
Abstract
Background: The role of arthroscopic repair in the treatment of posterior shoulder instability remains poorly defined.
Purpose: To evaluate the results of arthroscopic repair of posterior Bankart lesions.
Study Design: Retrospective review.
Methods: Records were reviewed of 27 shoulders (26 patients). All of the patients were male with a mean age of 28.7 years; in all cases symptoms were preceded by a traumatic event. Fourteen of the patients had 2+ to 3+ posterior translation noted under preoperative anesthesia. The posterior capsulolabral complex was found to be detached from the glenoid rim in all cases; bioabsorbable tack fixation was used for repair.
Results: At a mean follow-up of 5.1 years, no patients demonstrated a range of motion deficit. Muscle weakness (grade 4/5) in external rotation was noted in two patients (8%). There was no instability greater than 1+ in the anterior, posterior, or inferior directions. The mean L'Insalata shoulder score was 90.0 ± 13.9. The mean SF-36 physical and mental component scores were 50.4 ± 7 and 53.9 ± 9, respectively. Symptoms of pain and instability were eliminated in 24 patients (92%). Two patients (8%) required additional surgery after arthroscopic repair of the posterior Bankart lesion. Radiographs demonstrated that there had been no progressive glenohumeral joint degeneration.
Conclusions: Arthroscopic repair of the posterior capsulolabral complex is an effective means of eliminating symptoms of pain and instability associated with posterior Bankart lesions of traumatic origin.
The posterior Bankart lesion has been described as the detachment of the posterior capsule and labrum below the glenoid equator. This lesion has also been described as an etiologic factor in the development of shoulder pain, dysfunction, and instability. 18 The posterior Bankart lesion usually occurs after pathologic posterior translation of the humeral head in relation to the glenoid surface. It is seen less frequently than the anterior glenoid Bankart lesion. 16 Mair et al. 16 described a series of cases in which contact athletes underwent shoulder arthroscopy to repair the posterior capsule and labrum. The authors hypothesized that these athletes, predominantly football and lacrosse players, were at particular risk of developing this injury because of the high-energy extrinsic forces that were typically directed posteriorly to the athlete's outstretched arm. 16
Posterior shoulder instability includes a continuum of disorders and remains a poorly understood clinical problem. In general, symptomatic posterior shoulder instability is a condition in which symptoms are caused by an abnormal posterior translation of the humeral head relative to the glenoid surface. Posterior dislocation and recurrent subluxation can cause pain and symptoms of instability and may be associated with a posterior Bankart lesion (frank detachment of the posterior inferior capsulolabral complex), posterior capsular laxity, or both. 25 Although rehabilitation of the shoulder musculature remains one of the primary methods of treating patients with symptomatic posterior glenohumeral instability, surgical reconstruction of the capsulolabral complex may be necessary if shoulder symptoms persist. 7 Most of the surgical techniques for treatment of symptomatic posterior capsulolabral lesions involve direct repair of posterior Bankart lesions to the glenoid rim in combination with various capsulorrhaphy techniques.3,12,26 The role of arthroscopic repair in the treatment of posterior instability, however, remains poorly defined. Two studies have reported successful arthroscopic treatment for posterior instability.16,18 The clinical results of these studies suggest that arthroscopic posterior capsulolabral repair is an effective method of treating select patients with shoulder pain and symptoms of instability associated with posterior Bankart lesions of traumatic origin.
The hypothesis of this study was that arthroscopic repair of the detached posteroinferior capsulolabral complex is an effective means of relieving pain and symptoms of instability associated with traumatic posterior shoulder instability. To investigate this premise, we evaluated the clinical results of arthroscopic repair of symptomatic, posteroinferior capsulolabral complex lesions in a series of patients who came to our institution seeking treatment for traumatic glenohumeral avulsion injuries of the shoulder and posterior instability.
Materials and Methods
We retrospectively reviewed the cases of patients who underwent arthroscopic repair of a posterior capsulolabral detachment (posterior Bankart lesion) between 1989 and 1998. Twenty-seven shoulders in 26 patients were included in the study. Patients with concomitant anterior instability or patients who had undergone previous or concomitant capsular stabilization procedures were excluded.
All patients were examined by a single orthopaedic surgeon (RJW). The criteria for follow-up evaluation consisted of physical examination results, functional scores (L'Insalata shoulder rating score 15 and SF-36 physical and mental component score 17 ), subjective satisfaction questionnaire, and radiographs (AP and axillary views).
Demographic Data and Preoperative Findings
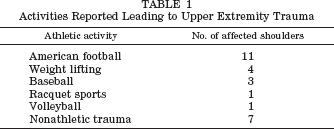
All 26 patients (27 shoulders) were male with a mean age of 28.7 years (range, 15 to 55). All 26 patients reported a specific traumatic event that occurred before onset of their symptoms: 18 reported a fall on the outstretched arm; 5, a direct blow to the shoulder; and 4, a subluxation event. The most common athletic activities associated with these injuries are shown in Table 1.
Activities Reported Leading to Upper Extremity Trauma
The most common symptoms were pain, weakness, and mechanical symptoms (catching, clicking, clunking). Three patients (12%) had a history of at least one documented instance of posterior dislocation that required closed reduction. The remaining 23 patients (24 shoulders) had symptoms of subluxation (clicking, catching, a sense of “looseness”) with activities of daily living or athletics.
Preoperative medical records revealed that all 26 patients had full range of motion (forward flexion, abduction, internal rotation, external rotation) compared with motion in the unaffected normal shoulder. In the patient with both shoulders affected, there was no difference in shoulder range of motion between the two sides. The posterior load and shift test (posteriorly directed force on the arm, with the arm positioned at 90° of forward flexion) was positive (eliciting pain) in 23 of the 27 shoulders (Fig. 1). No patient had gross posterior, anterior, or inferior (sulcus sign) shoulder instability (≥2+) on supine testing (with the patient awake) in the affected or contralateral extremity. Preoperative radiographic findings for the 27 shoulders were as follows: a bony posterior Bankart lesion alone (one patient), reverse Hill-Sachs lesion alone (one patient), and a bony posterior Bankart lesion in conjunction with a reverse Hill-Sachs lesion (two patients).

The posterior load and shift test. The examiner stands at the side the patient; the scapula of the affected upper extremity is stabilized. The affected arm is forward flexed to 90° and internally rotated. A posteriorly directed force is then applied by the examiner. A positive test is characterized by the elicitation of pain or a mechanical grind, or both, on performance of the maneuver. The load and shift test may also be performed with the patient in the supine position. The patient's torso should lie just off the examination table such that the medial scapula is stabilized by the table's edge. The load and shift maneuver is then performed as described above.
The mean interval from injury to surgical repair was 2.4 years (range, 2 weeks to 16 years). Before surgery, 25 of 26 patients participated for a minimum of 2 weeks (range, 2 weeks to 14 months) in a physical therapy regimen to strengthen the periscapular and rotator cuff musculature. Early in this study, we began treating patients whose nonoperative treatment failed with diagnostic shoulder arthroscopy with possible labral repair. This course of treatment was based on the presence of shoulder symptoms for at least 6 months. In 3 of the 27 cases, patients underwent arthroscopic posterior Bankart repair within 6 months of injury; each of these patients was an elite-level athlete whose diagnosis had been made by physical examination and MRI.
Operative Findings
Before surgery, we examined the affected shoulder with the patient under anesthesia. The results of supine posterior stability testing are shown in Table 2. Anterior shoulder instability of the affected shoulder was less than 1 + in all patients; the sulcus sign was less than 10 mm in all patients. There was a 1+ grade of translation in the anterior, posterior, and inferior directions in the contralateral shoulder of all 26 patients.
Grading of Glenohumeral Translation
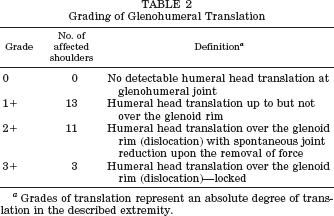
Grades of translation represent an absolute degree of translation in the described extremity.
All patients underwent shoulder arthroscopy in the beach-chair position with regional anesthesia. Typically, two portals were used for arthroscopic posterior Bankart repair. A single posterior portal was created 2 cm inferior and medial to the posterolateral corner of the acromion process. An accessory anterior portal was created 1 cm lateral and superior to the coracoid process, within the rotator interval. A systematic evaluation was conducted of the articular surfaces, rotator cuff tendons, biceps tendon, axillary recess, and of the structural integrity of the capsuloligamentous structures (superior, middle, and inferior glenohumeral ligaments) and labrum. Particular attention was paid to the posteroinferior glenoid and capsule, which was viewed with the arthroscope placed in the accessory anterior portal. A large-bore screw-in cannula was placed in the posterior portal. The posterior capsulolabral complex was found to be detached from the glenoid rim in all 27 shoulders. The area of injury was characterized as a posterior soft tissue Bankart lesion; the capsulolabral complex remained intact (no splits or tears of the labral tissue). When compared with a standard clock face, the posterior capsulolabral complex was detached from the glenoid rim at the 6- to 10-o'clock position in affected right shoulders and at the 2- to 6-o'clock position in affected left shoulders (Fig. 2). There were no tears or visible disruption of the posterior capsule or posterior band of the inferior glenohumeral ligament. The origin of the long head of the biceps tendon at the supraglenoid tubercle was not involved in any patient. There were three patients in whom bony fragmentation (posterior glenoid erosion) was noted at the site of the posterior Bankart lesion; however, no gross glenoid surface deficits were observed. Two patients had a gross reverse Hill-Sachs lesion noted at the anterior humeral head. No occult hyaline cartilage lesions were noted. There were no rotator cuff tears.
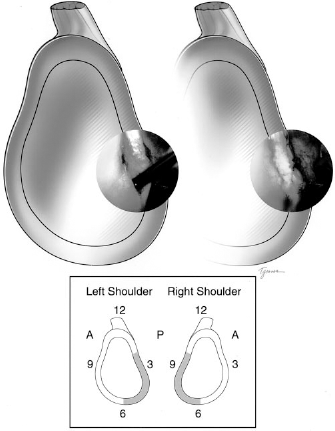
The preoperative and postoperative condition of a repaired posterior Bankart lesion in a left shoulder. Two bioabsorbable tacks were used. The drawing demonstrates (in gray shade) those areas typically affected by a posterior Bankart lesion. The numbers about the glenoid correspond to typical clock-face numbers. A, anterior; P, posterior.
The posterior capsulolabral repair was performed with the arthroscope placed anteriorly through an accessory anterior portal created in the rotator interval. After bony debridement to a bleeding bed of bone on the posterior glenoid rim, we reattached the capsule and labrum to the glenoid margin using bioabsorbable tack fixation (Sure-Tac, Acufex Microsurgical, Andover, Massachusetts). Two to three tacks were used for each labral repair (Fig. 2). If necessary, an accessory posteroinferior portal was created to facilitate capsulolabral repair near the 6-o'clock position on the glenoid rim. 5
Concomitant Procedures
Two patients underwent concomitant arthroscopic subacromial decompression (acromioplasty) at the time of posterior Bankart repair; these patients had demonstrated positive preoperative impingement signs and at surgery were noted to have anatomic findings consistent with this condition (frayed coracoacromial ligament and thickened subacromial bursa). One patient underwent a concomitant subacromial bursectomy.
After surgery, patients wore a sling for 3 to 4 weeks; during this initial healing phase, they began performing Codman's exercises, scapular protraction exercises, and elbow and wrist exercises. Subsequently, a regimen of physical therapy was instituted that focused on reestablishing glenohumeral range of motion and rotator cuff and periscapular muscle strength. Patients were allowed to return to activities as tolerated at 4 to 5 months. Contact sports were not allowed for 6 months.
There were no perioperative or long-term complications associated with these arthroscopic repair procedures.
Results
Follow-up Examination
The mean interval from surgery to follow-up examination was 5.1 years (range, 2.0 to 11.7). Follow-up examination consisted of range of motion testing, supine stability testing, active compression (O'Brien's) test, apprehension test, posterior load and shift test, and muscle strength testing. 20
Physical Examination
Range of Motion Testing
Forward flexion, abduction, internal rotation (measured at 0° and 90°), and external rotation (measured at 0° and 90°) were assessed. The range of motion was full (within 10° of that of the unaffected shoulder) for all shoulders. No abnormalities in motion were noted.
Muscle Strength Testing
In all patients, testing of the supraspinatus, subscapularis, deltoid, pectoralis major, biceps, and triceps muscles demonstrated full motor strength (grade 5/5). Isolated external rotation weakness (grade 4/5), representative of infraspinatus or teres minor muscle weakness, was noted in two patients (8%). One of these two patients had undergone a subsequent open posterior stabilization after the arthroscopic repair. The second patient had undergone arthroscopic repair alone 36 months before the follow-up examination. Full motor strength in external rotation (grade 5/5) was observed in the remaining 25 shoulders (93%).
Stability Testing
Supine stability testing (anterior and posterior) with the patient awake demonstrated no differences between unaffected and operated shoulders in any of the 26 patients (27 shoulders); no patient had an instability grade of greater than 1+ in either shoulder at follow-up. The sulcus sign was less than 10 mm in all shoulders.
Special Tests
The apprehension and relocation tests were negative in all 27 shoulders. The active compression test (O'Brien's test) was negative in all 27 shoulders. The posterior load and shift test was positive (producing pain) in 2 of 27 shoulders.
Functional Outcome
The L'Insalata shoulder questionnaire and SF-36 (physical and mental component scores) were used to assess functional outcome at the time of follow-up examination.15,17 The mean L'Insalata score (maximum 100 points) was 90 ± 13.9 (range, 50 to 100). The mean SF-36 physical component summary score was 50.4 ± 7 (range, 37 to 61); the mean SF-36 mental component score was 53.9 ± 9 (range, 31 to 63). The mean SF-36 physical and mental component score is 50 for normal healthy subjects. 17
Subjective symptoms of pain and instability were eliminated in 24 patients (92%; 25 shoulders). These 24 patients were able to return to unlimited athletic activity by 6 months after surgery. Overall satisfaction was high, as reflected by 25 patients (96%) responding that they found the procedure effective and would undergo the surgery again for the same clinical problem.
Clinical Failures
In two patients (8%), arthroscopic posterior Bankart repair failed and further surgery was required. One of the two patients, who had a known prior posterior dislocation and was one of the three patients with a posterior instability grade of 3 + noted under anesthesia, reported symptoms of persistent instability after arthroscopic stabilization and postoperative physical therapy. Open posterior stabilization (capsulorrhaphy) was performed 12 months after the initial arthroscopic repair; the open procedure eliminated the symptoms of pain and instability. The second patient, a professional baseball player, reported persistent mechanical symptoms (a clunk) with throwing and batting activities; these symptoms began approximately 8 months after arthroscopic posterior Bankart repair. Magnetic resonance imaging demonstrated persistent posterior labral detachment. This patient underwent a second shoulder arthroscopic procedure (labral debridement) 13 months after the initial capsulolabral repair. He was able to return to professional competition but still reported occasional pain with athletic activity at follow-up.
Radiographic Examination
For each patient, AP and axillary radiographs were obtained and evaluated by a single radiologist without knowledge of patient identity or date of the radiograph being examined. Preoperative and follow-up radiographs were available for all patients and were assessed for the presence of progressive degenerative changes of the glenohumeral joint and scored by using the criteria in Table 3.
Criteria for Assessment of Follow-Up Radiographs
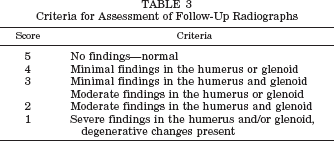
Anteroposterior radiographs were evaluated in terms of amount of joint space and the presence of subchondral sclerosis, subchondral cysts, osteophytes, surface erosion, and humeral head subluxation (superior or inferior). Axillary radiographs were evaluated for amount of joint space, presence of subchondral sclerosis, subchondral cysts, osteophytes, surface erosion, glenoid version, humeral head subluxation (anterior or posterior), reverse Hill-Sachs lesions, and posterior bony Bankart lesions. The maximum possible score was 5; the minimum possible score was 1. A summary numeric score including results of both radiographs was made in each case.
The mean radiographic score for preoperative radiographs was 3.96 ± 0.7 (range, 1 to 5). The mean radiographic score for follow-up radiographs was 3.71 ± 0.9 (range, 2 to 5). There was no significant difference between the radiographic scores of preoperative and postoperative radiographs, as indicated by use of the Student's two-tailed t-test (P > 0.05). Examination of follow-up radiographs demonstrated that those same shoulders that had demonstrated bony abnormalities of the posterior glenoid rim or anterior humeral head remained unchanged. At follow-up examination, a bony posterior Bankart lesion alone (one patient), reverse Hill-Sachs lesion alone (one patient), bony posterior Bankart lesion and reverse Hill-Sachs lesion (two patients) were noted (Fig. 3).
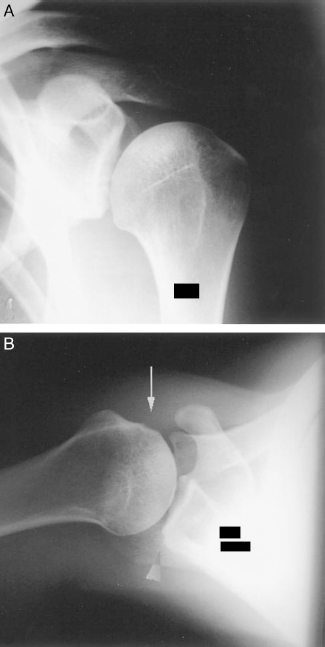
Follow-up radiographs (AP [A] and axillary [B] views) of a patient who underwent arthroscopic posterior Bankart repair 36 months previously. Of note are the presence of a posterior bony Bankart lesion (arrowhead) and reverse Hill-Sachs lesion (solid arrow).
Discussion
This study demonstrates that arthroscopic repair of the capsulolabral complex is an effective method of eliminating the symptoms of traumatic posterior shoulder instability associated with a posterior Bankart lesion in select patients.
Posterior shoulder instability remains a difficult clinical problem because both diagnosis and management can be difficult for even the most experienced clinician. Historically, most authors have advocated the use of extensive nonoperative measures for the treatment of symptomatic posterior shoulder instability.4,6,11,23–25 In patients in whom nonoperative measures fail, a myriad of open surgical procedures, including posterior capsulorrhaphy, bone-block procedures, glenoid osteotomy, humeral osteotomy, or a combination of these, have been described, with good-to-fair results.7,8,10,13,14,19,22,28 However, the role of arthroscopy remains less well defined. Arthroscopic methods of treatment for posterior instability include capsular plication, capsulolabral repair, and thermal shrinkage.1,9,16,30 Previous studies from this institution have demonstrated that bioabsorbable tack fixation is an effective means of treating anterior shoulder pain and instability caused by superior labral injuries and anterior Bankart lesions, respectively.21,27 In the current study, we sought to define our clinical experience in the repair of isolated detachments of the posterior capsulolabral complex (posterior Bankart lesions) with use of a bioabsorbable tack.
All 27 shoulders reviewed in this study were characterized by a symptomatic posterior Bankart lesion. Overwhelmingly, the most common complaint of patients was pain with athletics and activities of daily living. This is consistent with the findings of Tibone and Bradley, 29 who described a group of 40 athletes with a diagnosis of symptomatic shoulder subluxation. Although the pathologic cause of subluxation was posterior capsular laxity, the authors noted that the diagnosis is difficult to make because most patients report pain rather than apprehension or frank instability. Mechanical symptoms (clicking, clunking) were also common. The patients reviewed in our study each experienced an identifiable traumatic episode that resulted in the development of the described symptoms. Thus, we hypothesize that a single episode, either alone or superimposed on cumulative trauma, led to excessive posterior humeral head translation that resulted in the detachment of the posterior capsulolabral complex. Mair et al. 16 described the clinical results in nine patients who were unable to participate in sports because of symptomatic posterior instability resulting from athletic trauma. In that study, they repaired the posterior labral lesion with a bioabsorbable tack. At a minimum 2-year follow-up, all patients reported the elimination of pain symptoms and a return to competitive athletics. Mair et al. suggest that posteriorly directed vector forces (along the glenoid face), which occurred with athletic trauma, resulted in posterior capsulolabral detachment, without the development of capsular laxity. 16 Our results are comparable with those of Mair et al., in that 92% of the patients in our study were successfully treated and required no further treatment after arthroscopic stabilization.
An assessment of capsular laxity is important in the successful treatment of patients with posterior capsulolabral lesions. In this study, no gross disruption or tears of the posterior capsuloligamentous structures were observed. However, it is probable that some plastic deformation of the posterior capsule was present to allow abnormal posterior humeral head translation.2,3 Antoniou and colleagues 1 described a method of arthroscopic capsulolabral augmentation for the treatment of posteroinferior instability of the shoulder in 41 patients. Capsular laxity (a posteroinferior capsular recess) was observed in all patients; five patients had frank posterior labral detachment. Superomedial capsular plication was performed with absorbable (polydioxanone) suture. At a mean follow-up of 28 months, significant increases in the mean simple shoulder test and SF-36 scores were demonstrated; 85% of patients were satisfied. Although the patient groups in our current study and that of Antoniou et al. are different, the clinical results of both studies suggest that reestablishing a labral buttress and competent posterior band of the inferior glenohumeral ligament complex effectively reduces symptoms in patients with isolated posterior instability.
Fourteen of 27 patients (52%) in our study demonstrated posterior humeral head translation that was 2+ or greater under anesthesia. Interestingly, two of three patients with 3+ posterior humeral head translation were successfully treated by posterior capsulolabral repair alone. We do not recommend arthroscopic posterior labral repair alone for patients with recurrent posterior glenohumeral instability associated with a large posterior capsular recess. However, the clinical success of those patients with 3 + translation does suggest that reattachment of the labrum at the level of the posteroinferior glenohumeral ligament provides symptomatic relief. Studies from our institution suggest that the posterior band of the inferior glenohumeral complex is a static restraint to posterior glenohumeral translation from 30° to 90° of arm abduction. 20 Thus, detachment of the capsule and labrum at the area delineated by the posterior Bankart lesion would compromise the function of this static restraint and result in abnormal posterior humeral head translation. Therefore, restoration of the posterior labral buttress and tension in the posterior band of the inferior glenohumeral ligament complex likely resulted in a net decrease of posterior humeral head translation and the marked reduction of symptoms noted in patient groups described here and by Antoniou et al. 1
Because of the retrospective nature of this study, no preoperative functional scores could be calculated. The L'Insalata and SF-36 scores suggest that all 26 patients experienced excellent outcomes at a minimum 2-year follow-up interval. Overall satisfaction was high (92%), and symptoms were ultimately eliminated in 25 of 27 shoulders. The remaining two shoulders underwent additional surgery (arthroscopic debridement and open posterior capsulorrhaphy) to resolve symptoms of instability and pain.
Examination of radiographs demonstrated that there was no significant degenerative progression from surgery to follow-up over the mean 5.1-year follow-up interval. Although some degenerative findings were noted on preoperative radiographs, a blinded examiner was unable to note any changes from preoperative radiographs to those made at follow-up. These data suggest that arthroscopic posterior stabilization does not predispose the glenohumeral joint to degenerative change at a minimum 2-year follow-up.
We now routinely use MRI to aid in the diagnosis of posterior labral injuries (Fig. 4). Early in the study interval, the diagnosis of instability associated with a posterior Bankart lesion was made by physical examination and history. In 24 cases, the injury history, physical findings, and lack of symptomatic improvement over time ultimately led to shoulder arthroscopy for the surgical treatment of posterior glenohumeral instability. Three patients underwent arthroscopic repair within 6 months of injury; each of these patients had MRI scans that demonstrated a posterior Bankart lesion. Although we recommend physical therapy as a primary treatment modality for the majority of patients with symptomatic posterior instability, the decision for operative repair should take into consideration the patient's degree of disability and desired level of activity.
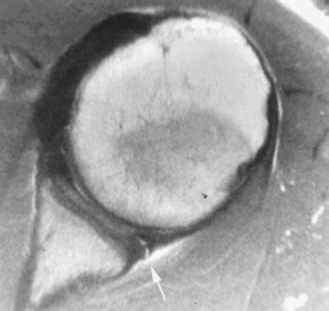
Magnetic resonance image (axial) demonstrating a posterior capsulolabral detachment from the glenoid rim (white arrow).
In this study, the observed morbidity for arthroscopic posterior labral repair was extremely low. There were no perioperative complications. The only significant follow-up finding was the external rotation weakness (4/5) that was observed in 2 of 26 patients (8%). There were no problems observed with range of motion of the operative extremity at follow-up examination.
The patient group described in this study is unique in that all of the patients had a history of a distinct traumatic episode, the presence of a posterior Bankart lesion, and minimal posterior capsular laxity. Therefore, although we describe the effectiveness of arthroscopic posterior capsulolabral repair, we also acknowledge the specific clinical circumstances unique to these patients. Capsular tension and competency of the posterior band is crucial to all posterior stabilization techniques. Thus, we recommend a thorough assessment of all etiologic factors, including the degree of capsular laxity, before proceeding with an isolated posterior capsulolabral repair.
Summary
Arthroscopic repair of the capsulolabral complex is an effective means of relieving symptoms of pain and instability associated with a posterior Bankart lesion. The select group of patients described in this study had a traumatic avulsion of the posterior capsulolabral sleeve from the glenoid rim (posterior Bankart lesion) and minimal-to-no capsular laxity. Arthroscopic repair of the capsulolabral complex eliminated pain and instability symptoms in 25 of 27 shoulders (93%). The procedure was successful despite the inclusion of 14 shoulders found to have 2+ to 3+ posterior humeral head translation at the time of surgery. Functional scores obtained through the use of validated outcome measures were excellent. Radiographic examination demonstrated no degenerative progression after arthroscopic posterior capsulolabral repair.