
Abstract
Shoulder dislocation and subluxation occur frequently in athletes, with peaks in the second and sixth decades. The majority of traumatic dislocations are in the anterior direction. The most frequent complication of shoulder dislocation is recurrence—a complication that occurs much more often in the adolescent population. The dynamic (muscular) and static (predominantly capsuloligamentous and labral) restraints to shoulder instability are now well defined. Recent surgical procedures for shoulder instability have become less interventional and have focused on restoring disrupted static restraints. The aim of rehabilitation is to enhance the dynamic muscular and proprioceptive restraints to shoulder instability.
Epidemiology
The shoulder is a joint evolved for mobility. To some extent, the structural stability of the shoulder has been sacrificed to achieve a wide range of motion. 53 Instability is usually defined as a clinical syndrome that occurs when shoulder laxity produces symptoms.
Dislocation and subluxation of the glenohumeral joint occurs relatively frequently in athletes. Rowe 73 identified a bimodal distribution of shoulder dislocation with peaks in the second and sixth decades (Fig. 1A). In 98% of cases, the shoulder displaces anteriorly and in about 2% of cases it displaces posteriorly. 73 In young people, most dislocations are intracapsular, with capsular and labral detachments. 20 In 89% of people (35 of 39) with a first-time dislocation after age 40, a rotator cuff tear has also resulted. 56
The major cause of shoulder dislocation is traumatic injury. Ninety-six percent of shoulder dislocations result from a forceful collision, a fall on an outstretched arm, or a sudden wrenching movement. 73 About 4% of dislocations are atraumatic in origin, caused by such minor incidents as raising the arm or moving during sleep. 73 Anterior dislocation usually occurs when the arm is forcibly abducted and externally rotated. Posterior traumatic dislocation of the glenohumeral joint usually occurs when load is placed through a flexed and slightly adducted arm.
Recurrent Dislocations
An important complication of primary dislocation is recurrent dislocation. Rowe 73 suggests that about 70% of those who have already experienced dislocation can expect a recurrent dislocation within 2 years of the initial injury. In another study, 71% of all recurrences (15 of 21) were in male subjects. 52
According to Rowe, 73 young and old subjects have a comparable incidence of primary shoulder dislocation (Fig. 1A). However, the incidence of recurrent dislocation is highly age-dependent. Recurrent dislocation occurs much more frequently in adolescents than in the older population (Fig. 1B). 52 Dislocation recurs in 83% to 90% of people 20 years of age or younger, in 60% to 63% of people between ages 20 and 40, and in 10% to 16% of people 40 years of age or older. In patients with primary dislocation the mean age was 48 years, whereas in patients with recurrent dislocation the mean age was 23 years.52,73

Pathogenesis
Functional Anatomy and Biomechanics
Shoulder stability is the result of a complex interaction between static and dynamic shoulder restraints. The static restraints refer to the bony ball-and-socket configuration of the shoulder and the major soft tissues holding these bones together. The soft tissues include the capsule, the glenohumeral ligaments, and the glenoid labrum. Dynamic shoulder restraints refer to the musculotendinous units that cross the glenohumeral joint and include the rotator cuff and biceps tendon.
There is minimal bony containment of the humeral head in the glenoid cavity. This allows a wide range of shoulder movement, but, as a result, the shoulder is the most commonly dislocated joint in the body. The articular surface area of the humeral head is two to four times that of the glenoid. The diameter of the humeral head is nearly twice that of the glenoid width when measured in the transverse plane. Under normal circumstances, the shoulder capsule is relatively large and loose. The discrete thickenings or capsular ligaments of the capsule have been named the superior glenohumeral ligament, the middle glenohumeral ligament, and the inferior glenohumeral ligament complex 60 (Fig. 2). The inferior glenohumeral ligament complex has been identified as the primary static restraint against anterior, posterior, and inferior translation in cadaveric specimens when the humerus is abducted beyond 45°. 60 In the midrange of elevation, the middle glenohumeral ligament and subscapularis tendon play a minor role in assisting the inferior glenohumeral ligament complex in resisting anterior and posterior translation. 57
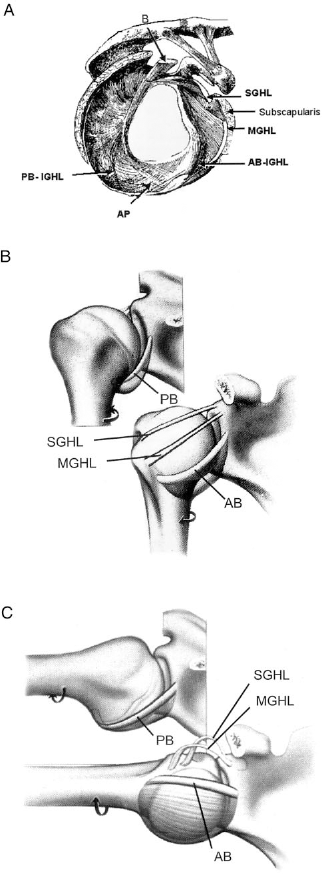
A, glenohumeral ligaments. Anatomic section of right shoulder joint with the humeral head removed. B, functional anatomy of the shoulder from the side. The inferior glenohumeral ligament complex is the primary restraint to inferior translation. (Adapted from Bowen and Warren 10 with permission.) C, functional anatomy of a 90° abducted shoulder in external rotation. With external rotation, the inferior glenohumeral ligament complex tightens around the head with the anterior band (AB) resisting anterior and posterior translation. The posterior band (PB) moves underneath the head to resist inferior translation. (Adapted from Bowen and Warren 10 with permission.) B, biceps tendon; SGHL, superior glenohumeral ligament; MGHL, middle glenohumeral ligament; IGHL, inferior glenohumeral ligament complex comprising an anterior band (AB) and posterior band (PB); AP, axillary pouch.
The labrum constitutes the fibrocartilaginous rim of the glenoid. Inferiorly, it is firmly attached to the glenoid, although it may be loose and mobile anteriorly and superiorly. The labrum contributes to shoulder stability by elevating the glenoid edge. Through this mechanism, the glenoid depth is doubled and the surface area is increased.47,84 The labrum may also act as a chock block, as evidenced by studies showing it to decrease resistance to glenohumeral translation by up to 20%.47,50 The labrum provides attachment of the glenohumeral ligaments and the biceps tendon (Fig. 2A).
A number of dynamic EMG studies have shown that the rotator cuff muscles work synergistically to create a compressive force at the glenohumeral joint during shoulder movement.11,36,41,48,65 Larger muscles crossing the glenohumeral joint (latissimus dorsi and pectoralis major) may also augment this compressive force.24,50 The biceps tendon may play a secondary role in anteroposterior stabilization, particularly with the arm in mid-elevation.24,36,65
Age-Related Changes
Collagen is the major protein of ligaments and tendons. In newborns, type III (soluble) collagen is synthesized, and the fibers formed from type III collagen are supple and elastic. With each passing decade, collagen-producing cells make less type III collagen and progressively convert to synthesizing type I collagen, which is insoluble and more stable (Fig. 3). Type I collagen has sulfur groups that have a high tendency to cross-link and form bridges between the collagen filaments, causing the fibers they compose to be relatively tough and nonelastic. This changing ratio of collagen types I and III throughout the body is so reliable that the chronologic age of a person can be determined by analyzing the type III collagen content of a skin sample. Analysis is performed according to the following equation 5 : type III collagen (in milligrams)/wet dermis (in grams) = 1.3e-Age/23.5. Thus, the higher content of stretchy type III collagen in tendons and ligaments helps account for the observation that young people who have already had a dislocated shoulder are much more prone to recurrent dislocation than are older people. Once excessively stretched, the capsule and ligaments may be too loose to provide the secure and stable shoulder support required for maximum athletic performance.
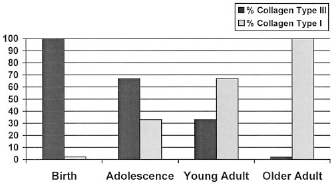
The changing ratios of collagen types III and I in soft tissues over time (based on data from Bakerman 5 ).
Traumatic Anterior Instability
There are several morphologic changes associated with glenohumeral joint instability. The most significant changes, in terms of recurrent instability, are those associated with the inferior glenohumeral ligament complex and its attachments to the labrum and humerus.
In 1906, Perthes 69 described capsulolabral avulsion at the anteroinferior glenoid rim as a cause for recurrent shoulder instability. In 1938 Bankart 6 described the anterior labral tear as the “essential lesion” in traumatic inferior instability (Fig. 4). This lesion has become known as the Bankart lesion. Rowe and Zarins 74 noted the lesion in 70% of their cases (16 of 23) of traumatic instability in which patients required surgery. Speer et al. 77 noted a minimal increase in humeral head translation after sectioning the anterior capsule just above its labral insertion. They hypothesized that plastic deformation of the capsule and inferior glenohumeral ligament complex occurred before medial detachment of the labrum. Bigliani et al. 8 have shown that an intrasubstance ligament injury occurs before labral avulsion. The glenohumeral ligament complex may avulse from its humeral attachment24,59,88 or, rarely, avulse in combination from both the humerus and the glenoid. 83
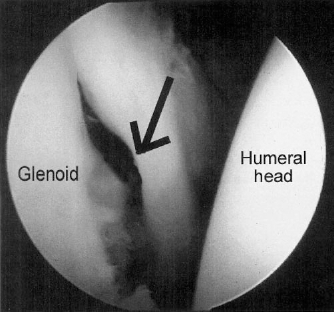
Arthroscopic image of detachment of the labrum and capsule from the anterior glenoid (Bankart lesion [arrow]) in a left shoulder.
Superior labral lesions have been associated with glenohumeral instability. Hintermann and Gachter 32 noted 7% of their patients (14 of 212) with traumatic anterior instability requiring surgery had lesions in the superior labrum. Pagnani et al. 64 showed in a cadaver study that superior labral lesions contributed to instability of the glenohumeral joint if the biceps attachment was destabilized.
The most common bony lesion associated with traumatic glenohumeral instability is a compression fracture at the posterolateral margin of the humeral head. This occurs as the humeral head impacts the glenoid edge during dislocation. This has been termed the “Hill-Sachs” lesion. 31 This lesion has been reported to occur in more than 80% of cases of traumatic instability,15,61,85 although it may be missed with standard radiographic views. To play a significant role in recurrent instability, the Hill-Sachs lesion must involve more than 30% of the proximal humeral articular surface. 75 The lesion is smaller than this in most cases of traumatic shoulder instability.75,85
Atraumatic Instability
A small group of patients dislocate or subluxate their shoulder after minimal force or by putting their arm into a certain position. Neer and Foster 58 believed the pathologic entity was a loose, redundant inferior capsule, and they introduced the term “multidirectional instability.” Multidirectional instability is less often associated with a labral detachment or Bankart lesion than other types of instability. The condition is associated with generalized ligamentous laxity in a small number of cases. 3
The definitive origin of atraumatic instability is still not clear; it may be multifactorial. Current etiologic theories include a deficiency in the interval between the subscapularis and supraspinatus tendons, suboptimal muscle control of shoulder function, and abnormalities in connective tissue. Rodeo et al. 72 analyzed the collagen and elastic fibers in the shoulder capsule of patients with unidirectional anterior instability, multidirectional instability at primary surgery, multidirectional instability at revision surgery, and patients with no history of shoulder instability. The unidirectional and the multidirectional instability groups had similar histologic results. Skin analysis between these groups demonstrated that there was a significantly smaller mean collagen fibril diameter in skin samples from the primary multidirectional instability group compared with the unidirectional anterior instability group. This suggests the possibility of an underlying connective tissue abnormality.
Impingement and Instability
Adolescent athletes are often seen with shoulder pain that is attributed to instability.1,2,24,42 These athletes usually perform activities that place the arm in the overhead position, such as are involved in volleyball, swimming, throwing, and tennis. A current hypothesis is that repetitive glenohumeral capsular overload at an extreme range of motion (especially abduction and external rotation of the shoulder) leads to gradual stretching of the anterior capsule and tightening of the posterior capsule, with a subsequent increase in humeral head translation.1,2,42 With the athlete's shoulder at an extreme range of motion or during periods of rotator cuff or periscapular muscle fatigue, this increase in humeral head translation may produce shoulder pain due to rotator cuff impingement and subsequent tendinosis.
Clinical Evaluation of Unstable Shoulders
The clinical evaluation of a shoulder, to determine its stability, is largely dependent on the patient's history. 14 It is valuable to elucidate the events surrounding any episodes of instability, the position in which symptoms are provoked, and the nature of the symptoms. It is important to be aware that only 50% of people whose shoulder subluxates can actually feel this occurring 58 and that this subtle instability can appear as a secondary impingement.38,39
The examination of a patient who has recently dislocated his or her shoulder is often difficult because of the pain evoked during the examination. We have found that unstable shoulders have more range of motion in external rotation and internal rotation, more supraspinatus muscle strength, more strength in external rotation, and lower scores for impingement than shoulders with other pathologic entities. 80
There are a number of techniques described for examining an unstable shoulder. These can be divided into tests for shoulder laxity and tests that reproduce some of the symptoms of glenohumeral joint instability.
The Sulcus Sign
The sulcus sign—a dimple created beneath the acromion when the subject's arm is translated inferiorly—is thought to be an indicator of shoulder capsular laxity. Biomechanical studies have determined that the superior glenohumeral ligament is the major ligament tested by the sulcus sign.7,9,18 When there is a sulcus sign of 2 cm or more when the arm is translated inferiorly, the likelihood of shoulder instability is high (likelihood ratio 6:1). 80
Load and Shift Test
The load and shift test is a test for shoulder laxity. Many variations of the test have been described. In our version, we position the patient supine. This involves positioning the patient so that the center of the scapula of the affected limb is on the edge of the bed, allowing a full range of movement of the humeral head while stabilizing the scapula. The patient's arm is grasped with both of the examiner's hands—one just distal to the elbow and the other just distal to the humeral head (Fig. 5A). The arm is placed in 90° of abduction and neutral rotation and the humeral head is loaded into the glenoid to ensure that it is centered. The examiner then attempts to shift the humeral head in the anterior, inferior, and posterior directions. The test is graded as illustrated in Figure 5B.
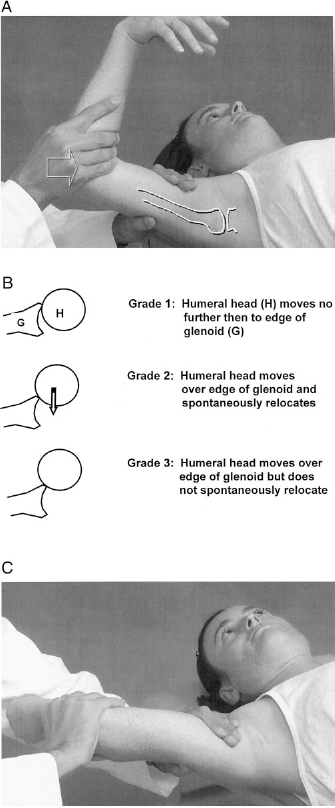
A, the load and shift test. B, method of grading the load and shift test (based on data from McFarland et al. 51 ). C, the apprehension test.
This test has a high specificity (98% to 100%) when positive; that is, it is rare for patients with stable shoulders to have a positive result (grade 2 or more) for this test in the clinic. 80 However, the test has a low sensitivity in the clinical setting (41% of subjects with unidirectional instability and 26% of subjects with multidirectional instability). 80 Levy et al. 45 recently demonstrated that this test has poor reproducibility (74% intraobserver and 78% interobserver when grade 0 and 1 are equalized). The accuracy and reproducibility of laxity testing is significantly improved when the patient is anesthetized. 43
Apprehension Test
The apprehension test 74 reproduces some of the symptoms of glenohumeral joint instability. In this test for stability, the patient is positioned as in the load and shift test. The arm is then abducted and externally rotated to 90° and then gradually further rotated and extended (Fig. 5C). A positive test occurs when the patient becomes apprehensive that his or her shoulder is going to dislocate or subluxate. Tzannes 79 found the test to have an interobserver reliability of 47%.
Relocation Test
The relocation test is another test of anterior stability. 39 To perform this test, the examiner tests the patient for apprehension and then applies a posteriorly directed force to the humeral head, which is thought to relocate it. The test is positive if the patient's symptoms are eased by the maneuver. This test has been determined by Speer et al. 78 to be most accurate when the symptom measured is apprehension alone, not pain (85% accuracy for apprehension versus 49% accuracy for pain). However, for patients whose unstable shoulder has never actually dislocated, pain is the most accurately measured symptom (84% accuracy for pain versus 48% accuracy for apprehension). It should be noted that these figures were obtained by using an anteriorly directed force to elucidate symptoms when the arm was in 90° of abduction (not maximal abduction) and external rotation.
Nonoperative Management
There are few data to support immobilization in a sling as a form of treatment for shoulder instability. In fact, a recent MRI study by Itoi et al. 37 has shown that immobilization in the traditional position of internal rotation causes more displacement of the labrum than positioning the arm in external rotation. Hovelius et al. 35 found that there was no difference in redislocation rates between patients treated with early mobilization and those treated with 3 to 4 weeks of immobilization in a sling. Furthermore, the results of nonoperative management in adolescents are particularly poor. Rowe 73 reported an 83% redislocation rate in patients under 20 years of age (82 of 99).
Management in subacute cases (3 days to 6 weeks after injury) may consist of pain control and gradual increase in range of motion exercises, starting with passive exercises and progressing to active-assisted and active exercises. Management in chronic cases (6 weeks or more after injury) may consist of strength and flexibility reconditioning. Rehabilitation should be based on the principle of progressive resistance and avoidance of aggravating factors.
Unidirectional Instability
Nonoperative management of recurrent unidirectional instability has a poor success rate. Burkhead and Rockwood 12 reported that patients in only 12 of 74 cases of recurrent unidirectional shoulder instability had good or excellent results after an exercise program. Kirkley et al. 40 found that young patients who had experienced a single episode of anterior shoulder instability and were randomized to a surgical treatment group had much better functional results than those in the nonoperative group, even when compared with patients in the nonoperative group who had not had recurrent dislocation.
Multidirectional Instability
The reported success rates for shoulder-strengthening protocols for the management of multidirectional instability are better than those reported for unidirectional instability.12,86
Surgical Management
Traumatic Unidirectional Instability
The most recent and most successful surgical procedures for unidirectional shoulder instability involve reattachment of the detached labrum and associated glenohumeral ligaments with little disruption to the length or attachment of other structures around the shoulder (Bankart repair). 68 An open Bankart repair consists of detachment and later reattachment of the humeral insertion of the subscapularis tendon and a reattachment of the labrum to the anterior glenoid with sutures through bone or with suture anchors. Most authors also reduce any capsular redundancy by imbricating the anterior capsule with sutures. Open anterior stabilization is associated with a 12° loss of external rotation of the shoulder, probably because of shortening of the subscapularis tendon after detachment and reattachment. 26
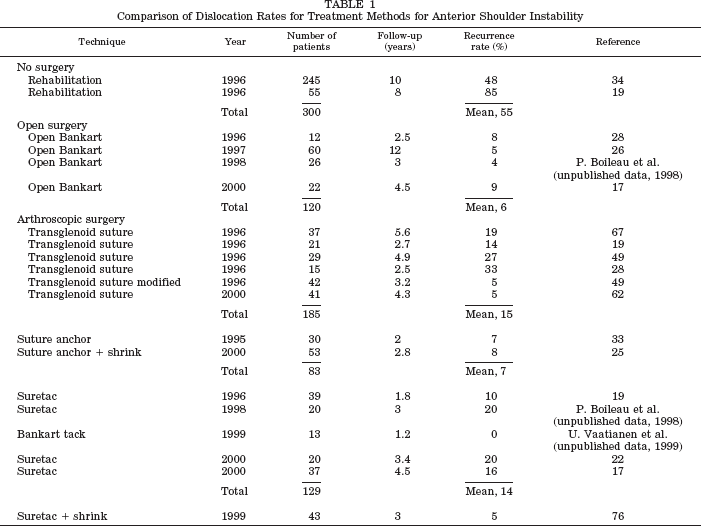
For management of unidirectional glenohumeral instability, arthroscopic techniques have been developed to reattach the labrum without an open incision and without subscapularis tendon detachment. The reported redislocation rates for arthroscopic anterior shoulder stabilization are inferior to those reported for open procedures (7% to 17% versus 5%, Table 1). However, arthroscopic procedures are associated with less loss in external rotation than are open procedures. Arthroscopic techniques for reattaching the labrum can be divided into three categories: 1) transglenoid suture technique,19,28,49,67 2) arthroscopically delivered and tied suture anchors, 33 and 3) an arthroscopically delivered biodegradable tack (for example, Suretac [Smith & Nephew, Inc., Endoscopy, Andover, Massachusetts]) (Fig. 6). A comparison of the reported rates of dislocation for each technique is made in Table 1.
Comparison of Dislocation Rates for Treatment Methods for Anterior Shoulder Instability
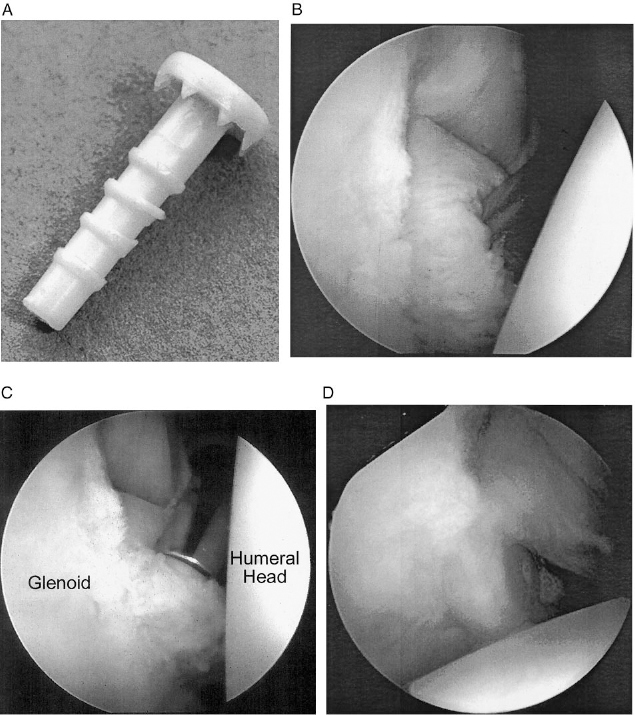
A, Suretac device for labral fixation, B, to fix the Bankart lesion (see Fig. 4), the detached labrum and capsule are captured with guidewire and drill. C, after drilling, the drill is removed and the Suretac is passed over the guidewire. D, the guidewire is removed and a second Suretac is placed to reattach the labrum and capsule.
Multidirectional Instability
Anterior Capsular Shift
The most commonly performed and most successfully reported surgical procedure for multidirectional instability of the shoulder is the anterior capsular shift, an open procedure that involves imbricating the anterior and inferior capsule.3,48,66,70 Closure of the capsular interval between the subscapularis and supraspinatus tendons has been reported to be successful in small series of patients with subluxation.23,30
Capsular Shrinkage
Thermal denaturation of collagen results in uncoupling of the triple helices and shortening of the collagen. 4 Several authors have noted a 15% to 40% reduction in length of collagenous tissue subjected to 65° to 72°C of heat81,82 (Fig. 7). They also noted an associated loss in load-to-failure properties. Arthroscopic devices have been designed to deliver heat to the shoulder capsule with the potential to “shrink” redundant capsule arthroscopically. 76 Good results have been reported with this technique in recent short-term studies of multidirectional instability 46 and internal impingement in baseball players. 44 Transient axillary nerve palsies 27 and capsular disruption 71 have been reported as complications after heating of the shoulder capsule. Further long-term evaluations are necessary to evaluate the technique, indications, and results of this novel method of reducing capsular volume.
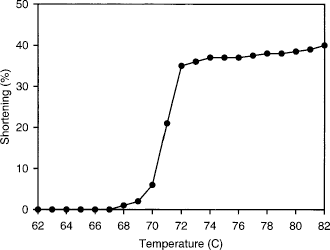
The effects of heat on shrinkage of soft tissue (data from Vangsness et al. 81 reprinted with permission).
Rehabilitation
The key to pain-free shoulder function for sporting activities is functional stability or a balance between the stabilizers of the shoulder and forces applied to the shoulder. Rehabilitation for shoulder instability, whether as nonoperative treatment or postoperative management, should aim to optimize the performance of the dynamic stabilizers.
Dynamic compression is the first mechanism thought to contribute to functional stability in the shoulder.63,87 In the transverse plane, the subscapularis muscle co-contracts with the infraspinatus and teres minor muscles to center and compress the humeral head into the deepest concavity of the glenoid fossa. In the coronal plane, the inferior fibers of the rotator cuff muscles co-contract with the anterior deltoid muscle, which again helps to keep the humeral head centered in the fossa. Weakness that affects any of these stabilizing force couples should be addressed from the outset of rehabilitation. Training for muscular endurance may be as important as regaining pure strength, because excessive humeral head translation may occur with fatigue of the dynamic stabilizers.
Dynamic ligament tension, as described by Clark and Harryman, 16 is the second mechanism thought to contribute to functional stability of the shoulder. The rotator cuff tendons blend with the shoulder capsule at their point of insertion and serve to tighten the otherwise redundant capsule on contraction. In effect, tensioning of the capsular complex helps to restrain excessive humeral head translation.
Wilk et al. 87 describe the third component to functional stability as reactive neuromuscular control. This involves exercising the unstable shoulder in positions that maximally challenge the dynamic stabilizers. Afferent information relating to joint position awareness is fed back to the central nervous system via the various mechanoreceptors that are contained within the capsulolabral structures. In situations of potential tissue damage, the afferent system effects a voluntary muscle contraction to reposition the joint and reduce mechanical stress on surrounding structures.
Plyometric exercise is one proposed method of retraining for neuromuscular control. The aim of this form of exercise is to prestretch the accelerator muscles of the upper limb via an eccentric contraction immediately before the phase of concentric return. As the target muscles lengthen (eccentric activity), energy is stored within the series elastic component of the musculotendinous unit. This “preloading” allows for enhanced power output when the same muscles contract and shorten (concentric activity) to produce the desired movement.
For anterior shoulder instability, 90° of abduction and external rotation is recognized as being a position of risk for anterior subluxation or dislocation. However, EMG studies have shown that this position allows for enhanced recruitment of the infraspinatus and teres minor muscles when compared with lower elevation ranges. At 90° of abduction, the posterior cuff has been shown to pull the humeral head posteriorly during external rotation, thus reducing the likelihood of anterior subluxation. 13 Theraband exercises (Hygenic Corporation, Akron, Ohio), or exercises that involve resistance tubing, may be a useful means of strengthening the rotator cuff, facilitating proprioceptive mechanisms, and preparing the athlete to return to sport.
To provide a stable platform under the humeral head, the scapula and humerus need to move in synchrony, and the orientation of the glenoid needs to adjust in response to changes in arm position. The trapezius and serratus anterior muscles contribute to two important force couples that produce scapular elevation and upward rotation. On the basis of EMG findings, Moseley et al. 54 advocate inclusion of four key exercises in any scapular muscle-strengthening program (rowing, scapular plane elevation, and press-up and push-up with accentuated protraction). However, all of the periscapular muscles should be assessed for length and strength, with particular emphasis on endurance training to facilitate their postural function.
Normalizing range of motion, particularly in capsular length, is an important aspect of rehabilitation. In situations of asymmetric capsular tightness, the humeral head has been shown to translate excessively in the direction opposite to the tightness. 29 In the athlete performing overhead sports, posterior capsular tightness is not an uncommon finding. 21 For this group of subjects, restoration of capsular length is crucial in prevention of or rehabilitation for anterior shoulder instability.
Conclusions
The incidence of shoulder instability in adolescent athletes is high because of their participation in activities that require the arm in the overhead position and the high type III to type I collagen ratio. Moreover, the outcome of nonoperative management for traumatic glenohumeral joint instability in the adolescent population is poor. Significant advances have been made with respect to understanding the mechanics of the shoulder joint and the important roles of the capsule and labrum. It is clear that both structures are vitally important to maintain shoulder stability. There have also been significant advances in methods to restore the malfunctioning anatomic structures in cases of both unidirectional and multidirectional shoulder instability. 55