
Abstract

The efficacy of applying a brace to a knee with a torn ACL is based on studies that have demonstrated a reduction in pathologic anterior translation of the tibia, relative to the femur, with the joint nonweightbearing.1,11,16,24 Recognizing that athletes depend on braces for protection during activities that impart substantial loads to the knee, Wojtys et al. 23 evaluated subjects with ACL-deficient knees while they were nonweightbearing and, more importantly, during weightbearing. Compared with the unbraced condition, bracing reduced anteroposterior (AP) laxity of the knee between 28.8% and 39.9% with the leg muscles relaxed and up to 84.9% with the muscles contracted, demonstrating that the effect of a functional brace on the ACL-deficient knee was dependent on whether the limb was weightbearing or nonweightbearing.
Currently, our understanding of the effect of braces on knees with ACL tears is based on studies that have been performed with the joint in either unweighted or weightbearing conditions, and very little is known about the effect of bracing on the knee during the transition between these circumstances. The latter condition is important because when a subject with a chronic ACL tear transitions between nonweightbearing and weightbearing postures, the tibia undergoes a dramatic anterior translation relative to the femur that can be three to four times greater than normal.3,20 Thus, our understanding of the effect of bracing on the knee is limited to measurements of translation of the tibia relative to the femur during isolated loading conditions (that is, while the knee is either unweighted or weightbearing) rather than a comprehensive evaluation throughout which an athlete depends on a brace for protection, such as the transition from nonweightbearing to weightbearing.
The objective of this investigation was to measure the effect of commercially available functional knee braces on the displacement response of the ACL-deficient knee while the joint was challenged with loads common to most athletic activities. Our hypothesis was that bracing the ACL-deficient knee during nonweightbearing, throughout the transition to weightbearing, and during weightbearing reduces the abnormal displacement behavior of the tibia relative to the femur to within the limits of the normal knee.
Materials and Methods
Human Subjects
Study Subject Characteristics and Outcome of Clinical Evaluation
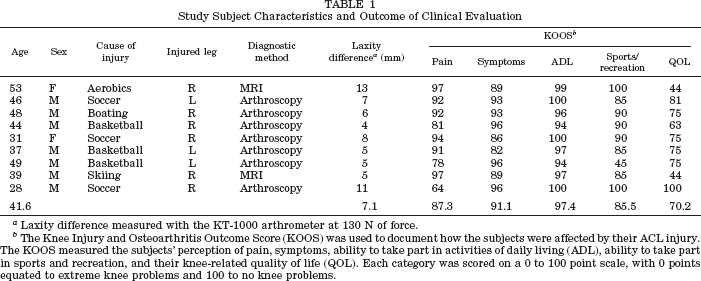
Laxity difference measured with the KT-1000 arthrometer at 130 N of force.
The Knee Injury and Osteoarthritis Outcome Score (KOOS) was used to document how the subjects were affected by their ACL injury. The KOOS measured the subjects' perception of pain, symptoms, ability to take part in activities of daily living (ADL), ability to take part in sports and recreation, and their knee-related quality of life (QOL). Each category was scored on a 0 to 100 point scale, with 0 points equated to extreme knee problems and 100 to no knee problems.
Vermont Knee Laxity Device (VKLD)
In an effort to provide a comprehensive description of the knee, we recognized the importance of obtaining a continuous measurement of translation of the tibia relative to the femur while the knee was unweighted (a situation similar to the swing phase of gait), throughout the transition to weightbearing (such as occurs during heel-strike), and while the knee was weightbearing (a condition such as the stance phase of gait). To accomplish this, the VKLD (Fig. 1) was used to measure the displacement response of the tibia relative to the femur in a continuous manner while the knee was nonweightbearing and AP loads were applied, throughout the transition to weightbearing when a compressive load was applied to the foot, and then during weightbearing while AP loads were applied to the knee.
21
A schematic representation of the Vermont Knee Laxity Device (VKLD) with the subject positioned supine. Counter weights were applied to the thigh and shank to eliminate the gravity loads acting on these respective limb segments, creating a zero shear load across the tibiofemoral joint and a reproducible reference for measurement of the position of the tibia relative to the femur. Anteroposterior directed shear loads were applied to the knee through a rack and pinion system that did not flex or extend the knee. Electromagnetic position sensors were fixed to the anterior aspects of the patella and the anteromedial flare of the proximal tibia to measure the translation of the tibia relative to the femur. Applied load and position data were sampled simultaneously and then used to quantify the load-displacement response of the tibia relative to the femur.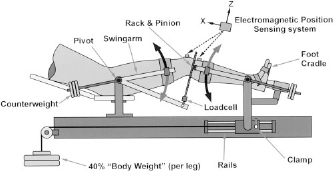
Previous work by our group has demonstrated that the VKLD provides reliable measurements of the AP load-displacement response of the tibia relative to the femur (AP laxity) 21 and accurate measurement of anterior translation of the tibia relative to the femur as the leg transitions from a nonweightbearing to a weightbearing condition. 3
The counterweight portion of the VKLD was used to offset the gravity loads acting on the thigh and shank,3,21 creating a zero shear load at the knee and a reproducible reference for the measurement of translation of the tibia relative to the femur21,25 (Fig. 1). This was accomplished by positioning subjects in the VKLD such that the axes of rotation of the ankle (identified as the most prominent portion of the lateral malleolus) and hip (located by palpating the greater trochanter) were aligned with the axes of rotation of the corresponding shank and thigh portions of the counterweight system (Fig. 1). The subject's feet were strapped to footplates that were equipped with six degree of freedom force sensors (SRMC3A Series, AMTI Incorporated, Newton, Massachusetts) that measured the reaction forces at the foot-footplate interfaces. Each footplate was attached to cradles that were either locked in place, allowing measurement of the AP load-displacement response of the knee while it was unweighted, or unlocked and allowed to slide freely along horizontal rails, permitting evaluation of the translation of the tibia relative to the femur during the transition between unweighted and weighted postures and evaluation of the AP load-displacement response of the knee during weightbearing (Fig. 1). Two-weight stacks, each equal to 40% of the subject's body weight, were applied to the foot cradles, advancing them in a proximal direction, and, as the subject resisted this motion to maintain the knee at 20° of flexion, a compressive load directed through the ankle and hip axes of rotation was created. Shoulder supports ensured that subjects maintained the same position in the VKLD. Anteroposterior directed loads were applied to the knee with a rack and pinion system such that opposing shear loads were applied simultaneously to the thigh and shank in a manner that did not create a flexion-extension moment about the knee. This approach was chosen to allow measurement of AP translation of the tibia relative to the femur produced by the corresponding AP loads, and not the translations that could have been produced by flexion-extension of the knee. An important feature of the VKLD was the capability to provide a continuous measurement of translation of the tibia relative to the femur while the knee was loaded with AP shear and compressive loads. This was accomplished with electromagnetic position sensors (Flock of Birds, Ascension Technologies, Colchester, Vermont) that were strapped to the midportion of the patella and the medial flare of the tibia at the level of the tubercle on each leg. The difference in position between the patella, an indirect but reliable measure of the position of the femur because of its congruency with the trochlea,7,21 and tibia sensors was used to measure the AP translations of the tibia relative to the femur.
Study Design
The subjects were positioned in the VKLD with their knees at 20° of flexion, and supports were located against the subjects' shoulders to maintain them in the same position throughout the testing protocol. The load-displacement responses of both knees were measured with the joints nonweightbearing; the foot cradles were unlocked, allowing application of the compressive loads; and then the load-displacement response of the knee was characterized during weightbearing. This procedure was performed over a short time interval, typically less than 1 minute, during which data were collected continuously. This allowed us to measure the translation of the tibia relative to the femur as the knee changed from nonweightbearing to weightbearing postures and to measure AP laxity during both conditions. This was repeated three times while the ACL-deficient knee was fitted with the following functional braces: The DonJoy Legend (dj Orthopedics, Inc., Vista, California), SofTec Genu (Bauerfeind USA, Inc. Kennesaw, Georgia), and the Townsend Rebel (Townsend Design, Bakersfield, California). Each brace was evaluated in random order. The protocol was finalized by retesting the ACL-deficient knee without a brace applied, to ensure reproducible results.
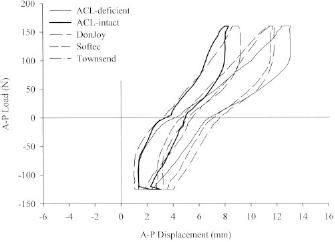
The three before-mentioned loading conditions (nonweightbearing, the transition from nonweightbearing to weightbearing, and weightbearing) were analyzed separately. The first and third conditions involved the application of AP-directed shear loads to the limb and measurement of corresponding AP translations, and for each condition AP translation of the tibia relative to the femur (AP laxity) produced by the 130-N anterior-directed and 120-N posterior-directed loads was determined and used as the dependent variable
21
(Fig. 2). The second condition involved application of the compressive load to the limb and measurement of translation of the tibia relative to the femur produced by the change from nonweightbearing to weightbearing postures, and this was used as the dependent variable (Fig. 2).
3
A two-factor analysis of variance for repeated measures was used to compare the anterior translation values produced by the transition from nonweightbearing to weightbearing between knee status (ACL-deficient versus normal) and brace condition (braced versus unbraced). A similar analysis was used to compare AP laxity values produced by corresponding AP shear loads applied to the knee during nonweightbearing and weightbearing.
The applied AP load versus AP translation data collected with the VKLD for nonweightbearing and weightbearing postures from a typical subject. Definition of the anterior translation and AP laxity values are presented. A positive load value is directed anteriorly (tibia relative to the femur), and a positive translation value represents anterior translation of the tibia relative to the femur.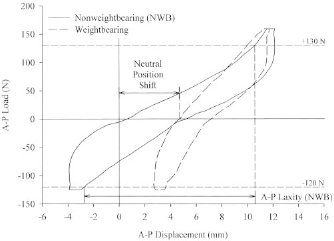
Results
The subjects reported moderate pain with activity (see Table 1 for KOOS scores), and they experienced symptoms with their ACL-deficient knee during daily activity. This did not limit the subjects from participating in their normal activities of daily living; however, it did limit them with regard to taking part in their sport and recreation activities, and this significantly reduced their quality of life. Examination of the subjects with the KT-1000 arthrometer revealed that, on average, the ACL-deficient knees demonstrated 7.1 mm of anterior laxity in comparison with the contralateral, normal knee (Table 1).
The Effect of Bracing the ACL-Deficient Limb on Translation of the Tibia Relative to the Femur during the Transition from Nonweightbearing to Weightbearing Postures
The change from nonweightbearing to weightbearing postures created an anterior translation of the tibia relative to the femur in both the normal and ACL-deficient limbs (Figs. 3 and .4). The anterior translation of the ACL-deficient knee was significantly greater than in the contralateral, normal knee (P < 0.05) (Fig. 5). Anterior translation of the ACL-deficient and normal knees were, on average, 4.6 mm (SD, 3.5) and 1.3 mm (SD, 3.5), respectively.
Mean load versus displacement data for each treatment with the knee nonweightbearing (N = 9). Mean load versus displacement data for each treatment with the knee weightbearing (N = 9). The mean anterior translation of the tibia relative to the femur (in millimeters) produced by transition of the knee from nonweightbearing to weightbearing for each treatment (N = 9). The error bars represent 1 SD.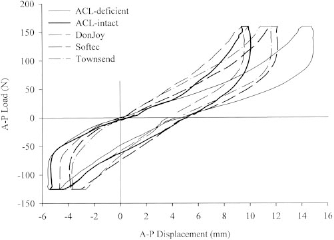
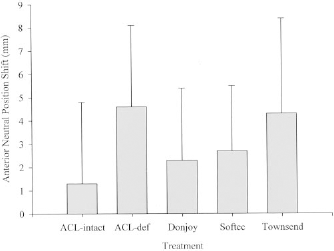
Application of the functional braces to the ACL-deficient knees did not reduce the anterior translations in comparison with the same knees without braces and did not reduce anterior translations to levels within the limits of the normal knees (Fig. 5). The anterior translations of the ACL-deficient knees with the DonJoy, SofTec, and Townsend braces applied were 2.3 mm (SD, 3.1), 2.7 mm (SD, 2.8), and 4.3 mm (SD, 4.1), respectively.
The Effect of Bracing the ACL-Deficient Limb on AP Laxity of the Knee during Nonweightbearing and Weightbearing Postures
As expected, the nonweightbearing ACL-deficient knees demonstrated significantly greater AP laxity values compared with the contralateral, normal limbs (P < 0.05) (Fig. 6). Similarly, during weightbearing, the ACL-deficient knees exhibited significantly greater AP laxity values compared with the normal sides (P < 0.05). The ACL-deficient knees had AP laxity values that were, on average, 17.4 mm (SD, 4.3) and 10.0 mm (SD, 5.5) during nonweightbearing and weightbearing, respectively, and for the normal knees these values were 12.7 mm (SD, 3.6) and 5.7 mm (SD, 2.9).
The mean AP laxity values for each treatment with the knee nonweightbearing and weightbearing (N = 9). The error bars represent 1 SD.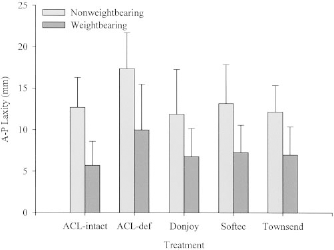
Bracing the ACL-deficient knees significantly reduced AP laxity values compared with the same knees without a brace applied during nonweightbearing and weightbearing conditions (P < 0.05). In each case, bracing the ACL-deficient knees restored AP laxity values to within the limits of the normal joints (Fig. 6). The AP laxity values for the nonweightbearing, ACL-deficient knees with the DonJoy, SofTec, and Townsend braces applied were, on average, 11.9 mm (SD, 5.4), 13.2 mm (SD, 4.7), and 12.2 mm (SD, 3.2), respectively, as compared with 17.4 mm (SD, 4.3) for the same knees without braces. During weightbearing, the same combination of braces produced values that were 6.8 mm (SD, 3.4), 7.3 mm (SD, 3.3), and 7.0 mm (SD, 3.4), respectively, as compared with 10.0 mm (SD, 5.5) for the same knees without a brace applied.
Discussion
This study demonstrated that knees with chronic ACL tears have significantly greater AP laxity values in comparison with the contralateral, normal knee during nonweightbearing and weightbearing circumstances and undergo a 3.5-fold increase in anterior translation when changing between these postures (on average, the normal and ACL-deficient knees underwent 1.3 and 4.6 mm of anterior translation, respectively). The latter finding confirms results of the earlier cadaver study by Torzilli et al. 20 that demonstrated that transition of the knee between nonweightbearing and weightbearing conditions produced an anterior translation of 5 mm for ACL-intact knees and 13 mm for ACL-sectioned knees (a 2.6-fold increase). This finding is also in agreement with earlier work from our laboratory in humans that revealed an anterior translation of 0.8 mm for normal knees and 3.4 mm for ACL-deficient knees (a 4-fold increase). 3 The observation that knees with a chronic ACL tear undergo a 4.6-mm increase in anterior translation (range, 1.4 to 10.6 mm) is not only a concern because it is significantly greater than that in the contralateral, normal knee (range, 0.5 to 3.3 mm), it is also substantially greater than 2.7 mm, or the 95% confidence intervals based on the side-to-side difference in AP laxity measured from subjects with normal knees during nonweightbearing. 6 In the ACL-deficient knee, the increased anterior translation of the tibia is restrained by other structures, such as the posterior horns of the menisci that wedge apart the articular surfaces of the tibiofemoral joint.14,19 This may explain, at least in part, the mechanism that produces the high incidence of meniscal tears associated with chronic ACL deficiency.12,13,22 From these perspectives, one should consider the anterior translation associated with the ACL-deficient knee to be abnormal. It is important to point out that the relationship between increased anterior translation, cartilage contact, and cartilage metabolism is unknown. As a result, it is difficult to assess what magnitude of the translation is acceptable and what proportion is deleterious to the intraarticular structures such as the menisci. Therefore, it is unclear what proportion of the increased anterior translation and AP laxity values should be reduced by a functional brace.
Our rationale for evaluating the effect of a functional brace on the knee in a sequential manner from nonweightbearing, throughout the transition to weightbearing, and then during weightbearing is based on a variety of important observations. These include the following: reproduction of the loading environment in which a subject depends on a brace for protection4,5,9,23; challenging the knee with muscle contraction and body weight to either increase ACL strain values in the normal knee4,8 or to produce the abnormal anterior translation of the tibia in the ACL-deficient knee 3 ; and including the stiffness of the soft tissues of the lower limb, the critical link that controls the transmission of forces from the brace to the tibia and femur, and, therefore, its ability to protect articular structures. 5 Most of what is known about the effect of functional braces on the ACL-deficient limb is derived from studies that have been performed on the nonweightbearing knee (that is, the forces produced by body weight and muscle contraction have not been included), and in the majority of these studies, researchers have applied AP loads to the joint while measuring the corresponding AP laxity. These studies have been performed in surrogate limbs, 15 cadavers,1,10,24 and humans2,11,16,23 and have shown that bracing reduces the abnormal AP laxity associated with the ACL-deficient knee. We confirmed these findings by demonstrating that during nonweightbearing the ACL-deficient knee had, on average, a 37% increase in AP laxity compared with the normal side and that bracing the ACL-deficient knees reduced these values to within 2.1% of the value in the normal knee. During weightbearing, the ACL-deficient knees demonstrated a 75% increase in AP laxity compared with the normal side, and bracing reduced the AP laxity values to within 23.4% of normal. These findings are similar to those reported by Wojtys et al. 23
An important feature of our investigation was the approach of measuring the anterior translation (produced by the internal loads created by contraction of the muscles and the compressive load acting at the foot) and AP laxity (created by the external shear loads applied by the VKLD) and using both to quantify the biomechanical behavior of the knee. This enabled us to characterize the complete displacement response of the tibia relative to the femur throughout the transition from nonweightbearing to weightbearing and during each respective posture. Although we demonstrated that several different commercially available functional braces were capable of reducing AP laxity of the ACL-deficient knee to within the limits of the contralateral, normal knee during nonweightbearing and weightbearing conditions, none of the braces reduced the anterior translation of the ACL-deficient knee to within the limits of normal during the transition from nonweightbearing to weightbearing. The latter finding is similar to that reported by Ramsey et al., 17 who implanted Steinmann pins into bone to directly measure displacement of the tibia relative to the femur during gait in subjects with ACL-deficient knees. They found that bracing the ACL-deficient knee did not produce changes in displacement of the tibia relative to the femur compared with the unbraced condition.
The work of Ramsey et al., when considered in combination with the findings from our study, indicates that the use of commercially available functional braces on ACL-deficient limbs can provide a beneficial reduction of abnormal AP laxity when AP-directed loads are applied to the tibia from an external source. An example of this would be when an anterior force is applied to the posterior aspect of an athlete's calf; however, bracing does not appear to provide control of the abnormal anterior translations that occur when the internal loads of body weight and muscle contraction are applied, at least to the extent that they are restored to within the limits of the normal knee. To our knowledge, this is a new and important observation because it suggests that during the transition from nonweightbearing to weightbearing, which is a common occurrence during activities such as the heel-strike phase of gait or when changing direction during a pivot maneuver, bracing may not be capable of reducing the abnormal anterior translation of the ACL-deficient knee to within the limits of the normal joint. This finding may help explain why subjects with ACL-deficient knees report giving-way episodes or abnormal translations at the knee while using a functional brace.
It is important for us to point out that athletes with an injured, disrupted, or reconstructed ACL depend on a functional brace for protection during activities that produce substantial compression and shear loads across the knee, and not only the moderate loads created by the VKLD. The VKLD was developed to measure knee biomechanics during passive conditions that involve relaxed muscles and during dynamic activities that include contraction of the leg muscles, such as occurs during weightbearing. The VKLD allowed us to apply controlled loads and continuously monitor the translation of the tibia relative to the femur during nonweightbearing, throughout the transition to weightbearing, and while the subjects were weightbearing. We considered this to be important because when subjects with ACL tears experience giving-way episodes at the knee, they frequently do so when their knee is exposed to the same nonweightbearing-to-weightbearing loading sequence.
Although it was never our intent to apply loads to the knee and create a giving-way episode, we were able to produce a dramatic anterior translation of the tibia relative to the femur that was 3.5 times greater than normal. In one subject, the anterior translation was 10.6 mm. This response occurred with application of the compressive joint load through the ankle and hip axes of rotation, a loading condition that we consider similar to that of landing from a vertical jump with both feet at shoulder width. The primary difference between the loading condition used in this study and that created by landing from a vertical jump was that the subjects were positioned supine in the VKLD and, therefore, the loads produced by the muscles that span the hip and stabilize the pelvis were different. These differences were considered minor and only had a pronounced effect on the biomechanical behavior of the hip. The loads that were produced about the ankle and knee were considered representative of weightbearing. Our future research will focus on other complex loading conditions, such as compressive loading combined with internal-external torque applied to the knee.