
Abstract
Background: Neither operative nor nonoperative treatment of posterior cruciate ligament rupture after multiligament knee injuries have shown very favorable outcomes.
Hypothesis: Reconstruction of the posterior cruciate ligament by combining the tibial-inlay and two-femoral-tunnel techniques will result in improved stability and functional outcomes.
Study Design: Prospective cohort study.
Methods: Twenty-nine patients with 30 posterior cruciate ligament ruptures and multiligament knee injuries treated with the combined technique were evaluated with clinical, radiographic, and functional outcome measures.
Results: All patients had a clinical examination result indicating joint stability (0 or 1+) at an average follow-up of 25 months (range, 15 to 39). Twenty-three knees had no laxity, and seven had 1+ laxity. The KT-2000 arthrometer data documented less than 0.5 mm of side-to-side mean difference for both posterior displacement and total anterior-posterior displacement at both 30° and 70° of knee flexion. Knee range of motion was a mean extension of 1° (range, 0° to 10°) and a mean flexion of 124° (range, 75° to 145°). Mean Lysholm knee score was 89.4.
Conclusions: Reconstruction with a combination tibial-inlay and two-femoral-tunnel technique provides good results after multiligament knee injuries. All patients had a stable posterior cruciate ligament at most recent clinical follow-up, and 77% had no laxity at all.
Rupture of the PCL is frequently a catastrophic injury to the knee associated with poor clinical outcomes because, as numerous authors have noted, the PCL is the primary posterior stabilizer of the knee.8,9,14,17,18,28,32,36 The choice of appropriate treatment for isolated PCL tears is controversial.1,8,11,14,15,18–20,23,24,27,28,32,34,36 However, there is a consensus that surgical stabilization is indicated for PCL tears associated with multiligament knee injuries.4,9,28,35 Some authors report acceptable results from nonoperative treatment of a ruptured PCL with long-term follow-up.4,30,34 However, authors of a number of recent articles have suggested that outcomes of nonoperative treatment are poor and characterized by instability, limited functional capability, and late degenerative changes.4,8,10,18–20
Although nonoperative treatment of PCL tears has yielded poor results, outcomes after surgical intervention have also been disappointing. Direct repair of midsubstance PCL tears has been attempted but has resulted in universal failure.1,27 Repair of bony avulsions has yielded consistently good results.3,15,32,34 Arthroscopic reconstruction of the PCL with a transtibial tunnel has become a commonly used technique that has clearly yielded improved stability when compared with the findings of the preoperative examination, but patients frequently retain grade 1 or 2 laxity.6,12,16,23,26,28
It has been suggested that two major factors may explain late loosening and low-grade laxity after surgical stabilization. The first factor is the acute angle that the graft must make to round the posterior lip of the tibia when exiting the transtibial tunnel. The angle has been described as “the killer turn” and can lead to abrasion of the graft and subsequent laxity and failure. 2 The second factor is that, although the PCL has at least two distinct bundles functionally, which tighten at different degrees of knee flexion,10,14,18,28 the transtibial arthroscopic technique reproduces only the anterolateral bundle. Some contemporary surgical techniques have been developed that attempt to address these shortcomings of the single-incision arthroscopic method. The tibial-inlay technique addresses the potential problems associated with the killer turn by placing a bone block in a trough on the posterior tibia at the site of insertion of the PCL.2,9,21,32 The two-femoral-tunnel technique allows reconstruction of both the anterolateral and posteromedial bundles of the PCL.7,25
The purpose of this paper was to present the results of a unique method of PCL reconstruction combining the tibial-inlay and two-femoral-tunnel techniques. Our hypothesis was that a more precise reconstruction of the natural anatomy of the PCL will result in improved stability and functional outcomes.
Materials and Methods
Patients
Our patient population consisted of 29 patients with 30 PCL tears that were treated with the combination tibial-inlay and two-femoral-tunnel technique between May 1998 and August 2000 at the University of Alabama at Birmingham Hospital. Patients eligible for inclusion in the study had sustained a PCL tear that required reconstruction and were available for at least 12 months of follow-up. Mean follow-up was 25 months (range, 15 to 39). Patients with bony avulsions of the PCL amenable to repair were excluded. Patients were followed in the clinic with serial physical examinations, recording of Lysholm knee scores, 33 KT-2000 arthrometer (Medmetric Corp., San Diego, California) evaluations, and Short-Form 36 (SF-36) outcome evaluations. Our study cohort consisted of 20 men and 9 women with a mean age of 30 years (range, 16 to 54). The average injury severity score was 20 (range, 9 to 50), with 20 patients having a score of 16 or higher, signifying multisystem trauma. Mechanisms of injury included motor vehicle accident (16), motorcycle accident (5), pedestrian struck by motor vehicle (3), fall (2), equestrian accident (1), boating accident (1), and sports injury (1). Twelve patients required admission to the intensive care unit for a mean of 11 days (range, 3 to 32). Fourteen patients (48%) sustained 16 ipsilateral extremity fractures, including 7 femur fractures, 5 tibial plateau fractures, 3 acetabulum fractures, and 1 tibial shaft fracture. Seven patients had peroneal nerve injuries and three had vascular injuries requiring repair at the time of admission. Four patients had grade III open fracture-dislocations.
All of the patients in our study sustained multiligament knee injuries. According to the Cooper classification of PCL tears (Table 1), 9 our patients’ tears were categorized as follows: 1 as IIA, 20 as IIIA, 3 as IIIC, 5 as IVA, and 1 as IVC. These ratings indicate that all of the patients had at least one associated ligament tear. Twenty-four patients with 25 PCL reconstructions had associated meniscal tears. There were 17 medial and 14 lateral tears, and 7 patients sustained tears to both menisci. The 17 medial tears included 6 peripheral tears that were repaired and 11 tears treated with a partial meniscectomy. Twelve of the peripheral tears among the 15 lateral meniscal tears were repaired, with the remainder undergoing a partial lateral meniscectomy. Table 2 provides a summary of the patients, their mechanism of injury, and the knee structures torn.
Classification of PCL Injuries a
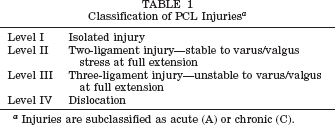
Injuries are subclassified as acute (A) or chronic (C).
Summary of Patient Mechanisms of Injury and Structures Injured
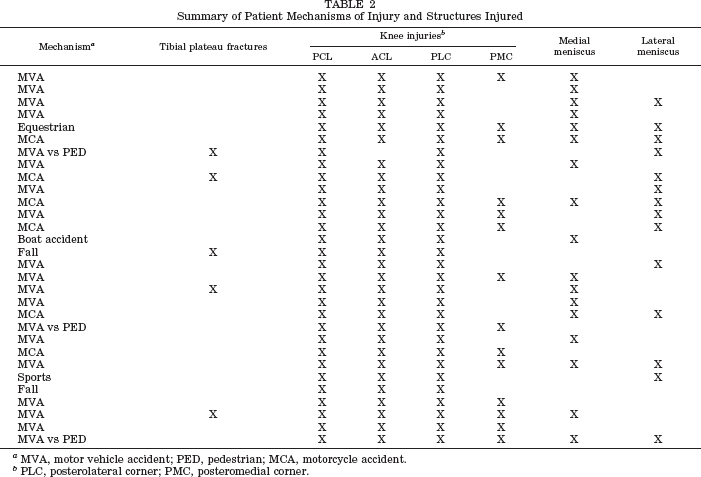
MVA, motor vehicle accident; PED, pedestrian; MCA, motorcycle accident.
PLC, posterolateral corner; PMC, posteromedial corner.
Operative Technique
Our PCL reconstruction is a combination of the tibial-inlay2,9,21,32 and two-femoral-tunnel7,25 techniques (Fig. 1). We are not aware of any other descriptions of this anatomic PCL reconstruction technique. Although the fine details of our technique are beyond the scope of this article, we will give a brief description of our surgical protocol. An Achilles tendon allograft was divided into a larger anterolateral and a smaller posteromedial bundle. The bone block was trimmed, and a permanent No. 2 suture was placed in each bundle to assist passage into the appropriate femoral tunnel. The notch was debrided arthroscopically, and any pathologic conditions of the meniscus were addressed simultaneously. When that was complete, a guide wire was drilled approximately 8 mm from the articular surface within the footprint of the PCL at the top of the notch. A second guide wire was placed posterior and inferior to the first guide wire, with care taken to make certain that they were spaced to provide a bone bridge of approximately 4 mm between the two tunnels. The tunnel size was selected based on the size of the Achilles tendon allografts; a 9-mm anterolateral tunnel and a 7-mm posteromedial tunnel were the most common sizes. The arthroscope was then removed from the knee and a posterolateral or posteromedial approach to the knee was performed, depending on associated ligament conditions. The medial approach was similar to that described by Burks and Schaffer 5 ; the lateral approach was similar but was made through the interval just anterior to the lateral head of the gastrocnemius muscle. A trough was created in the bone at the site of insertion of the PCL into the posterior tibia. Fixation was obtained with a single 4.5-mm cannulated screw and washer placed by using a lag technique. The two bundles were then advanced into the notch and into their respective femoral tunnels. The anterolateral bundle was tensioned at approximately 70° of knee flexion, and the posteromedial bundle was tensioned at approximately 20° of knee flexion. Both bundles were secured with absorbable interference screws that were the same size or 1 mm larger than the size of the tunnel.
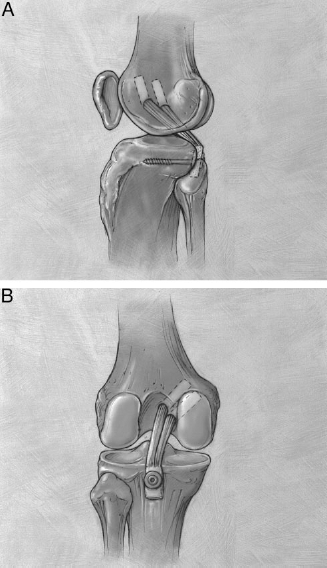
Lateral view (A) and posterior (B) view of the knee showing the combination of tibial-inlay and two-femoral-tunnel techniques.
The ideal timing of surgical reconstruction of multiligament knee injuries after high-energy trauma is unknown. We waited at least 7 days to allow some early healing of the capsule and soft tissues. Every effort was made to reconstruct the PCL and treat associated corner and meniscal injuries within 3 weeks of injury so that repairable structures could be identified and repaired. In cases where soft tissue injuries or associated neurologic, abdominal, or thoracic trauma prevented early surgery, the associated corner injuries were treated with reconstruction rather than repair. In knees with injuries of both cruciate ligaments, the ACL was reconstructed approximately 8 weeks after the PCL reconstruction and corner repairs or reconstructions to initiate rehabilitation of the PCL and obtain at least 90° of motion.
Results
Ligament stability was evaluated by clinical examination as well as by KT-2000 arthrometer evaluations. The clinical examination was graded on a scale of 0 to 3 +. Twenty-three patients with 24 PCL reconstructions received a final grade of 0, and the remaining 6 patients received a final grade of 1 +. Twenty-six of the patients have been evaluated with the KT-2000 arthrometer to date. The patients’ knees were placed at the quadriceps neutral angle, with great care taken to eliminate any residual sag before obtaining arthrometer data. The mean posterior displacement at maximum force and 30° of knee flexion was 1.6 mm on the injured side and 2.0 mm on the uninjured side. The mean posterior displacement at maximum force and 70° of knee flexion was 1.5 mm on the injured side and 1.8 mm on the uninjured side. This yielded a mean side-to-side difference of –0.4 mm at 30° of flexion and –0.3 mm at 70° of flexion. Twelve patients (46%) had knees with less posterior displacement on the injured side than on the normal side at 30° of flexion and 13 (50%) had less posterior displacement at 70° of flexion. The largest positive side-to-side difference between knees was 1 mm at both 30° and 70°.
We recognized the potential for false arthrometer data from patients with both ACL and PCL injuries when only posterior translation was measured; therefore, total anteroposterior (AP) displacement was calculated. At 30° of knee flexion, average total AP displacement at maximum force was 9.2 mm for the injured knee and 7.9 mm for the uninjured knee. This yielded a side-to-side difference of 1.3 mm, with the injured side having slightly greater translation (Fig. 2). When the three patients who had a torn ACL that had not been reconstructed were removed from the calculations, the total AP displacement was 8.1 mm on the injured side and 8.2 mm on the uninjured side. The side-to-side difference in patients who had both cruciate ligaments reconstructed was 0.1 mm, with the uninjured side having slightly greater translation (Fig. 2). Similarly, at 70° of flexion, the side-to-side difference for all patients was 1.1 mm, with the injured side having slightly greater translation. When the ACL-deficient patients were eliminated from the calculation, the side-to-side difference was 0.2 mm, with the injured side having slightly greater translation. Only one patient who had both cruciate ligaments reconstructed had 5 mm or greater total AP translation.
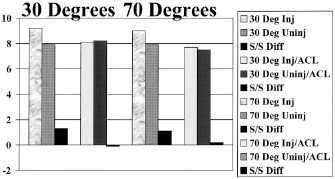
Total AP translation at 30° and 70° of knee flexion showing the side-to-side difference (S/S Diff) in patients who had both cruciate ligaments reconstructed. Inj, injured; Uninj, uninjured; Diff, difference.
Range of motion was a mean of 1° of extension (range, 0° to 10°), with 26 patients having full extension; two had a loss of 5°, and two had a loss of 10° of terminal extension. One of the patients with a 10° flexion contracture walks with a slight limp, but he had an ipsilateral acetabular fracture and significant heterotopic ossification at both the hip and knee. The mean flexion was 124° (range, 75° to 150°). Seven knees had flexion of less than 120°; two knees had less than 100° of flexion. Twelve of the 30 knees (40%) developed a degree of arthrofibrosis or difficulty obtaining motion and required manipulation under anesthesia or arthroscopic lysis of adhesions or both. It should be noted that six of the nine women in our study had problems with arthrofibrosis. Our protocol included aggressive return to the operating room for manipulation and lysis of adhesions, as needed, if patients failed to achieve at least 90° of flexion and 10° or fewer of extension within 2 months of their initial operation. When patients were evaluated for final range of motion, clinical stability, Lysholm knee score, and return-to-activity status, there was no significant difference between patients with arthrofibrosis and those without.
There were two intraoperative complications that occurred in patients in our study. One patient had a laceration to a large branch of the popliteal vein that required vascular consultation and eventual ligation with no additional sequelae. The other patient experienced a failure of fixation of the bone block from the tibial-inlay procedure with fracture of the block. This patient had a revision of his allograft successfully accomplished and has had an outstanding clinical outcome. The PCL reconstruction of one patient failed 6 months after his initial procedure. The clinical course before reconstruction failure was complicated by an infection that required numerous surgical irrigations and debridements. He underwent revision PCL reconstruction with use of our technique and has had an excellent final clinical result. Three of the 30 knees developed infections, all of which resolved with surgical irrigation and debridement. One patient developed a second infection after a grossly contaminated open fracture-dislocation. His reconstruction was delayed for 8 weeks to allow healing of the soft tissues and resolution of his initial infection. Another patient developed a superficial wound infection that resolved with irrigation and debridement and administration of oral antibiotics. When these patients were analyzed separately, there were no significant differences in range of motion, clinical laxity, Lysholm score, and return to activity status. Seven patients demonstrated some formation of heterotopic bone.
A number of our patients sustained associated injuries, including ipsilateral fractures and injuries to the peroneal nerve or vascular structures. Patients in this study sustained 16 fractures of the ipsilateral extremity, including 6 femoral fractures, 5 tibial plateau fractures, 3 acetabular fractures, and 2 tibial shaft fractures. When the knees were analyzed for range of motion, it was noted that, of the seven knees with flexion less than 120°, four were in patients who had ipsilateral fractures, and two of these had range of motion of less than 100°. There was a significant difference in the median Lysholm knee score between patients with ipsilateral fractures (88.5) and those without (97), with a P value of 0.047 as determined by the Kruskal-Wallis test. There was also a significant difference between these two groups when analyzed for return to work status (P = 0.049) and return to sports (P = 0.025) by the Fisher's exact test. There was no significant difference between patients with peroneal nerve or vascular injuries and those without when analyzed for range of motion, clinical stability, Lysholm knee score, and return-to-activity status.
Lysholm knee scores were obtained at the most recent follow-up for 23 of the patients’ knees. The mean score was 89.4. Two patients had scores of 70 or less, including one who has not yet had her ACL reconstructed. Seventeen patients had excellent outcomes with a score of 90 or higher.
Nineteen patients with 20 PCL reconstructions have been observed for more than 2 years. Analysis of these patients’ outcomes confirms that the stability of the reconstruction has been maintained with no significant change in range of motion or Lysholm knee score. This group of patients had a mean of 28.4 months of follow-up (range, 24 to 39), a mean Lysholm knee score of 88.1, and a mean range of motion of 1.6° to 122.9°. Sixteen of these knees had a clinical stability grade of 0, and four had a grade of 1 +. None of the outcomes for this group was significantly different from those of the entire study group.
Short Form-36 patient outcome surveys have been completed sequentially by all of our patients during their rehabilitation. The mean physical component summary score for our patients was 37.4. The mean mental component summary score was 49.1. The mean physical component summary score for those patients whose follow-up was less than 24 months was 34, compared with a mean score of 39 for patients with more than 24 months of follow-up. Work status was obtained from all 29 of our patients. Of these, 24 have returned to full-time work; 3 have returned to light duty and the remaining 21 patients returned to full duty in their previous occupation. Five patients have been unable to return to work. Sixteen patients returned to their previous level of recreational activity, 12 returned to a diminished level of activity, and 1 became sedentary.
Discussion
Posterior cruciate ligament tears, whether treated operatively or nonoperatively, are severe injuries that are often associated with poor outcomes.1,6,11,12,16,23,24,26-28,30,32,34 The results are even less favorable in knees with multiple ligament injuries.4,13,14,32 Similarly, worse outcomes are associated with PCL tears that result from high-energy trauma when compared with those that result from athletic injuries. 13 Nonoperative treatment has been associated with significant problems, including laxity, knee pain, difficulties with activities of daily living, difficulty climbing stairs, and significant degenerative changes on radiographs.4,11,15,20,24,30 Surgical results are often less than outstanding. Repair of midsubstance tears has been attempted, resulting in 78% to 100% laxity on stability examinations.1,27 Single-incision reconstruction with a transtibial tunnel is advocated by many authors; however, it is common to have mild-to-moderate instability as a result of this procedure.6,12,16,23,26,28 For example, Noyes and Barber-Westin 23 reported that 40% of their patients with early PCL reconstructions and 63% of those with late PCL reconstructions had at least 6 mm of laxity on KT-1000 arthrometer examinations. Similarly, Franklin et al. 16 reported an average side-to-side difference of 3.6 mm for 23 patients after PCL reconstruction. Using clinical examination to measure stability, Schulte et al. 28 noted that nearly 50% of their patients had 1+ to 2+ laxity on final outcome.
Anatomic studies of the PCL have clearly documented at least two distinct functional bundles.10,14,18,28 The anterolateral bundle is the larger of the two and provides maximum stability in flexion but is less taut in extension. The posteromedial bundle is smaller but provides maximum stability as the knee approaches extension.7,10,14,18,25,28,32 Most reconstruction techniques re-create the anterolateral bundle, and the graft is tensioned at nearly 90° of knee flexion. However, most functional activities are performed with the knee in significantly less flexion. Reconstruction of only the anterolateral bundle may result in cyclic fatigue and lengthening of the graft. 7 Two-tunnel techniques of PCL reconstruction have been developed that allow tensioning of the separate bundles.7,25 Petrie and Harner 25 have obtained kinematic data that show reduced posterior tibial translation at all flexion angles with the two-tunnel technique when compared with the single-tunnel technique.
Single-incision arthroscopic reconstruction techniques that employ a transtibial tunnel require the graft to turn a corner at an acute angle that can approach 140°.2,9,21,32 This killer turn, as well as the length of graft traversing the tibial tunnel, places the graft at potential risk for abrasion that may result in ligament rupture or stretching. 2 The tibial-inlay technique has been developed to address this problem and eliminate the acute graft angle by using a bone block fixed in a cancellous trough on the back of the tibia at the point of insertion of the PCL.2,9,21,32 Bone-tendon-bone autografts or allografts are generally used.2,9,21,32 This technique requires an open approach to the posterior aspect of the proximal tibia. The graft also enters the femoral tunnels at an angle, but we do not believe this angle poses a similar risk of abrasion and laxity for two reasons. The first is that the killer turn in the tibia forms a far more acute angle than in the femoral tunnel. The second reason is that the graft actually incorporates into the femoral tunnel at the point where the angle is formed, whereas it does not incorporate at the killer turn and is free to abrade and stretch. We placed the absorbable interference screws used for fixation in the femoral tunnels as close to the intraarticular edge of the tunnels as possible, to minimize abrasion.
In an attempt to re-create the anatomy of the PCL, we have developed a reconstruction technique that combines the tibial-inlay with the two-femoral-tunnel technique. This procedure allows us to eliminate the killer turn while re-creating the two functional bundles of the PCL with tensioning at different angles of knee flexion. An Achilles tendon allograft is an ideal tissue for combining the tibialinlay with the two-femoral-tunnel technique by using a single graft source.
Stability after use of conventional PCL reconstruction techniques has been fair to poor. Eighty percent of our patients achieved an excellent clinical stability result with a grade of 0 on their most recent examination. The remaining 20% had 1+ laxity. The results of KT-2000 arthrometer evaluations have been even more impressive, with the majority of patients demonstrating a slightly tighter knee in terms of posterior translation on the injured side compared with the uninjured side. Similarly, the side-to-side comparison for total AP displacement confirms the excellent stability achieved with the anatomic reconstruction. These results have been observed in patients with multiligament knee injuries resulting from high-energy trauma, despite an aggressive rehabilitation protocol that featured early motion. There was no difference in rehabilitation protocol among patients regardless of their associated injuries, with the exception of weightbearing status.
Many studies in the literature report a loss of terminal flexion of 10° to 20° after PCL reconstruction.18,23 Our patients achieved a mean flexion of 124°, with many having difficulty achieving the final portion of terminal flexion. Full extension was achieved in 26 of 30 (87%) knees. Motion is often a problem among patients with multiligament knee injuries. All of our patients had multiple ligaments torn, with nearly all of them having Cooper grade III or higher injuries. As has already been noted, trauma patients frequently have a less favorable outcome, including less range of motion. 13 Our patients often had multiple injuries, including ipsilateral skeletal injuries. Patients with ipsilateral fractures had a less favorable outcome in terms of Lysholm knee score, return to work, and return to activity. However, there was no difference in terms of range of motion or stability of the PCL.
Additionally, many of our patients were uninsured and had problems obtaining physical therapy during the rehabilitation period. Although the incidence of arthrofibrosis or motion problems was higher than we would like, it is comparable with or lower than that reported for many series of multiligament knee injuries.22,29,31 With aggressive treatment we have successfully obtained functional motion in our patients who have developed arthrofibrosis.
Posterior cruciate ligament tears associated with multiligament knee disruptions represent a catastrophic injury. Our SF-36 outcome data document the severity of the injury but also demonstrate significant improvement with long-term rehabilitation and increasing time from injury. Similarly, Lysholm knee scores demonstrated improvement with increasing duration of time from injury, with 70% demonstrating good or excellent results.
The tibial-inlay technique is technically challenging. We had two intraoperative complications during our early experience. Our only vascular problem was a tear of a large branch from the popliteal vein. Vascular consultation was obtained and the vein was ligated. We also had one failure of a bone block when it cracked and split around the fixation screw at the end of the reconstruction. A technical error of undersizing the bone block caused the complication. This case was salvaged by obtaining a new Achilles tendon allograft and repeating the reconstruction. We have had no other complications that are unique to our reconstruction technique. One of our patients’ PCL graft stretched out in the first 6 months after reconstruction. He had a significant infection that may have contributed to the failure. He was treated with a repeat reconstruction and has had a very successful result.
Conclusion
We have developed a reconstruction technique that combines two contemporary techniques and more precisely re-creates the anatomy of the PCL. An obvious weakness of our study is that our follow-up was relatively short, and late failure of the grafts remains a possibility. However, our study has a number of strengths as well. It represented a population of patients that frequently have poor outcomes (trauma, multiple ligament injuries). Additionally, all of the operations were performed by a single surgeon (JPS) with use of a single surgical technique. Our results to date have been very encouraging. Our patients have achieved outstanding stability after their PCL reconstructions. Motion has been a challenge, but the mean final range of motion has been good. Patient outcomes have been sequentially improving with time in terms of SF-36, Lysholm knee scores, and functional outcome. We recommend the combination of the tibial-inlay and two-femoral-tunnel techniques for PCL reconstruction. This method re-creates the normal anatomy more precisely than other techniques. Longer-term results are clearly needed, and we plan to continue to observe our patients carefully.