
Abstract
Background: The relevance of headache to outcome after sports-related concussion is poorly understood.
Hypotheses: High school athletes reporting headache approximately 1 week after injury will have significantly more other concussion symptoms and will perform more poorly on neuropsychological tests than athletes not experiencing headache.
Study Design: Prospective cohort study.
Methods: Study participants included 109 high school athletes who had sustained concussion and who were divided into two groups: those reporting headache 7 days after injury and those reporting no headaches. The two groups were compared regarding on-field markers of concussion severity at the time of injury and symptoms and neurocognitive test results collected via ImPACT, a computerized neuropsychological test battery and postconcussion symptom scale, at a mean of 6.8 days after injury.
Results: Athletes reporting posttraumatic headache demonstrated significantly worse performance on reaction time and memory ImPACT neurocognitive composite scores. These athletes also reported significantly more symptoms other than headache and were more likely to have demonstrated on-field anterograde amnesia.
Conclusions: Findings suggest that any degree of postconcussion headache in high school athletes 7 days after injury is likely associated with an incomplete recovery after concussion.
In the United States, 50,000 to 300,000 athletes sustain a concussion each season.9,25,26 More than 15 grading systems and return-to-play parameters have been published since 1973 to assist the team physician, athletic trainer, and coach in the evaluation and management of concussion. Variability in these management directives is attributable to a lack of scientific foundation, leading to an arbitrary delineation of concussion grades and criteria for return to play.4,15 At the current time, most concussion scales predicate return to play on the presence and duration of loss of consciousness or amnesia. However, neither symptom needs to be present for an injury to be classified as a concussion. In fact, a recent study of concussion in high school and collegiate football players revealed that loss of consciousness and amnesia occur relatively infrequently, in only 9% and 28% of concussion cases, respectively. 12
A more common feature of sports concussion is the occurrence of posttraumatic headache. McCrory et al. 22 and Guskiewicz et al. 12 have reported the frequency of postconcussive headache to be as low as 40% or as high as 86%, respectively. Despite the high prevalence of postconcussion headache, no current concussion grading scale includes this specific symptom as a criterion for defining severity of injury. In a general sense, most widely quoted guidelines, such as those of the Sports Medicine Committee of the Colorado Medical Society, 23 the American Academy of Neurology, 17 and the Cantu grading system 2 note that persistence of symptoms (such as headache) is a contraindication for return to play after concussion. Alternatively, because of the high frequency of headaches among athletes who have not sustained a concussion, 27 some physicians have advocated return to play for athletes who have persistent headache but normal results of neurologic sideline examinations. 24 Lack of prospective research in this regard has led to varied management options and subsequent confusion when headache is the primary clinical symptom. Recent recommendations from an international meeting on the topic of sports concussion 1 and prior recommendations from the AOSSM 28 have reinforced the need to reevaluate all concussion-severity grading systems. Both groups have stressed the need for the collection of prospective data regarding signs and symptoms of injury for correlation with outcome.
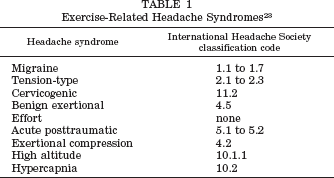
In 1997, the International Headache Society and the World Health Organization proposed a classification scheme for headaches. 14 This nomenclature did not adequately address differences among the various headache types commonly seen in athletes. To help clarify these issues, McCrory 21 later published an article that classified exercise-related headache syndromes into nine subtypes (Table 1). Acute posttraumatic headache was further delineated into six distinct classifications, although the author acknowledged that comorbidity and overlap of these headache subtypes are the norm. The management of posttraumatic headache is further complicated by the high percentage of athletes who experience other forms of nontraumatic exercise-related headaches. In a general sense, the significance of sports-related posttraumatic headache remains unknown, and, to date, no outcome study has examined this issue in athletes.
Exercise-Related Headache Syndromes 23
The current study was designed to investigate whether postconcussion headaches are associated with neurocognitive and other symptom impairment at approximately 1 week after injury in a large subset of high school athletes. Outcome variables for this study were derived from a computerized neuropsychological test battery. Four composite scores from this battery of tests were used, including a postconcussion symptom scale score and overall scores for reaction time, processing speed, and memory. It was hypothesized that high school athletes reporting headache at approximately 1 week after injury would report significantly more other concussion symptoms and would perform more poorly on neuropsychological testing than athletes who did not experience headache.
Materials and Methods
Subjects
Approval for this study of human subjects was granted through the University of Pittsburgh Institutional Review Board. Study participants were from 20 select high schools participating in the University of Pittsburgh Medical Center Sports Concussion Program within the states of Pennsylvania (10), Michigan (2), Illinois (2), Oregon (3), and Maine (3). The University of Pittsburgh Medical Center Sports Concussion Program is an ongoing clinical program that provides oversight and consultation regarding the implementation of neuropsychological tests to assist team medical staff in making objective return-to-play decisions after the occurrence of sports-related concussion. All 109 athletes from these institutions who sustained a sports-related concussion during the 2000 and 2001 athletic seasons were included in the current analysis.
The average age of the athletes was 15.8 years (SD, 1.2), and 84.5% (93) were male. The majority of concussed athletes were football players (64.2%, or 70 of 109). Other represented sports included basketball (14, or 12.8%), soccer (13, or 11.9%), hockey (4, 3.7%), lacrosse (3, 2.7%), softball (2, 1.8%), track (1, 0.9%), volleyball (1, 0.9%), and wrestling (1, 0.9%). Half of the subjects (55, 50.4%) reported at least one previous concussion, 37 (33.9%) reported that this was their first concussion, and data regarding previous concussions was missing for 17 (15.6%) of the athletes. Athletes were excluded from the study if a CT scan or MRI showed evidence of a hematoma or skull fracture, if there was a preexisting history of neurologic disease (such as a seizure disorder or brain tumor), if they had posttraumatic amnesia of more than 24 hours duration, or if they refused to participate in the study. No athlete was excluded on the basis of these criteria.
Initial on-field assessment was made by a certified athletic trainer or physician who was present at the time of injury. Concussion was diagnosed based on one or more of the following criteria as identified by on-field, court, or rink examination: 1) any observable alteration in mental status or consciousness; 2) loss of consciousness or presence of anterograde amnesia (difficulty in forming new memory after trauma) or retrograde amnesia (difficulty in recalling events during the period immediately preceding the trauma); or 3) evidence of a constellation of postconcussion symptoms, such as cognitive “fogginess,” nausea or vomiting, dizziness, balance problems, visual changes, or presence of posttraumatic headache after a collision involving the head or body.
Protocol and Outcome Measures
Data were collected through the administration of ImPACT, a computerized neuropsychological test battery used by all participating institutions that was designed specifically for diagnosis and management of sports-related concussion. The self-administered test battery consisted of seven individual cognitive test modules. Composite scores in the areas of memory, reaction time, and processing speed were computed by standardized formulas derived from the results of the seven individual cognitive tasks (Table 2). In addition, the computerized inventory included data from the postconcussion symptom scale, 18 which is now being used throughout both amateur and professional sports (Table 3). This Likert scale consists of 19 symptoms commonly associated with concussion (such as headache, dizziness, sleep deficits, nausea, and feeling slowed down) that are graded by the administrator from 0 (asymptomatic) to 6 (severely symptomatic). A more detailed description of the individual tests, computerized test battery, and the rationale for its development has been described previously. 19
ImPACT Neurocognitive Test Modules a
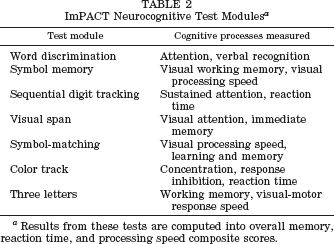
Results from these tests are computed into overall memory, reaction time, and processing speed composite scores.
Symptoms Rated in the Postconcussion Symptom Scale18a
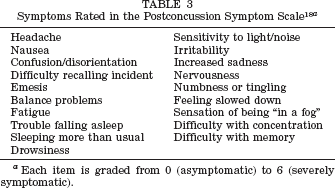
Each item is graded from 0 (asymptomatic) to 6 (severely symptomatic).
Postconcussion Evaluation
All concussed athletes were referred and subsequently evaluated via computerized neuropsychological testing 5 to 10 days after the diagnosis of concussion (mean, 6.8 days). Administration of the inventory was supervised by a team of clinical neuropsychologists, athletic trainers, or physicians who had been thoroughly trained in the use and implementation of the test battery. Training was completed at each site through a half-day seminar presented by one of the lead authors (MWC or MRL).
At the seminar, staff members were also trained to identify and document the presence and duration of on-field markers of concussion severity, including the presence and duration of disorientation, anterograde or retrograde amnesia, and loss of consciousness. For the purposes of this study, on-field disorientation was assessed by questioning the athlete's awareness of and orientation to surroundings (for example, his or her name, the current stadium, city, opposing team, and the current date) after the injury. On-field anterograde amnesia was assessed through immediate and delayed (0, 5, 15 minutes) memory for three words (for example, girl, dog, green). Anterograde amnesia was further documented at the follow-up evaluation by assessing the athlete's ability to recall all information subsequent to the trauma. Any loss of memory in this latter regard indicated the positive presence of anterograde amnesia. On-field retrograde amnesia was assessed by having the athlete recall events occurring just before the trauma (such as events that occurred in the first quarter, memory for play preceding the trauma, and the score of the game). Retrograde amnesia was further documented by assessing the athlete's ability to recall information from before the trauma. Any loss of memory in this latter regard indicated positive presence of retrograde amnesia. Loss of consciousness was documented when an athlete was unresponsive to external stimuli and in paralytic coma as reported by teammates or on-field evaluation. By definition, athletes experiencing loss of consciousness also experienced concomitant anterograde amnesia. For the purposes of this study, athletes with any degree of loss of consciousness were categorized in the positive loss of consciousness group rather than the anterograde amnesia group, regardless of the length of associated amnesia.
All aspects of the ImPACT evaluation were implemented in a standardized fashion. Further, results of the evaluation were automatically computer-scored and generated within a five-page clinical report. Therefore, there was no variation in administration or scoring technique between the participating sites.
Results
Data Analysis and Formulation of Headache Groups
Data collected from individual concussed athletes at participating institutions were pooled and analyzed with the Statistical Package for the Social Sciences 10.0 software (SPSS, Inc., Chicago, Illinois). Concussed athletes were divided into two groups on the basis of self-reported headache at the time of the follow-up neuropsychological evaluation. The first group reported no headaches at this follow-up interval (N = 73), whereas the second group reported experiencing headaches (N = 36). Concussed athletes were included in the headache group if they reported any degree of headache on the 6-point postconcussion symptom scale, with 1 indicating very mild headache and 6 indicating severe headache. The breakdown of this group by headache severity was as follows: 1 point, 5 athletes (13.9%); 2 points, 9 (25%); 3 points, 15 (41.7%); 4 points, 5 (13.9%); and 5 points, 2 (5.6%). The headache and no-headache groups did not differ in age (P < 0.80), sex (P < 0.81), or history of previous concussions (P < 0.28).
A subset of the concussed athletes in our sample, 53 subjects in the no-headache group and 20 in the headache group, had undergone preinjury baseline neuropsychological testing with ImPACT, conducted before the 2000 and 2001 athletic seasons. Student's t-tests were used to compare the preseason test scores for the two groups. The groups did not differ at baseline in terms of total self-reported symptoms (P < 0.23), preinjury headache prevalence (P < 0.81), memory performance (P < 0.43), reaction time (P < 0.21), or processing speed (P < 0.41).
Postconcussion Symptom and Cognitive Test Results
At approximately 7 days after concussion, athletes with headaches experienced a large number of other postconcussion symptoms compared with the athletes with no headaches (P < 0.001; D = 1.55, very large effect size). In addition, athletes with postconcussion headaches had significantly slower reaction times (P < 0.001; D = 0.80, large effect) and reduced memory performance (P < 0.02; D = 0.60, medium effect) as measured by the neuropsychological cognitive composite scores. The two groups did not differ on the processing speed composite score. Descriptive statistics, mean comparisons, and effect sizes are presented in Table 4.
Descriptive Statistics, Mean Comparisons, and Effect Sizes for Headache Groups a
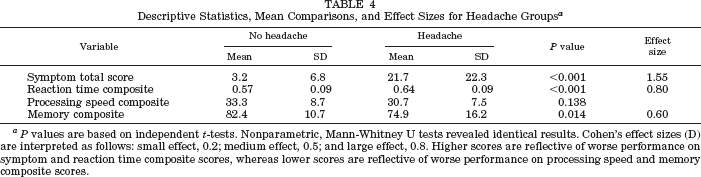
P values are based on independent t-tests. Nonparametric, Mann-Whitney U tests revealed identical results. Cohen's effect sizes (D) are interpreted as follows: small effect, 0.2; medium effect, 0.5; and large effect, 0.8. Higher scores are reflective of worse performance on symptom and reaction time composite scores, whereas lower scores are reflective of worse performance on processing speed and memory composite scores.
Athletes who reported headaches at approximately day 7 after injury were subdivided into two groups: those with mild headache (2 or 1 on the scale) versus those with moderate-to-severe headache (3 or higher on the scale). Fourteen subjects had mild headaches and 22 had moderate-to-severe headaches. These subgroups were compared on the primary dependent measures. Those with moderate-to-severe headaches reported a much higher number of other postconcussion symptoms relative to those with mild headache (means, 30.2 versus 8.3; P = 0.001; D = 1.2, very large effect size). There were no statistically significant differences between the two groups on the three neuropsychological composite scores. However, all ImPACT composite scores were reduced in the group with moderate-to-severe headaches. Because of the small sample size, there was low power for these latter analyses. It is notable that the effect size for the reaction time composite was 0.46, a medium effect, indicating that there was approximately a one-half standard deviation difference between groups. The effect sizes for memory and processing speed were small (D = 0.19 and 0.32, respectively).
Relationship of Headache to On-Field Markers of Concussion Severity
The two groups composing the total sample were used to investigate the relation between on-field injury severity markers and headache status at 1 week after injury. Chi-square between-group comparisons were conducted by using the on-field markers as dependent variables. As seen in Table 5, athletes with postconcussion headache were significantly more likely to experience on-field anterograde amnesia (ρ 2 = 4.2, P = 0.04). However, they were not more likely to experience an initial on-field loss of consciousness, retrograde amnesia, or disorientation. If the four primary on-field severity markers are considered simultaneously, 7 of the 73 athletes (9.4%) with no headache 1 week later evidenced three or four of these markers, whereas 11 of the 36 athletes (30.6%) in the postconcussion headache group evidenced three or four abnormal markers. An odds ratio revealed that players with postconcussion headache were approximately four times more likely to demonstrate three or four abnormal on-field markers of concussion severity.
On-field Concussion Severity Markers by Headache Group
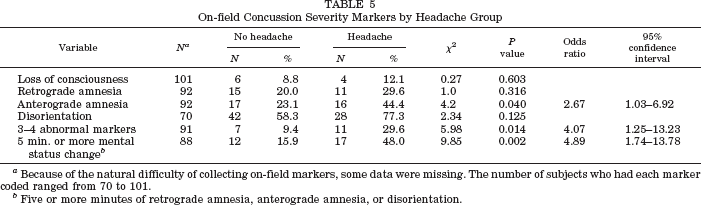
Because of the natural difficulty of collecting on-field markers, some data were missing. The number of subjects who had each marker coded ranged from 70 to 101.
Five or more minutes of retrograde amnesia, anterograde amnesia, or disorientation.
A variable representing on-field mental status change for 5 minutes or more was also created to differentiate transient from more severe injuries; it represents a common unit of time that can be tracked relatively easily on the athletic playing field. Twelve of the 73 players (16%) with no headache had prolonged postinjury mental status changes compared with 17 of the 36 players (48%) who reported headaches at approximately day 7 after injury. An odds ratio revealed that players with headaches were nearly five times more likely to demonstrate 5 minutes or more of sideline-assessed mental status change.
Discussion
The significance of headache after sports-related concussion is frequently and understandably questioned by physicians, athletic trainers, and coaches because as many as 86% of athletes who have sustained a concussion report posttraumatic headache. 12 Somewhat disconcerting, however, is that no prospective study has examined whether postconcussion headache is associated with neurocognitive impairment and presence of other postconcussion symptoms and thus suggestive of incomplete recovery. Moreover, neither headache nor even general clinical outcome after sports-related concussion in high school athletes has been studied.
Our findings suggest that high school athletes who have reported any degree of headache at approximately 1 week after injury are likely to have persistent adverse effects from their concussion, including the presence of other postconcussion symptoms and attenuated neurocognitive functioning. Headaches rated as moderate-to-severe may be associated with even worse neurocognitive status. Unfortunately, the sample size was insufficient to investigate this latter issue fully, although a trend in the data was suggestive.
The presence of postconcussion headache at approximately 7 days after injury was associated with a large number of postconcussion symptoms other than headache. There was a significant difference in the total number of symptoms reported by the headache and no-headache groups, as shown in Table 4.
Athletes reporting a headache at approximately day 7 after injury also demonstrated significantly slowed reaction times and reduced memory performance, and thus slower neurocognitive recovery curves, as measured by ImPACT. The underlying physiologic rationale to explain this association is difficult to ascertain, especially given the lack of specificity regarding headache subtype in our sample.
Other results from our analysis revealed that high school athletes with persistent postconcussion headaches sustained more severe concussions, as a group. Specifically, they were four times more likely to evidence three or four abnormal on-field injury severity markers, and were also five times more likely to show sideline-assessed mental status changes of 5 minutes or more. In terms of individual on-field severity markers, anterograde amnesia was significantly related to the presence of headaches at approximately 1 week after injury. Loss of consciousness, retrograde amnesia, and disorientation did not individually differentiate the headache group from the no-headache group.
Findings from the current study do not appear attributable to preexisting differences between the groups. Approximately two-thirds of our sample underwent preinjury baseline evaluation of neurocognitive and symptom status with ImPACT. Comparisons between these results for the headache and no-headache groups revealed no differences in terms of presence of concussion-related symptoms or neurocognitive test results. Moreover, these groups did not differ in terms of age, sex, or history of previous concussions.
Specific methodologic limitations of our study deserve mention. First, because our analysis examined athletes at only one time interval (on average, at 7 days after trauma), we could not determine the exact time frame and nature of headache onset and resolution (at the time of injury or delayed onset), nor the relationship of headache to the onset of other postconcussion symptoms. Similarly, our data did not indicate whether resolution of postconcussion headache was correlated with resolution of the ImPACT neurocognitive test data. If the resolution of headache is correlated with a return to baseline on cognitive and other symptom measures, it may potentially serve as an indicator determining the time of safe return to sports participation after concussive injury. Future studies are needed to prospectively examine the specific temporal pattern of posttraumatic headache and its relationship to other concussive symptoms and to neurocognitive status.
In addition, we examined “general” postconcussion headache without taking into account specific types of headache and exercise-related headache syndromes (Table 1). As McCrory 21 has stated, further studies are needed to examine the issue of sports-concussion headache and to develop uniform headache categorizations similar to those outlined by the International Headache Society diagnostic criteria. 14 Such studies might be designed to determine the incidence and relevance of specific exercise-related headache syndromes in the athlete (Table 1). On the basis of our experience, the relationship between exertion (physical activity) and postconcussion headache is salient. The current study did not measure or control for the postinjury level of exertion or physical or mental activity of the athletes. Thus, future studies might examine the role of exertion on the presence and duration of headache, other symptoms, and outcome. Such data may help to suggest better strategies for management of patients during recovery from concussion.
Notwithstanding the study limitations, our findings suggest a simplified general management and return-to-play heuristic for use by sports medicine practitioners. The presence of postconcussion headache is significantly associated with increased risk for incomplete recovery; high school athletes who report any degree of headache at approximately 1 week after concussion are likely to have persistent adverse effects across symptom and neurocognitive domains. Therefore, until follow-up studies are completed, it is recommended that such patients, regardless of the severity of the headache, be managed conservatively in terms of return to sport participation. Results of this study are in accordance with a recently published international consensus statement that concussed athletes who are symptomatic should be withheld from sport competition. 1
An athlete with a postconcussion headache may benefit from repeat physical examination and symptom assessment and an individualized evaluation to help delineate underlying deficits associated with the injury. Several diagnostic procedures and referral sources are currently available for use by the sports medicine practitioner. For example, neuropsychological testing can help to delineate the presence of underlying deficits associated with injury.3,6,13 Other neurodiagnostic techniques, such as postural stability testing,10,11 functional MRI,16,20 positron emission tomography, 8 and electrophysiologic measures,5,7 may also help to uncover lingering effects of concussive injury.