
Abstract
Background: Upper extremity vascular injuries are uncommon in the elite throwing athlete. However, the extreme stresses that are placed on the upper extremity of elite baseball players, especially pitchers, puts them at risk for such injuries. One such injury is upper extremity venous thrombosis or “effort thrombosis.”
Purpose: We wanted to review the common initial clinical symptoms and physical examination findings of effort thrombosis in elite baseball players and to review the associated clinical conditions such as hypercoagulable states and pulmonary embolism. Study Design: Retrospective review of a series of cases.
Methods: A retrospective review of the medical records of a Major League Baseball organization and a Division I college was performed for the period 1987 to 1997.
Results: We located four cases of effort thrombosis involving elite baseball players. Contrast venography was used to confirm the diagnosis in all cases. All patients were successfully treated with transluminal catheter-directed urokinase thrombolysis followed by first rib resection and systemic anticoagulant therapy for up to 3 months. All four players returned to play at or above their previous level of competition with no long-term chronic sequelae.
Conclusions: Prompt clinical recognition, diagnosis, and treatment of effort thrombosis in the elite baseball player provides the player with an excellent prognosis for return to the previous level of play.
The extreme stresses of the repetitive overhead-throwing motion that are placed on the upper extremity of elite baseball players, especially pitchers, make these players prone to musculoskeletal overuse injuries. One such injury is thoracic outlet syndrome. 4 Thoracic outlet syndrome is associated with neurologic symptoms in more than 90% of patients. Arterial or venous symptoms have been described as the primary symptom in only 3% to 5% of patients.27,33 Venous thrombosis of the upper extremity has been termed “effort thrombosis” because of its common association with repetitive upper extremity activities.2,5,10,13 Although uncommon in the elite throwing athlete, effort thrombosis has a characteristic clinical picture that requires timely diagnosis and treatment. Previously published individual case reports offer little guidance with respect to current diagnostic and therapeutic alternatives in this select patient population. In this article we present four cases of effort thrombosis in elite baseball players and review the current literature relevant to this clinical entity.
Materials and Methods
A retrospective review of the medical records of a Major League Baseball organization and the baseball players at a Division I college was performed for the period 1987 to 1997. We identified five players with the diagnosis of vascular lesions of the upper extremity. Four of the five patients had upper extremity venous thrombosis, or effort thrombosis. 18 One patient had an acute arterial thrombosis and was not included in this review. Records of the patients’ symptoms when they first sought treatment, diagnostic evaluation, treatment, rehabilitation, and outcome were reviewed. The primary determinant of a successful outcome was asymptomatic return to competitive play at or above the level of play before the development of effort thrombosis.
Results
Two of the players were professionals at the minor league level and two were Division I college players. There were three pitchers and one catcher. Their average age was 22 years. All patients were right-handed and the dominant arm was affected in all cases. All players reported initial symptoms of arm “tiredness” or “heaviness” and a gradual onset of swelling of the upper extremity over a period of 2 to 7 days. Additional symptoms included the presence of mild discoloration of the extremity, nonspecific paresthesia, or palpable axillary cords. Characteristic findings at physical examination included venous engorgement of the arm, upper extremity swelling of several centimeters, discoloration, and palpable cords. No player had documented neurologic or arterial compromise. Diagnosis was confirmed by contrast venography (Fig. 1). Additional serologic screening for hypercoagulable states was performed. All patients had evidence of venous thrombosis of the axillary or subclavian veins in close proximity to the intersection of the clavicle and first rib. One patient had a diagnosis of pulmonary embolism and a hypercoagulable state caused by anticardiolipin antibody.
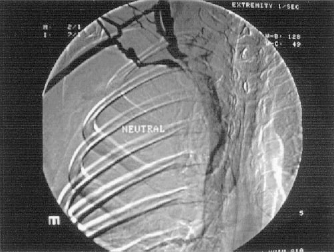
Venogram showing venous occlusion of the right upper extremity.
All patients underwent initial catheter-directed urokinase thrombolysis. After thrombolysis, each patient was treated with systemic anticoagulant therapy with heparin initially followed by warfarin sodium for 3 months. Follow-up positional venograms were obtained 1 to 3 weeks after initial thrombolysis in an effort to document continued patency of the venous system and to evaluate the thoracic outlet for an etiologic factor contributing to the thrombosis. The follow-up venogram revealed venous stenosis in one patient. The stenosis was managed with balloon venoplasty with good results. In all patients, the site of thrombosis was the thoracic outlet, with compression of the vein at the level of the first rib. No cervical ribs were noted. Three patients had complete positional occlusion of venous return with the arm in full abduction. One patient demonstrated this phenomenon bilaterally, although he was asymptomatic on the nondominant side.
All patients underwent delayed transaxillary first rib resection at intervals ranging from 1 week to 3 months after their initial clinical visit. No patient required thrombectomy. Postoperatively, patients were treated with the systemic anticoagulant warfarin sodium for 6 to 12 weeks. Rehabilitation consisted of early range of motion and strengthening exercises followed by initiation of a light tossing program at 8 weeks postoperatively. A graduated throwing program was instituted at 12 weeks postoperatively, with progression to the premorbid level of throwing intensity. All of the patients returned to competitive baseball by the next season. At a minimum of 36 months and an average 63 months’ follow-up (range, 36 to 84 months), no player had developed a recurrence of symptoms. All four players resumed play at or above their previous level of play.
Discussion
Although deep venous thrombosis is a commonly seen clinical entity, only 2% of cases are reported to involve the upper extremity. 30 Paget, 29 in 1875, and von Schroetter, 41 in 1884, were the first to describe venous thrombosis of the upper extremity. Deep venous thrombosis has classically been related to venous stasis, intimal injury, and coagulation diathesis (Virchow's triad). Upper extremity venous thrombosis may have a primary or secondary cause; patient characteristics are distinctly different depending on the etiologic type. Patients who develop primary, or effort, thrombosis are generally young, healthy, athletic men. Effort thrombosis has been described in patients involved in a wide variety of sports, including baseball, softball, 27 hockey, 9 swimming, 40 wrestling, 24 martial arts, 43 back packing, 20 and billiards. 17 Patients who develop secondary thrombosis are typically older and have concurrent systemic illness. Indwelling central venous access catheters have been reported as significant risk factors for the development of secondary thrombosis.1,8
Although the classification of deep venous thrombosis as “primary” implies that there is no known etiologic factor, compression of the venous anatomy at the thoracic outlet is believed to be a related factor. 13 The subclavian vein is bound by the anterior scalene muscle posteriorly; by the clavicle, costoclavicular ligament, and subclavius muscle anteriorly and superiorly; and by the first rib inferiorly. 27 Consequently, the vein can be compressed by any of these anatomic structures. In addition, other anatomic structures, including the pectoralis minor and subscapularis muscles, the coracocostal ligament, the prevenous phrenic nerve, osseous exostoses, cervical ribs, or any of nine types of fibrous cords can act as sites of compression.11,30,31,42 Although no cervical ribs were noted in our patients, cervical ribs have been implicated as a cause in thoracic outlet syndrome. Brown and Charlesworth, 7 in a report of their experience with cervical ribs in thoracic outlet syndrome, noted a 0.5% to 1% incidence of cervical ribs (with 50% bilaterality) in the general population. However, less than 10% of these people experience symptoms. Furthermore, when initially seen, symptomatic patients usually have arterial or neurologic rather than venous symptoms.
Wood et al. 42 have suggested hyperabduction of the shoulder resulting in compression or injury of the subclavian vein as a mechanism for the development of effort thrombosis. More recent studies by Thompson et al. 36 and Kunkel and Machleder 21 support this conclusion. The repetitive abduction and external rotation that is required of the overhead-throwing athlete is a probable contributing factor. Venographic evidence of positional occlusion was demonstrated in 21 of 25 patients in whom effort thrombosis was diagnosed in the series reported by Kunkel and Machleder. 21 Twelve of 15 patients in whom both extremities were studied exhibited this finding bilaterally. Furthermore, at the time of surgical treatment, 18 of 25 patients were found to have osseous or musculoskeletal abnormalities causing venous compression at the thoracic outlet.
Although the majority of patients who develop effort thrombosis have no predisposing systemic factors, the presence of a hypercoagulable state as a possible contributing factor to thrombosis must be considered. One patient in our series was found to have a coagulation abnormality believed to have contributed to the development of thrombosis and subsequent pulmonary embolism. Other cases of effort thrombosis and hypercoagulable states have also been described in the literature.15,32 The possibility of pulmonary embolism secondary to upper extremity thrombosis has also been described in the literature13,18,27 and, although very rare, should be considered.
Historically, patients with effort thrombosis were treated nonsurgically with bed rest, elevation of the extremity, and anticoagulation therapy with heparin and warfarin.1,2,18,27,37,38 However, reported high rates of continued disability after treatment prompted concern that more aggressive treatment might be necessary.1,38 AbuRahma et al. 1 reported that up to 73% of patients experienced chronic symptoms of upper extremity fatigue and weakness on exertion. Urschel and Razzuk 38 reported that 21 of 34 patients who were originally treated with the anticoagulants heparin and warfarin developed recurrent symptoms.
Lindblad et al., 22 in a review of their experience in Malmö, Sweden, identified 120 patients who had venographic evidence of thrombi in the axillary or subclavian vein. Seventy-three cases were classified as primary and 47 as secondary. Treatment was limited to anticoagulant therapy. Three patients with primary thrombosis had “moderate” residual complaints and 15 had “mild” residual complaints. In no case were the residual symptoms severe enough to require a change in occupation. The authors concluded that primary thrombosis was a “benign” disease and, in general, treatment with anticoagulants was sufficient.
Ameli et al. 4 attempted to evaluate the long-term effects of “conservative” management, which they defined as heparin followed by warfarin therapy for 3 months. They reviewed the cases of 20 patients with axillary vein thrombosis. Three patients developed thrombosis caused by an intravenous catheter. Seven patients developed classic effort thrombosis. In 10 patients, the cause was unknown. Three patients underwent first rib resection with no residual symptoms; the rest were treated nonoperatively. At an average follow-up of 42 months, five patients treated nonoperatively had residual minimal swelling and two had minor discomfort. Thus 7 of 17 patients (41%) treated nonoperatively had residual symptoms. The authors concluded that the nonoperative management of axillary vein thrombosis, irrespective of cause, provided a predictably good outcome and that more aggressive approaches did not appear justified.
Despite these conclusions, persistent concern over residual symptoms after upper extremity thrombosis managed by anticoagulant therapy alone prompted a search for more effective treatment. Thrombolytic therapy with streptokinase and urokinase was instituted. 12 Urokinase is the more widely used agent because of a lower incidence of side effects.30,39 Side effects with streptokinase include allergic reactions ranging from high fever to death (a 5% mortality rate has been reported); brain, liver, and lung hemorrhage; and longer required treatment times.30,39 Urokinase is considered a safe and effective treatment.1,2,12,28,34 Concurrent with the use of these thrombolytic agents, a variety of other treatments have also been recommended, including venous thrombectomy and anticoagulant therapy, 19 venous stent placement,10,14 vein reconstruction,6,25,26 low molecular weight heparin, 35 and surgical decompression of the thoracic outlet.3,5,7,21,23,36
Over the past 10 to 15 years, there have been many published reports attempting to clarify which of these treatments is the most effective. Hicken and Ameli 16 performed a literature review in an effort to determine the optimum treatment of effort thrombosis. They reported that the literature contained a wide variety of patients, treatments, follow-up, and conclusions. Their conclusion was that the optimal management of effort thrombosis remains controversial. Although anticoagulant therapy is usually the initial treatment of choice, thrombolysis and surgery are appropriate in selected cases. The authors recommended that a prospective, multicenter trial be performed.
Urschel and Razzuk 37 have reported the largest series of cases of effort thrombosis. Over a period of 50 years, thoracic outlet syndrome was diagnosed in 15,000 patients. Two hundred sixty-four of these patients developed effort thrombosis. Of these, 211 were treated with urokinase thrombolysis followed by first rib resection with excellent long-term results.
Machleder 23 studied 50 patients with the diagnosis of effort thrombosis and reported that venous patency was crucial for the prevention of recurrent or residual symptoms. Ninety-three percent of 27 patients with a patent vein after treatment were symptom-free versus only 64% of 22 patients with documented residual occlusion after treatment. Machleder reported that the most effective sequence of treatment was transluminal thrombolytic therapy followed by 3 months of anticoagulation therapy with warfarin sodium. Patients then underwent transaxillary first rib resection and decompression of the thoracic outlet. Cases of underlying stenosis were managed with balloon angioplasty. Other authors have also supported this management protocol for effort thrombosis.3,21,34,36,37
The importance of venous patency in preventing recurrent symptoms is well accepted. Sheeran et al. 34 used urokinase thrombolysis to manage 20 thromboses in 14 patients and found an immediate (without further intervention) patency rate of 93%. Adelman et al. 3 treated 17 of their 18 patients with effort thrombosis (with 82% complete thrombolysis) with urokinase. Surgical decompression, including first rib resection, was performed in 11 patients, and all 17 patients had excellent results, with no recurrent thromboses at an average 21-month follow-up. Molina 25 reviewed the experience with effort thrombosis at the University of Minnesota and suggested that effort thrombosis be treated as an emergency. He divided patients into three groups based on the nature of their symptoms. In the acute group, symptoms were of a duration less than 1 week; in the subacute group, symptoms were 1 to 2 weeks in duration; and in the chronic group, symptoms had lasted over 2 weeks. Patients in the acute group had 100% resolution of symptoms (all eight patients), whereas all of the patients in the chronic group required vein patch angioplasty to resolve the stricture caused by fibrous obliteration and scarring of the vein at the site of the thrombosis. If the stricture was less than 2 cm in length, there was 100% success, whereas if the stricture was greater than 2 cm in length, only 37.5% of the patients (three of eight) improved. This work, and a prior study by the same author, 26 provide evidence that the earlier clot dissolution can be accomplished, the more likely it is that complete venous patency can be restored and maintained with avoidance of residual symptoms.
Conclusions
Although rare, vascular injuries do occur in the elite throwing athlete. We report four cases of “effort” or “spontaneous” thrombosis in elite baseball players. This is the largest series examining this condition in such elite throwing athletes. In all cases the thrombosis was believed to be related to repeated compression of the subclavian vein secondary to the extreme abduction and external rotation that occurs during the throwing motion. A high index of suspicion should be maintained in those players who are initially seen with complaints of a “heavy” or “dead” arm and insidious onset of upper extremity swelling. Because outcomes are improved with early diagnosis and treatment, prompt clinical intervention should be instituted. Diagnostic evaluation should include contrast venography and serologic screening for a possible hypercoagulable state. On confirmation of the diagnosis, we recommend transluminal catheter-directed urokinase thrombolysis followed by systemic anticoagulation therapy and delayed first rib resection. Follow-up venography should be performed within 1 to 3 weeks of surgery. Persistent stenosis should be treated by balloon angioplasty. Early rehabilitation should be instituted with a progressive return to throwing, beginning at 12 weeks postoperatively. We believe such treatment provides the player with an excellent prognosis for return to his or her previous level of play.