
Abstract
Background: Nonoperative treatment of traumatic shoulder dislocations leads to a high rate of recurrent dislocations.
Hypothesis: Early arthroscopic treatment for shoulder dislocation will result in a lower recurrence rate than nonoperative treatment.
Study Design: Prospective, randomized clinical trial.
Methods: Two groups of patients were studied to compare nonoperative treatment with arthroscopic Bankart repair for acute, traumatic shoulder dislocations in young athletes. Fourteen nonoperatively treated patients underwent 4 weeks of immobilization followed by a supervised rehabilitation program. Ten operatively treated patients underwent arthroscopic Bankart repair with a bioabsorbable tack followed by the same rehabilitation protocol as the nonoperatively treated patients. The average follow-up was 36 months.
Results: Three patients were lost to follow-up. Twelve nonoperatively treated patients remained for follow-up. Nine of these (75%) developed recurrent instability. Six of the nine have required subsequent open Bankart repair for recurrent instability. Of the nine operatively treated patients available for follow-up, only one (11.1%) developed recurrent instability.
Conclusions: Arthroscopic stabilization of traumatic, first-time anterior shoulder dislocations is an effective and safe treatment that significantly reduces the recurrence rate of shoulder dislocations in young athletes when compared with conventional, nonoperative treatment.
Numerous studies have shown that conventional, nonoperative treatment of shoulder dislocations in young athletes has resulted in a high rate of recurrence.1, 2, 8, 13–20, 25, 30, 33 Non-operative treatment, which typically includes a short period of immobilization followed by rehabilitation, has resulted in recurrent instability rates ranging from 17% to 96% in patients under 30 years of age. Because of this high rate of recurrence in young patients, some researchers have investigated the role of arthroscopic treatment of patients after shoulder dislocation. Wheeler et al. 30 reported a 22% redislocation rate (2 of 9) in West Point cadets after Bankart repair with an arthroscopically inserted staple. This was in comparison with a 92% failure rate (35 of 38) for patients with nonoperative treatment. Subsequently, Arciero et al., 2 using a transglenoid suture technique in a prospective study of 36 cadets at the same institution, reported a 14% failure rate (3 of 21) in the operatively treated group compared with an 80% failure rate (12 of 15) in the nonoperatively treated group. In another study of 26 patients with first-time shoulder dislocations, Arciero et al., 1 after repairing the capsulolabral avulsion with a bioabsorbable tack, reported a 10% recurrence rate. In a prospective, randomized study in which transglenoid fixation was used in patients under 30 with first-time shoulder dislocations, Kirkley et al. 20 reported a recurrence rate of 15.8% (3 of 19), compared with 47% (9 of 19) in patients treated nonoperatively. Additionally, a quality of life assessment demonstrated that operatively treated patients had a superior outcome compared with the nonoperatively treated group.
From these studies, it appears that operative treatment for primary anterior shoulder dislocations may reduce recurrence, improve outcome, and avoid the frequent necessity of open reconstructive procedures to treat recurrent instability. There have been many reports of the use of the transglenoid suture technique for arthroscopic Bankart repair. Disadvantages of this technique include the necessity of tying sutures over posterior soft tissue with occasional superficial infections and the potential for suprascapular nerve injury.20, 23 A cannulated bioabsorbable tack to secure the capsulolabral tissue to the glenoid eliminates the need to pass and tie sutures over the posterior glenoid. The relatively simple arthroscopic insertion and bioabsorbability of the tack make this technique an attractive alternative. Warner and Warren 29 first described the use of this tack for arthroscopic Bankart repairs.
The purpose of this article is to report the results of our prospective, randomized study comparing nonoperative treatment of patients with first-time, traumatic shoulder dislocations with early arthroscopic Bankart repair with a bioabsorbable tack in a group of active-duty military personnel.
Materials and Methods
Patients between the ages of 18 and 26 who sustained a primary, traumatic shoulder dislocation that required a manual reduction by medical personnel were prospectively randomized to one of two treatment groups. The referral base included all active-duty military personnel and their families stationed on Oahu who were eligible for care in the military health care system. All patients who sustained a dislocation were referred to our orthopaedic clinic within 48 hours after reduction. The patients were informed of the study design, the expected natural history, and the surgical procedure and risks. Exclusion criteria included the presence of a tuberosity fracture or other concomitant fracture, neurologic injury, or any history of previous shoulder injury, previous subluxation, or dead arm syndrome. Patients who voluntarily entered the study were randomized to one of two groups by using the last digit of their social security numbers; that is, patients with odd numbers were assigned to the operative group. Each patient underwent an MRI scan to allow evaluation of the capsulolabral injury. The protocol was approved by the Clinical Investigation and Human Use Committee of our institution.
In the nonoperatively treated group, patients had their shoulders immobilized for 4 weeks in a sling and then underwent supervised rehabilitation as described under “Rehabilitation.” At 4 months, after rehabilitation, the patients were allowed to return to full active duty, including contact sports.
All operatively treated patients underwent surgery within 10 days of their injury. We used a combination of interscalene and general anesthesia. The interscalene regional anesthesia, which has been described by several authors,5, 7, 21, 27 was performed with the patient awake, thereby providing postoperative analgesia. After the interscalene administration, the patients were administered a general anesthetic, which then allowed examination of the uninjured shoulder without voluntary muscle contraction. The examination under anesthesia included the supine load shift test with the arm abducted at 70° to 90° to document and quantify the degree of anterior instability of the glenohumeral joint when compared with the contralateral side. A 1+ shift described a shoulder that could be brought to the anterior glenoid rim. A 2+ shift meant translation over the glenoid rim with spontaneous reduction after release of the anterior force. A 3+ shift meant glenohumeral dislocation without spontaneous reduction.
All patients were operated on in the beach-chair position as described by Skyhar and associates. 27 The patient was positioned upright and a beanbag was used to project the shoulder girdle away from the operating table and improve exposure. A standard posterior portal was used for visualization. Two portals, an anteroinferior and an anterosuperior, were used for instrumentation. These portals were made by using an outside-in technique guided by a spinal needle for proper placement. The anterosuperior portal was made just off the anterolateral acromion to allow enough space between the two anterior portals for insertion of 8-mm cannulas. Translucent cannulas (Acufex Corp., Mansfield, Massachusetts) were used in both anterior portals to allow easy access to the joint with the instruments as well as visualization of the tack deployment through the clear plastic. A systematic diagnostic arthroscopy was performed to assess all pathologic conditions. After the capsulolabral avulsion was identified, a motorized shaver was used to debride the clot and frayed tissue along the anterior glenoid. Decortication of the glenoid rim was performed with a mechanical abrader to stimulate healing of the tissue back to the glenoid. Through the anteroinferior portal, the capsulolabral tissue was then pierced and translated superiorly along the glenoid face with the Suretac (Acufex Corp.) drill and guide pin assembly as described by Morgan and Bodenstab. 24 Occasionally, a soft tissue grasper was inserted through the anterosuperior portal to assist in the translation of the tissue. The guide pin was driven 1.8 cm into the anterior glenoid, followed by the cannulated drill under arthroscopic guidance. The tissue was then secured to the glenoid rim with the bioabsorbable tack. The tissue and the head of the tack were then probed to ensure proper tension and secure fixation. Additional tacks were then placed superiorly along the face of the glenoid to restore the anatomic position of the tissue as needed. Postoperatively, the shoulder was placed in a sling and the patient kept overnight at the hospital.
Rehabilitation
Patients in both groups underwent a therapist-supervised three-phase rehabilitation program. The first phase consisted of sling immobilization for 4 weeks with limited active range of motion. Codman's exercises 31 and isometric muscle contractions were performed with the patient under the supervision of a physical therapist. The second phase, lasting 4 weeks, consisted of progressive passive motion exercises followed by active-assisted range of motion exercises without resistance. The third 4-week phase focused on restoration of full active range of motion with progressively greater resistance exercises. Return to full active duty, contact sports, and activities requiring overhead or heavy lifting were restricted until 4 months postoperatively.
Evaluation
All patients were examined weekly during the first 8 weeks and then monthly until 6 months after their injury or surgery. The criteria used to define the treatment as a failure was either a second dislocation or symptomatic subluxation or instability preventing return to full active duty or necessitating an additional surgical stabilization procedure. The patients were examined every 6 months or contacted by telephone once they left Hawaii. The goal was a minimum of 24 months of follow-up or follow-up until failure by the established criteria, but at last evaluation some patients had been followed as long as 56 months. The evaluation consisted of the single assessment numeric evaluation (SANE) method as described by Williams et al. 32 and the L'Insalata shoulder evaluation. 22 In addition, functional status (the ability to return to the activities required of the active-duty military) and patient satisfaction information were recorded. 10 The Student's t-test was used to compare the failure rates between groups, with significance set at 0.05.
Results
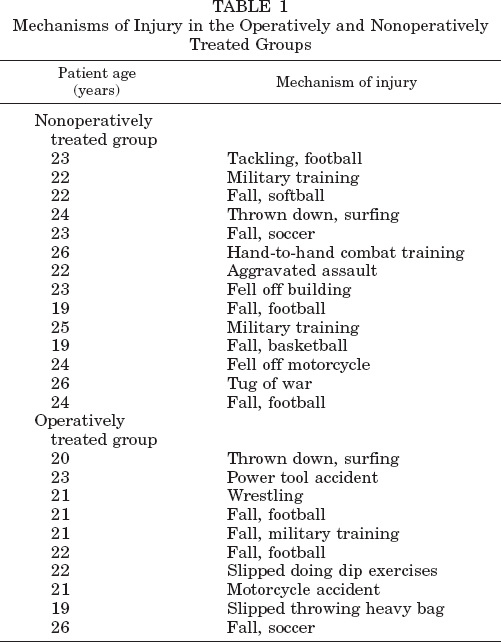
From November 1994 to April 1998, 27 patients sustained a primary anterior dislocation. Three patients were excluded, one because of a greater tuberosity fracture and two because of axillary nerve palsy, leaving 24 patients enrolled in the study. Fourteen patients were randomized to receive nonoperative treatment and 10 to receive operative treatment. All of the patients were male active-duty military personnel with an average age of 22.4 years. The average age of the nonoperatively treated patients was 23 years (range, 19 to 26), compared with 21.6 years (range, 19 to 26) in the operatively treated group. The dominant shoulder was involved in 6 of 14 (42.9%) nonoperatively treated patients and in 4 of 10 (40%) operatively treated patients. The mechanisms of injury are described in Table 1. Magnetic resonance imaging evaluations demonstrated hemarthrosis, Hill-Sachs lesions of varying size, and a capsulolabral avulsion injury (Bankart lesion) in all patients. The average follow-up was 36 months (range, 16 to 56). The average follow-up for the nonoperatively treated group was 37 months (range, 16 to 56) and for the operatively treated group was 35 months (range, 17 to 56). All patients in both groups completed the same rehabilitation program and were subsequently returned to full active duty.
Mechanisms of Injury in the Operatively and Nonoperatively Treated Groups
In the operatively treated group, examination under anesthesia revealed a 2+ load shift in eight shoulders and a 3+ in two shoulders. Hemarthrosis, a Bankart lesion, and a Hill-Sachs lesion (chondral in four patients, osteochondral in six) were identified arthroscopically in all patients. There were no capsular tears greater than 10 mm or humeral avulsions of the glenohumeral ligaments noted. In two shoulders, a small (< 10 mm) anteroinferior capsular extension was noted, indicating that the energy from the dislocation had propagated through the capsulolabral avulsion into the anteroinferior capsule. Additionally, two superior labral (SLAP) lesions were found at arthroscopy; two of these were type I and one was type III. To repair the Bankart lesions, we used two bioabsorbable tacks in nine of the patients and three tacks in one patient. There were no intraoperative complications.
Follow-up
Of the 24 patients, 3 were lost to follow-up, leaving 12 patients in the nonoperatively treated group and 9 in the operatively treated group for follow-up. In 9 of the 12 patients (75%), nonoperative treatment failed according to the established criteria, whereas in the group treated with arthroscopic repair, the repair failed in only 1 of the 9 patients (11.1%). Of the 12 nonoperatively treated patients, only 3 were followed for less than 2 years, and for 2 of these patients treatment had already failed. Six of the nine patients (66.7%) whose nonoperative treatment failed went on to have an open Bankart reconstruction. The one patient whose operative treatment failed sustained a second traumatic dislocation while playing football 14 months after his initial surgery. He has subsequently had an open Bankart reconstruction. There was no clinical evidence of reactive synovitis from the bioabsorbable tacks.
Follow-up range of motion was determined at 6 months after injury or surgery. There was no statistical difference noted in the range of motion of those shoulders treated surgically compared with those shoulders treated nonoperatively. The average loss of external rotation in the nonoperatively treated group was 3° (range, 0° to 16°). In the operatively treated group, the average loss was 4° (range, 0° to 15°).
The SANE scores averaged 57 (range, 46 to 98) for nonoperatively treated patients and 88 (range, 60 to 100) for operatively treated patients (P < 0.002). The L'Insalata scores averaged 73 (range, 46 to 92) for nonoperatively treated patients and 94 (range, 65 to 98) for operatively treated patients (P < 0.002). On the survey of patient satisfaction, the three patients who did not exhibit instability in the nonoperatively treated group rated their shoulders as excellent. All nine of the remaining patients rated their shoulders as poor after recurrence of instability. In the operatively treated group, six of nine patients rated their shoulders as excellent, two as good, and one, the patient who redislocated his shoulder, as poor.
Discussion
The rate of redislocation after an initial traumatic shoulder dislocation has varied with different reports. Over the past decade, redislocation rates after nonoperative treatment in several studies at the U.S. Military Academy at West Point have been reported to be between 80% and 92%.1, 2, 8, 30 Kirkley et al. 20 reported a redislocation rate of 47% in a randomized, prospective study of civilian patients under the age of 30 who were treated nonoperatively. The difference in reported recurrence rates is often correlated with the age of the patients at the time of the first dislocation. In a study of young Swedish hockey players, Hovelius 15 reported the recurrence rate after nonoperative treatment in players under the age of 20 to be 88% (23 of 26). Aronen and Regan 3 reported a redislocation rate of only 25% in 20 U.S. Naval Academy midshipmen treated with a supervised rehabilitation program. The group at the Naval Academy accounted for this lower rate by a well-controlled supervised rehabilitation. However, despite using a similar rehabilitation program in three previous studies at West Point, other investigators were not able to duplicate these results.1, 2, 8 We have no explanation for this discrepancy from most other reports in the literature.
The level of activity a patient resumes after an initial shoulder dislocation may determine his or her risk for reinjury. The cadets at the military academies have extraordinary demands placed on them because of their military and obligatory athletic training. According to Kirkley et al., 20 this is a potential explanation for the increased redislocation rate at West Point. They suggested that the studies performed at the military academies, although well done, are not a true representation of the general population, ostensibly because of the rigorous physical demands placed on the cadets and their more strict compliance with rehabilitation.
In this study, our patients were active-duty personnel assigned to military units in Hawaii. The average age of our patients was 2 years older than that of the cadets at the academies. Our study population consisted of active-duty soldiers and sailors with diverse athletic interests who were assigned to a variety of duties. We believe this population closely approximates a relatively athletic group within the general population who are unwilling or unable to modify demands placed on the upper extremities and the shoulder in particular.
Kirkley et al. 20 also suggested that dislocation should not be the sole criterion for failure. We strongly agree, and thus, subluxation leading to an inability to perform one's duties was also considered a criterion for failure in our study. In addition, the L'Insalata questionnaire 22 addresses the use of the shoulder both for daily activities as well as sports. Any limitations in the use of the shoulder would be reflected in lower overall scores. Our results with nonoperative treatment (75% failure rate) reflect the average for the numerous studies evaluating first-time shoulder dislocations in young patients.
A number of arthroscopic techniques used to treat patients with primary shoulder dislocations have been reported. The evolution of operative treatment at the United States Military Academy began with Wheeler et al., 30 who used an arthroscopic staple as described by Detrisac and Johnson. 9 Although this method was relatively successful, the difficulty with insertion and the potential for a displaced staple wreaking havoc on the articular cartilage led to the abandonment of this technique.2, 20 Subsequently, Arciero et al. 2 and others20, 23, 25, 30 have reported good success rates with transglenoid fixation of Bankart lesions. Medialization of the capsulolabral complex and neurovascular injuries from the posteriorly exiting sutures are some of the potential complications with this technique. The development of a polyglycolic acid (PGA) tack that could provide fixation of tissue to bone and subsequently be hydrolyzed alleviated problems with both of the previous methods. 28 The PGA tack (Suretac, Acufex Corp.) is arthroscopically inserted but has limited holding capacity compared with currently used suture anchors.4, 12 Some surgeons believe this limited fixation strength necessitates shoulder immobilization for the first 4 weeks so that the tissues can heal back to their anatomic location, thus restoring the capsulolabral buttress.1–3, 24 Burkart et al. 6 and others with anecdotal reports11, 26 have identified perioperative synovitis and shoulder stiffness and pain with use of the Suretac device. In this study, we identified no cases of synovitis or reaction to the implants, as would be manifested by increased postoperative pain or stiffness.
Conclusions
In this study we attempted to evaluate the use of an arthroscopically inserted bioabsorbable tack in young patients to repair the capsulolabral injury associated with an acute shoulder dislocation in comparison with traditional nonoperative treatment. The ability, with surgery, to reverse the natural history of this problem suggests that restoration of the capsulolabral complex back to its anatomic position can lead to normal function without instability. Our current approach is to offer young, athletic patients (< 25 years) with known high recurrence rates the option of arthroscopic repair in the acute stage after injury. On the basis of our previous work and that of others cited, we believe that this treatment is more predictable, lowers recurrence rates, and improves overall outcome.