
Abstract
Successful treatment of anterior instability of the shoulder requires a balance between restoring joint stability and minimizing loss of glenohumeral motion. The choice of treatment should be individualized on the basis of the patient's occupation and level of participation in sports, as well as on the degree of instability of the shoulder. Despite discussions to the contrary, there is no single “essential lesion,” as proposed by Bankart, that is responsible for recurrent anterior shoulder instability, although the Bankart lesion is by far the most important. The choice of operative treatment must be tailored to correct the abnormality that is identified at the time of surgery. A variety of promising arthroscopic techniques have been developed for the treatment of anterior shoulder instability; however, open stabilization remains the standard, especially for severe instabilities, revision procedures, and for athletes who participate in contact sports. This article will review the open surgical techniques used for treatment of anterior instability of the shoulder. Both current and historical operations will be discussed. Regardless of which procedure is chosen by a surgeon, the treatment should follow the guidelines taught by Rowe: anatomic dissection at the time of surgery, identification and repair of the lesions responsible for the instability, returning tissues to their anatomic locations, and early postoperative range of motion. By following these guidelines, the results of treatment of anterior instability of the shoulder can be optimized.
Glenohumeral stability is achieved by the interaction between static and dynamic forces around the shoulder. Static stability is conferred by the bony configuration of the glenohumeral joint, the fibrocartilaginous glenoid labrum, the capsule and its ligamentous thickenings, 53 and a negative intraarticular pressure. 24 Dynamic control is a result of rotator cuff 36 and scapular muscle function. 62
Glenohumeral instability exists in many forms and may be classified according to its degree, the circumstances in which it occurs, the original cause, and the direction in which the humeral head displaces. 49 Most shoulder dislocations occur in patients who are in their early 20s, with an 85% to 90% male predominance.7,75 A family history of instability is present in 25% of patients who sustain a shoulder dislocation. 70 There is no predilection for dislocation of the dominant versus nondominant shoulder. The direction of dislocation in 95% of patients is anterior.13,23 The mechanism of injury causing dislocation is a combination of abduction and external rotation in 75% of patients; other mechanisms are elevation combined with external rotation, a direct blow, and a fall on an outstretched arm. 70
The spectrum of disability after an anterior shoulder dislocation ranges from pain and apprehension when the arm is used overhead (such as in throwing or serving in tennis), to episodic subluxation to recurrent dislocations.43,74 Successful surgical treatment for anterior instability can be performed using either open or arthroscopic approaches. The purpose of this article is to present the principles and techniques of open operations for the treatment of anterior glenohumeral instability.
Normal Anatomy
Ordinarily, the humeral head is retroverted 30° in relationship to the transepicondylar axis of the humerus, and the typical neck-shaft angle is 130°. 76 The glenoid fossa arises from the lateral aspect of the scapula. Its average radius of curvature is 24 mm, which is only 2 mm less than that of the humeral head. 37 However, because less than one-third of the humeral head articulates with the glenoid during any given position of rotation, the glenohumeral articulation is minimally constrained by bony anatomy alone. The glenoid labrum is a fibrocartilaginous structure that functionally deepens the glenoid fossa, 35 serves as an anatomic restraint to humeral head translation, and provides an anchor point for the glenohumeral ligaments. Stability is conferred by a series of dynamic and static soft tissue restraints including the rotator cuff, labrum, glenohumeral ligaments, and capsule. There is dynamic interplay between the capsuloligamentous restraints during contraction of the rotator cuff, allowing a large range of motion while maintaining stability. 82
The main static restraints to glenohumeral instability are the glenohumeral ligaments. These “ligaments” are discrete capsular thickenings rather than isolated structures, as in the knee. The actual size of the glenohumeral ligaments varies significantly between persons. The ligaments work together along a spectrum of activity depending on the position of the arm, its degree of rotation, and the direction of a given applied force. 81
The superior glenohumeral ligament has been described as the primary restraint to inferior translation in the adducted shoulder, while the role of the coracohumeral ligament is less clear. 83 The superior glenohumeral ligament originates from the supraglenoid tubercle, while the coracohumeral ligament originates from the coracoid process. The two structures pass through the rotator interval, where the distinct fibers blend together and insert on the lesser tuberosity. These structures are relatively constant and are present in over 90% of shoulders. The superior glenohumeral ligament and coracohumeral ligament have a secondary role in preventing posterior translation of the humeral head when the shoulder is in flexion, adduction, and internal rotation.
The middle glenohumeral ligament is a less constant structure. It has been described as being present in 80% of shoulders. Its appearance varies from a discrete band to a sheet-like structure inserting just superior to the anterior band of the inferior glenohumeral ligament on the glenoid rim. The middle glenohumeral ligament prevents anterior translation of the humeral head with the shoulder externally rotated in a midrange of abduction (45°) in conjunction with the subscapularis muscle. 81
The inferior glenohumeral ligament complex is the main static stabilizer of the glenohumeral joint. 57 The inferior glenohumeral ligament complex has been compared to a “hammock,” with an axillary pouch and two discrete bands (anterior and posterior). The anterior band is the main static restraint to anterior translation with the arm abducted and externally rotated. The posterior band is the main restraint to posterior translation in conjunction with the posterior capsule with the arm abducted.
Pathologic Anatomy in Recurrent Instability
The pathoanatomy that can contribute to anterior shoulder instability includes Bankart lesions, bony Bankart lesions, capsular injury, excessive capsular laxity, Hill-Sachs lesions, rotator cuff and subscapularis muscle injuries, glenoid fractures, and glenoid dysplasia. Bankart lesions are found in 65% to 90% of shoulders that undergo surgery to correct anterior instability15,20,53,70,75 (Fig. 1). Hill-Sachs lesions have been found in 77% of unstable shoulders, damage to the glenoid rim including fracture in 73%,43,72 loose bodies in 14%,
20
rotator cuff tears in 13%, posterior glenoid labral tears in 10%,
15
and glenoid avulsion fractures in 4%. If a glenoid fossa fracture involves greater than one-third the diameter of the glenoid, it should be repaired.
Typical pathologic findings in a shoulder that is unstable anteriorly, a Bankart lesion (with or without a fracture of the anterior glenoid rim) and a Hill-Sachs lesion. The anterior capsule can be overstretched in the absence of a Bankart lesion.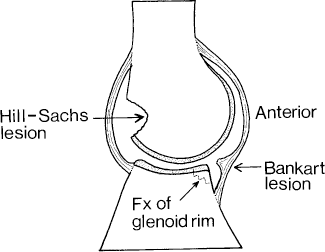
The anterior shoulder capsule and glenoid labrum are commonly avulsed from the anterior glenoid rim in patients who have had a shoulder dislocation (the Bankart lesion). 9 Bankart 8 noted that “To anyone who has seen this typical lesion exposed at operation it must be obvious that the only rational treatment is to reattach the fibrous capsule to the glenoid ligament whence it was torn.” In describing how to reattach the avulsed capsule, he stated that “It should be remembered that the capsule of the shoulder joint is normally a lax, and not a tense, structure,” 8 reinforcing the principle of anatomic repair.
A redundant capsule and deficient subscapularis muscle can also contribute to shoulder instability. 72 These findings are somewhat subjective and can be subtle. The presence of these lesions is best assessed through an open approach. 19 The exact role that capsular stretching may play in causing an unstable shoulder is the subject of much discussion. Repetitive stress from the throwing motion may lead to stretching of the capsule without causing a Bankart lesion. 93 In one series, 74 18 of 50 patients who had transient subluxation did not have Bankart lesions. Bigliani et al. 12 and Speer et al. 78 have performed studies suggesting that capsular stretching coexists with Bankart lesions and that the capsule must be stretched to allow the humeral head to dislocate.
Rowe and Zarins
74
first described a large opening in the interval between the anterior border of the supraspinatus tendon and the upper border of the subscapularis tendon 3(“rotator interval” or “seam”) as contributing to anterior instability of the shoulder (Fig. 2). It has been reported that an enlarged rotator cuff interval can be the primary abnormality in some patients who have anterior shoulder instability and have undergone isolated rotator cuff interval closure to correct anterior shoulder instability.
17
A tear of the rotator cuff interval should be repaired when found; however, care should be taken not to overtighten the interval to prevent postoperative loss of shoulder motion.
97
A, a lesion that is commonly seen in shoulders that are unstable in an anterior direction is an enlargement of the interval (seam) between the anterior border of the supraspinatus tendon and the superior border of the subscapularis tendon. B, after closing the interval, check the rotation to ensure that the joint is not overconstrained.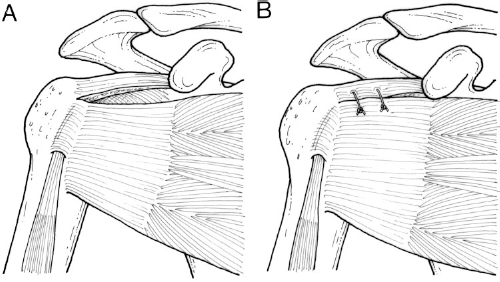
Effect of Age
The age of a patient at the time of initial dislocation plays a role in the tissues that are disrupted. In patients older than 40 years, there is a high incidence of rotator cuff tears associated with dislocations. 55 Younger patients may have more glenoid labral disruptions, whereas older patients may have primarily capsular disruptions. 7 Younger patients also have a higher incidence of osteochondral loose bodies and may have a lower prevalence of Bankart lesions. 20
Imaging
Studying preoperative radiographs may serve to alert the surgeon to the presence of associated abnormalities. 58 An AP view in internal rotation and a Stryker notch view are useful to demonstrate Hill-Sachs lesions, whereas osseous Bankart lesions are better seen on a West Point view. The use of MRI is helpful in identifying labral abnormalities and subscapularis muscle tears while highlighting secondary signs of instability such as small Hill-Sachs impaction fractures or small anteroinferior glenoid rim injuries.
Nonoperative Management
If a dislocation has occurred, a brief period of immobilization is recommended after reduction to reduce symptoms. Despite a report to the contrary, 58 it has not been proven that immobilizing a shoulder for 3 or 4 weeks after initial dislocation results in a lower redislocation rate compared with allowing early range of motion after injury.31,32 Initial therapy should aim to restore a painless full range of motion. Then, rotator cuff and periscapular muscle strengthening exercises are prescribed.
Many patients who dislocate their shoulders do well in the short term. However, long-term success rates have been reported to be as low as 18% for patients who dislocate their shoulders for the first time, and 9% in patients who have had prior dislocations. 13 Age is a significant factor in patients with shoulder instability. Rowe 70 reported a 100% redislocation rate in patients who were under 10 years old at the time of initial dislocation, 94% for patients who were between 10 and 20 years old, 79% for patients between 20 and 30 years old, and 50% for patients who were between 30 and 40 years old. The activity level of the patient also plays a role in shoulder instability. One study reported that 87% of athletes develop recurrent instability, compared with 30% of patients who are not athletes. 77
The success of nonoperative management requires avoidance of situations in which the arm is put at risk of dislocating (such as overhead abduction and external rotation for anterior instability). Rotational and scapular muscle strengthening exercises should be performed. Harnesses that limit the arm from going into extreme external rotation while abducted are useful in special circumstances.
Indications for Surgery
The following types of situations are usual indications for surgery: 1) initial dislocation in a patient who participates in high-risk or high-demand activities in whom recurrent dislocation would be inopportune or dangerous (for example, professional athletes, mountain climbers, certain types of construction workers), 2) recurrence of dislocation or subluxation after trauma treated adequately with nonoperative measures, and 3) pain due to recurrent transient shoulder subluxation when the arm is used for overhead activities.
Patients who have symptoms of shoulder instability after a prior shoulder dislocation do not always have obvious signs of instability when returning for examination. Recurrent transient subluxation of the shoulder may be the cause. The so-called “dead-arm syndrome” was described by Rowe and Zarins 74 and is characterized by a sudden sharp or paralyzing pain when the shoulder is moved quickly into a position of maximum external rotation in abduction and elevation, or when the shoulder is subjected to a direct blow. Half of patients who have transient shoulder subluxation are unaware that one shoulder is slipping out of joint. 74 This syndrome is common in athletes who use the overhead motion to throw, swim, or serve in tennis, and in patients who work with their arms in an overhead position. 93
First-Time Dislocation
Management of a patient with a first-time dislocation of the shoulder as the result of trauma remains controversial. 28 Treatment options range from prolonged immobilization in a sling 88 to early range of motion5,30 to immediate surgical stabilization.4,50 Factors such as the patient's age, the force of trauma that caused the dislocation, the absence or presence of generalized ligamentous laxity, the sport in which the patient participates and the level of participation, and the timing during an athletic season all must be considered. There is a high co-morbidity of rotator cuff tears and greater tuberosity fractures in patients older than 40 years. 32 The presence of a torn rotator cuff would be a strong indication for initial repair after a shoulder dislocation. Patients in whom minor trauma caused the initial dislocation have a higher rate of recurrent instability compared with those patients whose initial dislocation was major trauma. 71 However, results of surgical repair of atraumatic recurrent instability are not as good as repair for instability caused by trauma.
A recent study reported lower recurrence rates and good function in patients who were treated surgically after initial shoulder dislocation. 4 Although controversial, performing surgery after an initial episode of shoulder dislocation is becoming increasingly popular as arthroscopic surgical techniques improve.
Nonanatomic Repairs
In the past, a variety of nonanatomic repairs have been described for the treatment of anterior glenohumeral instability, some of which reported good short-term results. We believe that there are infrequent indications for using these procedures except in revision surgery. However, some of these operations are still popular.
The Bristow procedure was first proposed by Latarjet 41 and later popularized by Helfet in 1958. 29 In this procedure, the coracoid process is divided with an osteotome. Together with its attached tendons, the coracoid is transferred to the anteroinferior glenoid rim. The coracoid process is secured to the glenoid rim with a screw through a split in the subscapularis tendon. The goal of the Bristow procedure is to achieve stability by creating a sling effect or by making a bone block. 51 Studies have reported recurrence rates as low as 2% to 6%,10,33 but as high as 33.5%.22,61 However, the Bristow procedure causes a loss of external rotation up to 23°, 80 shortens the subscapularis tendon and muscle, and decreases internal rotation of the shoulder. Athletes who are involved in sports that require overhead use of their arms are typically unable to return to high-performance levels, especially to throwing, because of the alteration of normal anatomy.44,63
Studies have documented numerous complications after the Bristow procedure, including recurrent painful anterior instability, articular cartilage damage, nonunion of the coracoid bone block, loosening and migration of hardware, 98 neurovascular injury (especially musculocutaneous nerve), and posterior instability. 89 Revision of a failed Bristow procedure is also very difficult because of the significant scarring that occurs. The Bristow technique results in an average loss of motion of 11° of external rotation and an inability to return to the activity level that was possible before surgery. 29
The Putti-Platt procedure was first described by Osmond-Clarke in 1948. 60 Unlike the Bankart procedure, the Putti-Platt procedure does not attempt to correct the underlying pathologic lesions. However, the operation is much easier to perform than a Bankart procedure, making it more attractive. 67 In the Putti-Platt procedure, a vertical incision is made in the subscapularis tendon and capsule. The tendon and capsule are then significantly shortened by overlapping them in a “pants-over-vest” fashion. The Bankart lesion, if present, is not repaired. Although technically simpler than the Bankart procedure, and generally successful in stabilizing the shoulder, the Putti-Platt procedure results in complications such as limitation of external rotation and degenerative arthritis. 46 Furthermore, patients are unable to return to competitive throwing after a Putti-Platt procedure. 67 Recurrence rates range from 1.2% 42 to 19%, 34 whereas the loss of external rotation ranges from 6° to 29°. 18
The Magnuson-Stack procedure was first described in 1943. 47 In this operation, the subscapularis tendon is detached from its insertion on the lesser tuberosity and transferred laterally to the greater tuberosity. The procedure, like the Putti-Platt procedure, is designed to restrict external rotation without correcting any underlying lesion that causes shoulder instability. Recurrence rates range from 2% 39 to 17%, 52 whereas loss of external rotation ranges from 10° to 30°.39,52 The Nicola and Magnuson-Stack techniques not only result in loss of motion, but they result in glenohumeral arthritis and muscle weakness as well.45,47,56
Restoring normal anatomy is the guiding principle in surgery to correct anterior shoulder instability. If a Bankart lesion is present, it should be repaired and tissues returned to their correct locations. Failure to repair a Bankart lesion is the major cause of failure if nonanatomic repairs have been employed. 75
Anatomic Repairs
In the normal shoulder, no single structure is responsible for stability in all ranges of glenohumeral motion.26,72 Careful preoperative and intraoperative evaluations are necessary to ensure that all pathologic lesions are identified.
Rather than performing a favorite operation, it seems prudent for the surgeon to use an approach that corrects any abnormalities that can be identified, either on preoperative imaging or at the time of surgery. By doing so, surgical procedures for anterior instability are tailored to treat the specific abnormality confronted at surgery.55,58 If the labrum has been detached, it is reattached to the anterior glenoid rim. If the capsule has been stripped off the glenoid neck, the capsule is reattached to the bony glenoid rim. 28 The capsule can be reattached to the glenoid rim even in the presence of a fracture of the rim up to one-third of the glenoid fossa. If greater than one-third of the glenoid fossa is involved, a bone block procedure such as a Bristow or iliac crest bone graft may be considered, although this is rarely necessary. 58
Examination of the shoulder under anesthesia before operating is important to determine the degree of laxity. The opposite shoulder is always examined for comparison. Assessment of laxity is important to help determine the need for a capsulorrhaphy and to diagnose multidirectional instability.
The surgical approach must give enough exposure to allow full inspection of injured tissues and performance of corrective procedures. 26 The joint should be explored both visually and by direct probing. 28
Surgical Approach
The deltopectoral approach is routinely used for the open treatment of anterior glenohumeral instability, regardless of the procedure that will be performed. An incision is made in the anterior axillary fold for a distance of 5 cm. If cosmesis is of particular concern, the incision can be made closer to the axilla. The deep fascia is exposed and the deltopectoral groove is identified. The cephalic vein is mobilized laterally with the deltoid muscle. Retraction of the vein medially carries the risk of injuring the large veins that drain the deltoid muscle. The pectoralis major muscle is retracted medially together with the conjoined tendon. Medial retraction protects the musculocutaneous nerve. Care is taken to preserve a small part of the coracobrachialis muscle that lies lateral to the tendinous portion of the conjoined tendon and to retract it medially with the conjoined tendon. The shoulder should be inspected for a torn rotator cuff interval. 75 This enlarged seam should be partially repaired when found. The arm is then externally rotated to identify the subscapularis muscle and tendon. This is performed with the arm in adduction to protect the axillary nerve.
Incision of the Subscapularis Tendon and Capsule
There are several ways to divide the subscapularis tendon (Fig. 3). A vertical tenotomy can be made 2 cm medial to the lesser tuberosity (Fig. 3A). The entire subscapularis tendon is then carefully elevated from the anterior capsule, ligating the vessels at its inferior border.
72
This technique was preferred by Rowe et al.
72
because it allows the best visualization of the glenohumeral joint. Rather than elevating the entire subscapularis tendon, Rockwood has recommended dissecting off the superior 75%, but leaving the inferior 25% of the subscapularis tendon intact, creating an L-shaped incision.
48
This approach protects the anterior circumflex humeral vessels and axillary nerve and may minimize the risk of overconstraining the joint at the time of tendon closure (Fig. 3B). The subscapularis tendon and muscle can also be divided transversely in line with its fibers (Fig. 3C).
96
Visualization of the glenoid rim is more difficult, but motion is less restricted postoperatively. This approach may be useful in athletes who throw, in whom any restriction in external rotation postoperatively should be avoided.
Several ways to divide the subscapularis tendon are a vertical tenotomy (A), an L-shaped incision (B), or a transverse incision (C).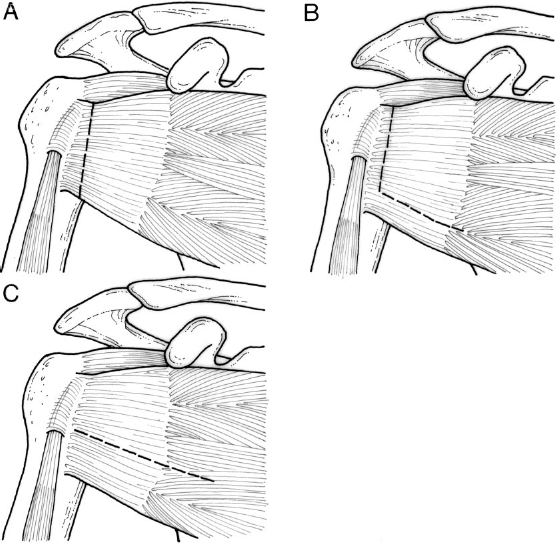
Rowe et al. 72 recommended incising the subscapularis tendon and muscle vertically and sharply dissecting them from the capsule. The capsule is divided vertically 5 mm lateral to the glenoid rim. A coracoid osteotomy is optional and gives greater exposure.
Thomas and Matsen
79
incised both the subscapularis tendon and capsule in a vertical fashion just medial to the bicipital groove (Fig. 4). The capsule and labrum are repaired to the glenoid rim from inside the joint. Advantages of this approach are reported to be technical facility, the ability to tailor the amount of desired tension on closure, and the avoidance of scarring between the subscapularis tendon and capsule. Disadvantages include the inability to judge or modify the degree of capsular laxity and the risk of subscapularis tendon and capsule disruption after repair.
The subscapularis tendon and anterior capsule can be divided together 1 cm medial to the biceps groove. The capsule and labrum are then repaired to the glenoid from inside the joint (an “inside-out repair”).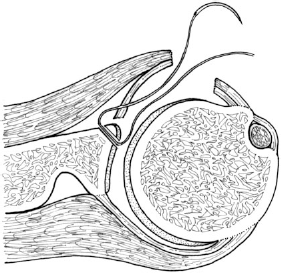
In the anterior capsulolabral reconstruction described by Jobe et al., 38 which is actually a Bankart procedure, a subscapularis muscle-splitting approach is used to gain access to the underlying capsule. A transverse capsulotomy is made in line with the split subscapularis muscle between the upper two-thirds and the lower one-third of the subscapularis tendon. The capsulotomy is extended medially to the labrum and glenoid neck at approximately the 4-o'clock position in a right shoulder. Repair of a Bankart lesion is performed using suture anchors. The capsule is subperiostally elevated superiorly and inferiorly along the glenoid neck.
After the capsule has been exposed, there are several ways to incise the capsule: vertically, “T-shaped,” or transversely (Fig. 5). The top of the T can be based either near the glenoid rim or laterally near the humeral head.
Several ways to incise the capsule are a vertical incision 0.5 cm lateral to the glenoid rim (A), a T-shaped incision (B), or a transverse incision (C).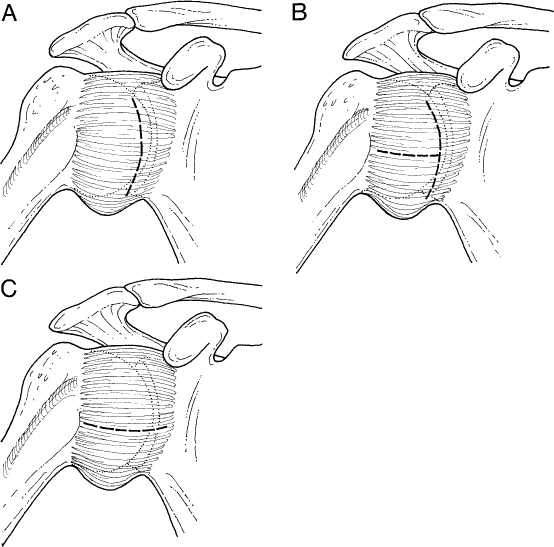
Zarins and colleagues93,96 have described a method of incising the capsule in athletes who throw, in whom it is imperative to maintain a full range of external rotation after surgery. A transverse capsular incision is made. The incision is extended medially across the glenoid rim and onto the neck of the glenoid. The flaps of the capsule are retracted superiorly and inferiorly for exposure to allow the placement of holes or anchors in the glenoid rim. The sutures are passed through the capsule without advancing the capsule medially. The flaps of the capsule can be overlapped by pulling the inferior flap upward and the superior flap downward during closure. This technique will give sufficient exposure only if the capsule has been stripped from the glenoid neck, as seen in a shoulder that has a Bankart lesion.
Andrews and Satterwhite
2
described an “anatomical capsular shift” that splits the subscapularis tendon in its middle third (Fig. 6). The capsule is incised close to the humerus beginning on the anatomic neck of the humerus at the superior corner of the middle glenohumeral ligament attachment and extending inferiorly. The inferior limit of the dissection is determined by the severity of the instability as well as the presence of any multidirectional component. A Bankart repair can be performed by reflecting the capsule medially. The humerus is prepared for reattachment of the capsule by debriding the site of the capsulotomy down to bleeding bone and placing three or four suture anchors.
The capsular shift method of incising the capsule close to the humerus. A Bankart lesion is repaired medially and the capsule is reattached.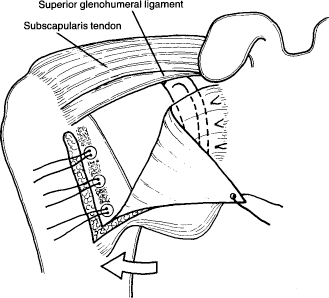
Bankart Repair
In the Bankart repair20,72,90–92 and its variations, avulsed capsule is sutured back to the glenoid rim. We believe that the Bankart procedure is the best open surgical procedure for traumatic anterior instability of the shoulder because it corrects the most common defect in traumatic anterior instability, the Bankart lesion.
Several techniques have been described to reattach an avulsed capsule to the glenoid rim. In one method, stay sutures are placed in each corner of the capsule and the subscapularis tendon, which have been divided. 96 The labrum and medial flap of the capsule are retracted medially and the anterior glenoid rim is scraped. Three suture anchors (or drill holes) are placed in the anterior rim of the glenoid at approximately the 2-, 4-, and 6-o'clock positions in the right shoulder, and the 6-, 8-, and 10-o'clock positions in the left shoulder. 43
The use of curved awls or drills to make holes through the glenoid rim is technically demanding, but it gives the strongest repair, in our experience. Heavy nonabsorbable sutures are routinely used to reattach the avulsed capsule to the glenoid rim.
Transglenoid sutures have been used to avoid complications such as fracture of the glenoid rim. 64 DuToit and Roux 16 used metal staples to repair the labrum, but they reported an unacceptable incidence of fixation failure. Complications included recurrence of instability, staple migration, penetration of articular cartilage, and hardware loosening. 59
Suture anchors are commonly used to secure the sutures to the glenoid rim. Anchors are easy to use and allow the soft tissue repair to be placed precisely on the apex of the glenoid rim, or even on the articular surface itself, to re-create the “bumper effect” of the glenoid labrum. The pull-out strength of suture anchors has been studied. Double-barbed suture anchors can withstand a force of 90 N, compared with 98 N for sutures through drill holes.86,87 The main disadvantages of anchors are 1) their potential for pulling out and becoming loose inside the joint, 2) there may be less surface area of contact between the capsule and glenoid rim when anchors are used instead of drill holes, and 3) it can be difficult to place an anchor safely at the 6-o'clock position.
In the Bankart repair, the capsule is attached to the glenoid rim by using the sutures that have already been placed (Fig. 7). Mattress sutures are not necessary because simple sutures have adequate strength for the repair. The capsule can be imbricated or overlapped if excessive capsular laxity is present. The goal for immediate postoperative motion is approximately half the external rotation as the opposite side.
Reattachment of the capsule to the glenoid rim. The amount of capsule that is overlapped at the middle suture depends on the amount of capsular redundancy that is present.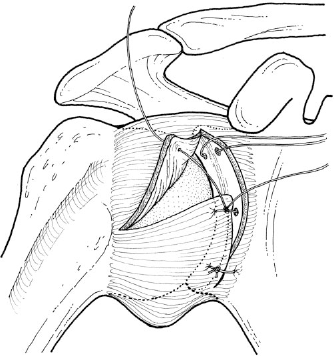
Although the presence of a large Hill-Sachs lesion doubles the recurrence rate after Bankart repair (from 3% to 6%), 20 it is almost never necessary to fill in the defect with a bone graft, perform a rotational osteotomy, or transplant the infraspinatus tendon into the defect. 58 Excessive capsular plication is also seldom necessary, although it would prevent engagement of the bony defect on the glenoid rim.
If a Bankart lesion is not found at the time of surgery, a modified Bankart repair (that is, a capsulorrhaphy) can be performed
96
(Fig. 8). If the anterior capsule and labrum have not been avulsed from the glenoid rim, the sutures may be passed through the labrum itself instead of through bone.
92
The amount of capsular plication that needs to be created depends on the degree of translation that is found when the shoulder is examined under anesthesia, the amount of tissue damage that is found, the size of the Bankart lesion present, and the sport or work that the patient will perform after surgery. However, care should be taken to avoid overtightening the capsule.
In the absence of a true Bankart lesion, a capsulorrhaphy can be performed. The suture is passed through the labrum instead of through the anterior glenoid rim.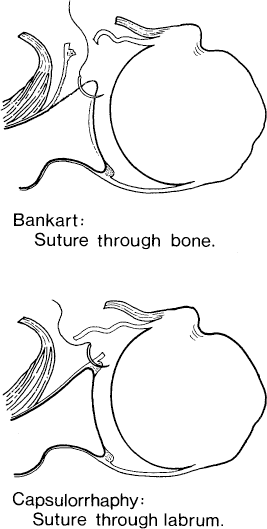
Modifications to the Bankart Repair
Modifications of the classic Bankart technique have been developed to gain stability without compromising motion. They have resulted in varying degrees of success.19,79,86,95 All include the basic premise of repairing the detached capsule back to the anterior glenoid rim. The labrum itself is rarely a factor in the Bankart repair since the capsule is incised just lateral to the labrum and the capsule itself is reattached to the glenoid rim. The labrum is often used as an overlap to reinforce the repair. 20
Bigliani et al. 11 combined a capsular shift with a Bankart repair. Gill et al. 20 described a “swing stitch” used to imbricate any inferior redundancy, shifting the capsule superiorly.
The manner in which the capsule is cut and repaired is the aspect of the Bankart repair that is most commonly modified. Altcheck et al. 1 described a technique in which a T-shaped incision is made in the capsule medially and the inferior flap of the capsule is shifted superiorly. The average loss of external rotation was reported to be 5°, and 95% of patients had satisfactory results. However, athletes who throw were unable to throw a ball with as much speed after the operation as before.
Warner et al. 84 prefer a modified Bankart repair. The inferior capsule is shifted superiorly while the arm is held in a position of abduction and external rotation. The superior flap of capsule is shifted inferiorly while the arm is held in a position of adduction and internal rotation. In this way, full postoperative motion can be regained.
The surgeon should not deliberately shorten the shoulder capsule or otherwise restrict external rotation of the shoulder as a means of preventing the shoulder from dislocating again. To prevent excessive loss of rotation after a Bankart repair, the shoulder should be externally rotated completely before the vertical incision is made in the capsule. The capsule is incised 5 mm lateral to the glenoid rim in most instances. 72 In keeping with the principle of anatomic correction, the subscapularis tendon is not advanced laterally and is imbricated on closure. 72
Capsular Shifts
If anterior capsular redundancy is the primary lesion causing the instability, the capsule can be imbricated or “shifted.” The shift can be performed laterally, especially if no Bankart lesion is present, 54 or medially in conjunction with a Bankart repair.84,95
Neer and Foster 54 described the inferior capsular shift in 1980 as a means of decreasing capsular redundancy. A laterally based T-shaped incision is made in the glenohumeral capsule, the inferior flap of which is shifted superiorly and laterally and then reinforced with the superior capsular flap.
In the anatomic capsular shift described by Andrews and Satterwhite, 2 the arm is held in 60° to 90° of scapular abduction and 45° to 60° of external rotation while the capsule is pulled superiorly and its lateral edge is secured to the humerus by using the previously placed suture anchors (Fig. 6). Careful attention is paid to limiting the amount of lateral advancement of the capsule. The rotator interval is also repaired if it is found enlarged.
Thomas and Matsen 79 repair the lateral capsular flap directly to the humerus without reefing. Warren 85 advances the inferior capsular flap only if there is preoperative inferior subluxation.
No matter what operative approach is used, the surgeon's experience and familiarity with the procedure will play a large role in the results that are obtained.
Rehabilitation
The postoperative rehabilitation program that should be prescribed depends on the type of repair that has been done, its strength, and the individual patient's requirements. In general, passive elevation to 90° and external rotation to 0° are allowed in the immediate postoperative period. If the repair is strong, a sling is not needed after the 1st day except to protect the shoulder from unexpected motions, such as while sleeping or being in a crowd. Full elevation, full internal rotation, and gradually increasing external rotation with terminal stretching are allowed at 4 to 6 weeks, at which time resistive exercises using elastic bands are initiated. Regaining external rotation requires careful attention. The goal is to achieve 50% of the external rotation of the contralateral extremity by 6 weeks, and full external rotation by 12 weeks after surgery. Full range of motion and strength should be achieved by 12 weeks postoperatively. For the athlete who throws, it is desirable to regain full motion earlier than previously described (R. J. Hawkins, unpublished data, 1998).
Contact sports are allowed at 4 to 6 months, and throwing is permitted at 6 to 9 months. For each patient, the criteria for allowing return to activity are full, pain-free motion, no apprehension when the arm is in a position of abduction and external rotation, and full strength.
Results of the Bankart Repair
At a mean follow-up of 12 years after Bankart repair, Gill et al. 20 reported that 52 of 56 shoulders had good or excellent results; 55 patients had returned to their preoperative occupation and 3 had a recurrent dislocation more than 3 years postoperatively due to a new trauma. Fifty-four patients said that they would have a Bankart procedure again for the same problem. Rowe et al. 72 reported 97% good or excellent results and 3% poor results in 145 patients. Sixty-nine percent had full range of motion, and only 2% had redislocations. If a large Hill-Sachs lesion was present, 6% redislocated.
There is currently a lack of consensus on how best to evaluate the results of surgery done for shoulder instability. Patient-derived outcome systems are available. 20 Other scores used have been derived from Rowe et al. 72 and the American Shoulder and Elbow surgeons. 65
Several generalizations can be made regarding patient views with respect to outcomes. Patients prefer a more loose shoulder with full motion rather than a shoulder that has restricted motion. 20 This should be considered if an overlap capsulorrhaphy or a capsular shift procedure is performed in addition to a Bankart repair. There is a direct correlation between the range of motion obtained after a Bankart repair and the clinical outcome. Rehabilitation is also very important, with most patients stating that they wished they had worked harder on their exercises during the initial postoperative periods. 20
Complications of Operations for Recurrent Instability
Complications may occur during surgery for anterior instability.21,26 Such complications include recurrent instability, neurovascular injury, limitation of motion, and problems from retained hardware. The most common causes of failure of surgery for anterior shoulder instability are persisting or renewed instability, postoperative pain, and restricted shoulder motion. 26
Recurrent Instability
Persistent instability after an anterior shoulder stabilization procedure can be the result of new trauma after an adequate repair for the correct diagnosis, a minor trauma after an inadequate repair for the correct diagnosis, or a procedure performed for the incorrect diagnosis (such as an anterior repair done in the presence of an undiagnosed posterior instability). Pathologic findings that are found when reoperating shoulders for recurrent instability include a new Bankart lesion, an attenuated capsule, a scarred subscapularis muscle that is dysfunctional, a wide rotator cuff interval, or a large Hill-Sachs lesion.6,25,52,75
Recurrent instability after anterior stabilization of the shoulder occurs in 0% to 11% of patients. 10 The most common causes for failure are 1) continued presence of an avulsed anterior capsule and labrum from the glenoid rim (unrepaired Bankart lesion), 26 2) excessive capsular laxity, 75 3) an enlarged “rotator interval,” 74 and 4) failure to diagnose the correct direction(s) of instability. Other causes include the presence of a Hill-Sachs lesion, 75 reduced humeral head retroversion, 40 excessive glenoid cavity retroversion, 97 avulsion of the anterior capsule from its lateral humeral attachment, 6 and a scarred or weakened subscapularis muscle or tendon.
Specific guidelines for treatment to correct recurrent anterior shoulder instability after prior treatment have previously been reported by Zarins and Kolettis 94 and Gill et al. 21 At revision surgery, if the capsule is found to be deficient, a Putti-Platt procedure can be performed. 69 If a fracture of the glenoid rim involves less than 25% of the glenoid surface, a standard Bankart repair should be performed, repairing the avulsed capsule to the remaining rim. 97 Fracture of the glenoid rim does not appear to increase the risk of recurrence, whereas a moderate-to-severe Hill-Sachs lesion increases the risk of failure. 72 If the fracture of the glenoid rim involves more than 25% of the fossa, a Bristow procedure may be indicated. 94 If the shoulder has a large Hill-Sachs lesion, surgical options include overtightening the anterior capsule to prevent external rotation. However, this carries the risk of causing posterior humeral subluxation. Another alternative is transfer of the greater tuberosity and the attached infraspinatus into the humeral head defect (Connolly procedure). 14 This procedure is effective in restoring stability, but causes loss of motion. A rotational proximal humeral osteotomy or Eden-Hybinette type of anterior bone block technique can also be used.
Revision Bankart procedures are usually successful in restoring shoulder stability. Rowe et al. 75 reported successful results in 22 of 24 shoulders (92%) that were treated with revision Bankart procedures. No degenerative changes were noted intraoperatively at the time of revision surgery. The prognosis after reoperation for involuntary instability is much better than that for voluntary instability.73,97 The ultimate treatment for failed surgery to treat instability is arthrodesis. 94
In addition to recurrent instability, other complications of surgery for anterior instability include loss of motion, 26 hardware failure,26,98 neurovascular injury,3,10 degenerative joint disease,3,15,68 and weakness. 97 Persisting postoperative pain can be the result of impingement of the greater tuberosity against the acromion process, osteoarthritis, hardware, arthrofibrosis, or subluxation. Restricted motion is usually due to an excessively tight anterior repair. Loss of motion is commonly due to a vertical capsulotomy that was made too far lateral to the glenoid rim. 92 Excessively tight repairs alter the biomechanics of the shoulder joint and lead to joint degeneration, typically long after surgery (up to 13 years).26,27 Excessive overlapping of a T-shaped capsular incision in an inferosuperior direction can also limit motion. Passive range of motion exercises should be initiated immediately after surgery to minimize arthrofibrosis.
The musculocutaneous nerve is at risk from excessive retraction of the conjoined tendon at the time of surgery. The axillary nerve can be injured while dissecting below the inferior border of the subscapularis tendon, or when placing sutures into the inferior capsule at the 6-o'clock position.
Conclusions
Successful treatment of anterior instability of the shoulder is achieving a balance between the restoration of joint stability while minimizing loss of glenohumeral motion. The choice of treatment should be individualized on the basis of the patient's occupation and level of participation in sports, as well as on the degree of instability of the shoulder. In 1923, Bankart 8 stated that surgeons concentrated on stability alone, selecting the simplest procedure that achieves stability with the lowest recurrence rate. These procedures include the Magnuson-Stack, Putti-Platt, Bristow, and DuToit procedures, which frequently provided joint stability but at the expense of glenohumeral motion.
There appears to be no single “essential lesion” as proposed by Bankart 8 that is responsible for recurrent anterior shoulder instability, although the Bankart lesion is by far the most important. The operation must, therefore, be tailored to correct the abnormality that is identified at the time of surgery.
A variety of promising arthroscopic techniques have been developed for the treatment of anterior shoulder instability. However, open stabilization remains the standard procedure for treatment of anterior stabilization (Ref. 19; R. J. Hawkins, unpublished data, 1998), especially for severe instabilities, revision procedures, and for treating athletes who participate in contact sports. Regardless of which procedure is performed, and whether it is performed open or arthroscopically, the treatment should follow the guidelines taught by Rowe 68 : anatomic dissection at the time of surgery, identification and repair of the lesions responsible for the instability, returning tissues to their anatomic locations, and early postoperative range of motion. By following these guidelines, the results of treatment of anterior instability of the shoulder can be optimized.