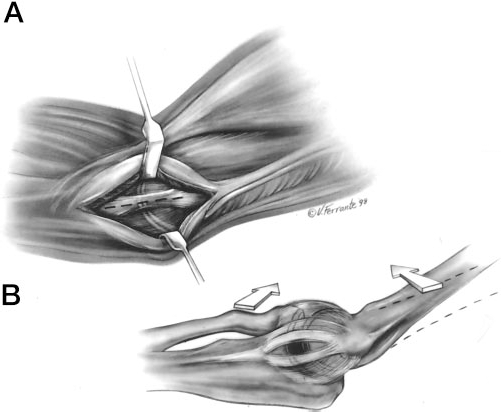
A, submuscular exposure of the MCL. B, assessment of joint laxity after a longitudinal incision of the native ligament. Note the opening (in black) between the medial ulnohumeral articulation with valgus stress. (Reprinted with permission of Hospital for Special Surgery, New York, New York.)
The tunnel positions for the ulna were exposed. The posterior tunnel position required the surgeon to expose the ulna subperiosteally 4 to 5 mm posterior to the sublime tubercle while meticulously protecting the ulnar nerve. If the nerve was seen to subluxate anteriorly such that it could not be adequately protected, a transposition of the ulnar nerve was performed. Tunnels were made anterior and posterior to the sublime tubercle by using a 3-mm bur to create a 2-cm bridge between them. The tunnels were connected using a small, curved curette, and the surgeon took care not to violate the bony bridge (Fig. 6A). A No. 1 Ethibond Excel OS-2 needle was then used to pass a looped 2.0 suture.
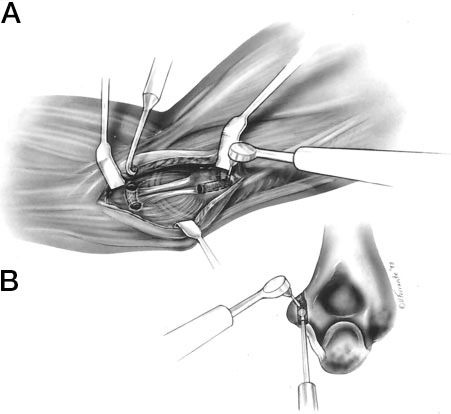
A, creation of the ulnar tunnel using a curved curette to connect the ulnar holes. B, creation of the single humeral tunnel and the exit punctures for the two suture bundles using the dental bur. (Reprinted with permission of Hospital for Special Surgery, New York, New York.)
The humeral tunnel position was located in the anterior half of the medial epicondyle in the anterior position of the existing MCL. The previous longitudinal incision in the native ligament was extended proximally in line with its fibers to expose the humeral origin. Small blunt retractors were used to protect the fibers anterior and posterior to the tunnel site. A longitudinal tunnel was created up the axis of the medial epicondyle to a depth of 15 mm by using a 4-mm bur (Fig. 6B). The upper border of the epicondyle, just anterior to the intramuscular septum, was exposed. With use of a dental drill with a small bit, two small exit punctures separated by 5 mm to 1 cm were created to allow suture passage from the primary humeral tunnel (Fig. 6). A suture passer was used from each of the two exit punctures to pass a looped suture, to be used for later graft passage.
With the elbow in forearm supination and mild varus stress, the horizontal incision in the native MCL was repaired with a 2.0 absorbable suture. The graft was then passed through the ulnar tunnel from anterior to posterior. The limb of the graft that had sutures already in place was passed into the humeral tunnel, and the sutures were pulled through one of the small superior humeral punctures (Fig. 7). With this first limb of the graft securely docked in the humerus, the elbow was again reduced with maximum forearm supination and gentle varus stress. While tension was maintained on the graft, the arm was moved so that the elbow ranged from flexion to extension to eliminate potential creep within the graft. The final length of the graft was estimated by placing the free limb of the graft adjacent to the humeral tunnel and visually estimating the length of the graft that would allow the graft to be tensioned within the humeral tunnel (Fig. 7). This point was marked with dye and a No. 1 braided nonabsorbable suture was placed in a Krackow fashion (Fig. 7). The excess graft was excised immediately above the Krackow stitch. This end of the graft was docked securely in the humeral tunnel with the sutures exiting the small puncture holes.
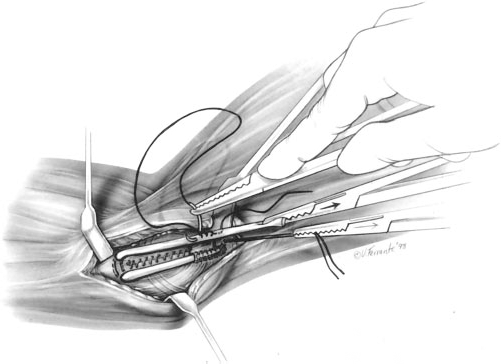
The posterior limb of the graft was docked in the humeral tunnel. The elbow was reduced with varus stress, and, after final tensioning of the graft, a Krackow stitch using No. 1 Ethibond was placed in the anterior limb of the graft. (Reprinted with permission of Hospital for Special Surgery, New York, New York.)
Final graft tensioning was performed by again placing the elbow through a full range of motion with varus stress placed on the elbow. Once the surgeon was satisfied with the graft tension, the two sets of graft sutures were tied over the bony bridge on the humeral epicondyle (Fig. 8). The tourniquet was deflated and the wound was copiously irrigated. Closure was performed by approximating the flexor carpi ulnaris fascia and subcutaneous and subcuticular closure. After surgery, the elbow was placed in a plaster splint at 60° of flexion.
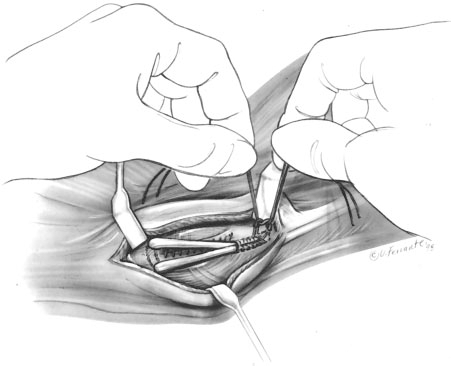
The anterior limb was passed into the humeral tunnel, and the sutures from both limbs were tied over the bone bridge to secure the graft. (Reprinted with permission of Hospital for Special Surgery, New York, New York.)
Postoperative Management
The arm was maintained in the immediate postoperative splint for 1 week, at which point the sutures were removed and the elbow was placed in a hinged brace. Initially, motion was allowed between 45° of extension and 90° of flexion. Over the following 5 weeks, motion was gradually advanced to full. Wrist motion was allowed immediately postoperatively because we believed that the benefits of early wrist motion outweighed the risks of mild pronation during this period. However, the patient was instructed to perform gentle wrist flexion and extension and to avoid pronation.
Formal physical therapy was begun 6 weeks postoperatively. Any residual losses of elbow motion were corrected, and gradual strengthening of the forearm and shoulder musculature was commenced. Care was taken not to apply a valgus load across the elbow during this phase of rehabilitation. At 12 weeks, the strengthening program became more vigorous, and activities such as bench pressing light to moderate weights were allowed. At 4 months, a throwing program was commenced, beginning with short tossing. Pitching from flat ground was started in month 6 and from the mound at month 7. Generally, players did not pitch in competitive situations until 9 months after the operation.
Results
The operative technique resulted in adequate exposure of the origin and insertion sites of the MCL in every case. A taut graft was achieved on the operating table, without pullout of the Krackow stitch or suture breakage, in each case. Palmaris longus tendon autograft was used in 34 of 36 cases. In two cases a palmaris tendon was not present, and a gracilis tendon and toe extensor tendon were used. Tendon graft sources and harvesting methods resulted in more than sufficient graft length in each case.
Seven patients underwent MCL reconstruction before our routine use of elbow arthroscopy as part of the reconstructive procedure. The remaining 29 patients underwent elbow arthroscopy just before ligament reconstruction. In 13 of these patients (45%), osteophytes were removed arthroscopically from the posteromedial margin of the olecranon or the coronoid process. Two patients underwent ulnar nerve transposition secondary to preoperative clinical findings consistent with chronic ulnar nerve instability or compression. A subcutaneous transposition with a fascial sling was performed.
At a mean follow-up of 3.3 years (range, 2.1 to 5.3), 21 patients had returned to their previous level of play for at least 1 year. An additional 12 patients had exceeded their previous level of competition and had competed at a higher level for at least 1 year. Thus, 33 of 36 patients (92%) met the Conway-Jobe classification 5 of “excellent” by returning to the previous level of competition for a 1-year period. Furthermore, no professional or collegiate athletes undergoing MCL reconstruction with the docking technique failed to return to their previous competition level.
There were two minor postoperative complications: a wound hematoma and mild paresthesia in the ulnar nerve distribution. Both resolved within 3 weeks. An additional patient treated before routine arthroscopy was added required repeat surgery for symptomatic posteromedial impingement, which was treated successfully with arthroscopic debridement. There were no range of motion deficits noted in any patient at follow-up examination; however, goniometric measurements were not taken.
Three patients had poor results. The first patient was treated with ulnar nerve transposition and superficial neuroma excision for chronic neurogenic pain before a diagnosis was made of reflex sympathetic dystrophy in the operated extremity. He was treated successfully with stellate ganglion blocks, and the condition ultimately resolved. The second patient returned to batting practice 7 months postoperatively and fractured the ulnar tunnel while swinging the bat. The patient underwent successful revision reconstruction and returned to his previous level of competition in high school baseball. The third patient, a high school pitcher, was unable to achieve sufficient power during throwing and did not return to competitive pitching.
Discussion
In all reported series of MCL reconstructions of the elbow, the primary outcome measure has been the return, or failure to return, to the player's previous level of competition.2, 5, 15, 30 Although limited in scope, this outcome measure is of particular relevance to MCL reconstruction for several reasons. We do not currently have an accurate objective measure of medial elbow laxity. Although in severe cases laxity can be felt by the examiner, the diagnosis in the majority of cases is made by the presence of medial elbow pain while throwing, helped by the reproduction of pain during valgus stress, and confirmed by MRI findings. Stress radiographs have not exhibited predictable objective reliability.2, 5, 7, 15, 17, 18 Return to elite throwing is a more stringent outcome measure than objective testing performed during a physical examination. The competitive pitcher places more stress on the medial elbow structures than can be achieved in any examination maneuver5, 6, 8, 10, 23, 31 and does it repetitively. Although it is true that return to play is affected by many factors, many of these uncontrolled factors work against the athlete's return to play, even with a good surgical outcome.
Conway et al. 5 reported on the outcome of 56 athletes who underwent MCL reconstruction; 68% returned to their previous level of competition for at least 12 months. Ninety-six percent of the patients were available for follow-up, with an average follow-up period of 6.3 years (range, 2 to 15). These results reflect the first generation of the procedure as originally described. 15 In a later series, Thompson et al. 30 reported 82% of 33 athletes returned to their previous level with a minimum follow-up of 2 years. Azar and coworkers 2 have recently reported on 78 patients who underwent MCL reconstruction. Fifty-nine of the 78 patients (76%) were available for follow-up; 48 of 59 patients (81%) returned to their previous level of competition. The average follow-up period was nearly 3 years (range, 1 to 6). We report on a consecutive series of 36 athletes who underwent MCL reconstructions performed by the same surgeon with level of postoperative performance confirmed by telephone follow-up in 100% of the patients. Our results (92% return to competition) compared favorably with those of previous studies and had a comparable follow-up period (mean, 3.3 years; range, 2.1 to 5.3).
The goals of a reconstructive procedure of the MCL of the elbow are to dependably reproduce the tension, strength, and anatomic attachment sites of the native MCL, while minimizing the risk of morbidity and maximizing tendon-to-bone healing potential. The Jobe procedure pioneered these efforts by introducing a technique of free tendon graft placed in bony tunnels. 15 After early clinical experience with the Jobe procedure, we have expanded and clarified our goals to include preservation of the flexor muscle origin, avoiding obligatory transposition of the ulnar nerve, complete arthroscopic assessment and treatment of associated lesions, and minimizing the number of bony tunnels in the medial epicondyle.
The most prevalent problem in early reports of MCL reconstruction were complications relating to the ulnar nerve.5, 15 Several studies have confirmed that the anterior bundle of the MCL originates from the inferior aspect of the medial epicondyle, not from the medial or anterior surface.3, 19, 22 Because the common tendon of the flexor pronator attachment originates on the body of the medial epicondyle, it is possible to split the attachment longitudinally and expose the origin of the anterior MCL bundle. Smith and coworkers 29 from this institution have described a “safe zone” for MCL exposure through a flexor carpi ulnaris muscle-splitting incision that allows MCL reconstruction to be performed without ulnar nerve transposition or flexor pronator muscle takedown. With this muscle-splitting approach, transposition of the ulnar nerve is not necessary for surgical exposure. Thus, the decision for transposition can be made on the basis of clinical indications.
There has been significant variation in the reported prevalence of ulnar nerve involvement with MCL laxity.2, 5, 30 Later studies using either a muscle-splitting approach or routine subcutaneous transposition have reported a much lower incidence.2, 30 Thompson et al. 30 have reported on the short-term results of 83 patients who underwent MCL reconstruction using a muscle-splitting approach. Only one patient (1%) had transient ulnar neuropathy lasting longer than 3 weeks postoperatively. In our series, only two patients had significant preoperative ulnar nerve findings warranting transposition. The absence of significant complications relating to the ulnar nerve in our series suggests that it may be beneficial to leave the normal cubital tunnel anatomy intact.
The pathologic process of valgus extension overload suggests that intraarticular pathologic conditions can be present posteromedially as well as in the lateral compartment in patients with MCL insufficiency (Refs. 1, 2, 5, 18, 28; N. M. Breazeale et al., unpublished data, 1999). Although many associated lesions can be treated through a posterior arthrotomy at the time of ligament reconstruction, preoperative recognition of the lesion is necessary. In addition, posterior arthrotomy necessitates transposition of the ulnar nerve. Arthroscopic examination of both the anterior and posterior compartments allows recognition of intraarticular pathologic conditions that may not be recognized on preoperative imaging studies. In this series, 13 of 29 patients (45%) who underwent arthroscopic examination had arthroscopically treatable lesions, particularly impingement lesions such as fragmented spurring. Of these patients, detection of the lesions on preoperative imaging studies occurred in only 8 of 13 cases.
We believe that the docking modifications provided significant improvement of technical issues such as graft fixation and tensioning. Previous authors have used two divergent humeral tunnels, resulting in three drill holes in the medial epicondyle. The tendon graft was then pulled through the resulting bony tunnels in a figure-of-8 fashion and sutured to itself (Fig. 1).2, 5, 15 Potential disadvantages of this technique were the relatively high number of large drill holes within the limited area of the epicondyle, the difficulty in holding tension on the graft during fixation, and the strength of tendon fixation. In our experience, a properly placed Krackow stitch with No. 1 Ethibond suture allowed the surgeon to pull maximally on the graft while tying over a bony bridge, providing strong fixation and greatly facilitating graft tensioning. In addition, the single-tunnel modification resulted in a single drill hole in the epicondyle.
Reconstruction of the MCL of the elbow has been shown to be a dependable procedure in the throwing athlete with a diagnosis of MCL insufficiency. Athletes of all skill levels can expect a high rate of return to their previous level of play. The results of this study suggest that previous success rates can be matched and even improved using the docking technique modifications.