
Abstract
Background: Large bucket-handle meniscal tears in knees with chronic anterior cruciate ligament deficiency have been considered avascular and, thus, irreparable.
Hypothesis: The rate of meniscal healing is higher than previously reported.
Study Design: Prospective cohort study.
Methods: Fifty-nine patients underwent staged surgical procedures of meniscal repair followed at an average of 77 ± 58 days by ligament reconstruction once full range of motion was obtained.
Results: Fifty-two patients with 55 meniscal repairs were available for follow-up. At reconstruction, 30 menisci (55%) appeared healed; 19 (34%), partially healed; and 6 (11%) showed no healing (only 4 were removed). Of 43 tears in the white-on-white zone, 21 appeared healed; 17, partially healed; and 5 showed no healing. Of 11 in the red-on-white zone, 8 appeared healed; 2, partially healed; and 1 showed no healing. One meniscal tear in the red-on-red zone appeared healed. At an average follow-up of 4.3 ± 3.1 years, 36 of the 43 (83.7%) white-on-white meniscal repairs remained asymptomatic; all repairs in the other zones remained asymptomatic.
Conclusion: Locked bucket-handle meniscal tears heal at a high rate when repaired as an isolated procedure, even when full weightbearing and activity before reconstruction is allowed and when the tear is in the white-on-white zone.
Patients who have chronic ACL deficiency often seek treatment for their knee at the time when they experience debilitating symptoms and severe loss of knee extension from a locked bucket-handle meniscal tear that causes their previously acceptable knee symptoms to become disabling. These meniscal tears are large and usually involve the avascular zone and thus are thought to have a low potential to heal after repair.6,9,12 We routinely perform a two-staged procedure of meniscal repair and ACL reconstruction in patients from this unique population to avoid an increased likelihood of postoperative knee motion problems. 14 This approach allows us to evaluate meniscal healing and to determine the definitive treatment of the repaired meniscus.
The purpose of this study was twofold: 1) to evaluate arthroscopically the status of the meniscal repair at the time of ACL reconstruction and to determine what effect unrestricted range of motion and weightbearing during the postoperative period might have had on such a difficult tear and 2) to evaluate the long-term sequelae of repair with clinical follow-up and subjective evaluations.
Materials and Methods
Subjects
Between 1987 and 1999, the senior author (KDS) performed 1470 ACL reconstructions for chronic ACL injuries. Eighty-eight patients who had a locked bucket-handle meniscal tear that severely limited knee extension were seen for an initial evaluation. The diagnosis of displaced bucket-handle meniscal tear was made on clinical examination with or without an MRI scan. The average amount of knee flexion contracture at evaluation was 20° ± 10° from 0° of extension. The mean range of motion in the contralateral normal knee was from 6° of hyperextension to 140° of flexion. The patients underwent staged procedures of arthroscopic meniscal repair (59 patients) or removal (29 patients) followed by ACL reconstruction at a time when the patient had regained full knee range of motion and when it was suitable to the patient's athletic, school, or work schedule.
Surgical Procedure for Meniscal Repair
The average age of the patients at the time of meniscal repair was 22.6 ± 7.7 years (range, 14.4 to 53.3). The average time from injury to arthroscopic meniscal repair was 10 ± 8 days (range, 1 to 29). At the time of the initial arthroscopic procedure, a decision was made regarding the potential for the torn meniscus to heal with repair. If repair was chosen, an inside-out technique, as described previously, was used. 17 Before meniscal repair, the tear sites were prepared by debridement with or without trephination of the rim of the meniscus (Fig. 1). Trephination was performed by using a suture repair needle to stab approximately 20 holes through both sides of the meniscal tear and through the capsule to create vascular channels. Approximately three to six vertical mattress sutures (2–0 Ethibond, Ethicon, Inc., Somerville, New Jersey) were used. The zone of the tear was described and recorded as 1) red-on-red, both the peripheral rim and inner edge of the tear showed vascular bleeding; 2) red-on-white, the peripheral rim showed vascular bleeding but the inner edge of the tear did not have vascular bleeding; or 3) white-on-white, both the peripheral rim and the inner edge of the tear did not show vascular bleeding.
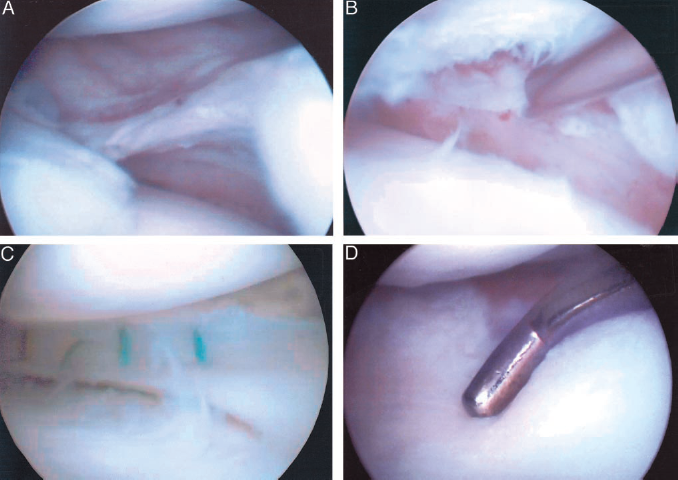
A, the white-on-white bucket-handle meniscal tear had no vascular bleeding on the rim or the inner surface of the tear; B, abrasion and trephination were performed to create vascular channels for healing; C, sutures were inserted for repair; D, at the time of ACL reconstruction (5 weeks after meniscal repair) the meniscus appeared to be healed.
Rehabilitation Program between Meniscal Repair and ACL Reconstruction
After meniscal repair, patients were instructed to remain on bed rest for 3 days, during which time the leg was kept elevated above the heart and a cold compression device was worn continuously to prevent postoperative hemarthrosis. At 3 days after surgery, the patients began range of motion exercises to regain full range of motion, and full weightbearing was allowed. Full knee range of motion equal to that of the noninvolved knee, which was our requirement for proceeding with ACL reconstruction, was achieved at a mean of 26.6 ± 13.6 days after meniscal repair. Quadriceps muscle-strengthening exercises, including stair-climbing, stationary bicycling, and isokinetic exercises were prescribed once full range of motion was achieved. If there was going to be a delay in ACL reconstruction, sports involving cutting maneuvers were restricted between the time of meniscal repair and the ACL reconstruction.
Surgical Procedure for Second-Look Arthroscopy and ACL Reconstruction
The average time between meniscal repair and ACL reconstruction was 77 ± 58 days (range, 24 to 400). The time between meniscal repair and ACL reconstruction was less than 60 days for 25 of the 59 patients (42%) and between 60 and 90 days for 13 patients (22%). At the time of ACL reconstruction, a diagnostic arthroscopic examination was performed to evaluate healing of the meniscal repair. The meniscal repair was described as healed if the superior and inferior portions were confluent to probing throughout the entire length of the meniscus. The meniscal repair was considered partially healed if a portion of the superior or inferior portion of the meniscus or both was not confluent. The meniscal repair was considered not healed if the superior and inferior portions of the meniscus were not confluent to probing throughout the length of the meniscus. After the diagnostic arthroscopic procedure, a mini-arthrotomy ACL reconstruction was performed, 15 and the patient underwent postoperative rehabilitation as previously described. 16
Postoperative Evaluation
Patients were requested to return for long-term postoperative evaluation 2, 5, and 10 years after ACL reconstruction. Objective measurements included early and long-term range of motion and manual maximum side-to-side difference with KT-1000 arthrometer (Medmetric Corp., San Diego, California) testing. Knee range of motion was measured as the degree of hyperextension/the degree of extension short of 0°/the degree of flexion. Subjective evaluation was obtained yearly with a modified Noyes questionnaire, which contained a specific question asking if the patient had obtained a subsequent meniscectomy operation from another physician. If surgery was performed elsewhere, the patient's medical records were obtained.
Results
Fifty-two patients (38 men and 14 women) with 55 meniscal repairs (45 medial and 10 lateral) were available for follow-up. Of the repaired displaced bucket-handle meniscal tears, 43 were in the white-on-white zone, 11 were in the red-on-white zone, and 1 was in the red-on-red zone. At the time of ACL reconstruction, arthroscopic examination revealed that 30 menisci (55%) appeared healed, 19 menisci (34%) appeared partially healed, and 6 menisci (11%) showed no healing (Table 1). Of the six menisci with no signs of healing, three were removed, one was partially removed, and two were left in situ.
Status of Meniscal Repair Healing at Time of ACL Reconstruction
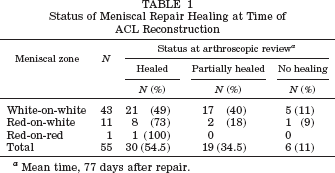
Mean time, 77 days after repair.
At an average follow-up of 4.3 ±3.1 years, four additional menisci (7%) were symptomatic and required meniscectomy for a failed repair; two of the tears were originally considered healed, one partially healed, and one not healed at the time of ACL reconstruction. All of these tears were of the medial meniscus in the white-on-white zone, and the time from repair to failure for the four patients was 1 year, 1.5 years, 1.8 years, and 10.5 years, respectively. From the time of meniscal repair, 36 of the 43 (83.7%) meniscal repairs in the white-on-white zone remained asymptomatic; all of the repairs in the red-on-white zone and red-on-red zone remained asymptomatic.
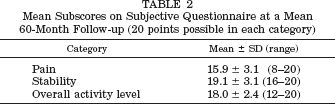
At a mean of 60 months, the average modified Noyes score was 89.9 ± 8.6 (range, 67 to 100). The average scores for the categories of pain, stability, and overall activity level are presented in Table 2. When comparing the patients’ current level of activity with that before their injury, 17% (9 of 52) had increased their level, 33% (17) had returned to their full level of work or sport, 44% (23) could participate in their same work or sport but at a lower level, and 6% (3) could participate in light recreational activities or work but had to be careful.
Mean Subscores on Subjective Questionnaire at a Mean 60-Month Follow-up (20 points possible in each category)
The average range of motion of the noninvolved knee was 6°/0°/140°. The average range of motion at 1 month after ACL reconstruction was 5°/0°/131°, and the range of motion at the latest follow-up was 5°/0°/140°. The mean KT-1000 arthrometer manual maximum side-to-side difference was 2.0 ± 1.0 mm (range, 0 to 4). Three patients had a 4-mm side-to-side difference. Two of these patients had had their medial meniscus resected at the time of ACL reconstruction. Other than the meniscal repairs that failed, there were no complications and no motion problems.
Discussion
The results of this study showed that, in the short-term (mean, 77 days), after isolated meniscal repair, only 6 of 55 (11%) menisci had not healed. These results were obtained with a rehabilitation program that did not restrict range of motion and weightbearing. Furthermore, at more than 4 years after surgery, only 7 of 55 menisci caused debilitating symptoms that required meniscal removal.
The meniscus has been shown to transmit 30% to 55% of the load across the knee joint; without it, load distribution is altered and increased wear and joint degeneration can result.3,8,10,19 Baratz et al. 2 showed that even partial meniscectomies resulted in marked changes in the loads transmitted to the joint surfaces. Therefore, preservation of the meniscus is desirable to preserve the integrity of the articular cartilage, whenever possible. Meniscal tears in the avascular white-on-white zone are thought to lack the ability to heal, and, therefore, many surgeons recommend excision. Some authors have suggested that only tears communicating with the periphery have the potential to heal.6,12,18 Studies show that the blood supply only penetrates the outer 10% to 30% of the medial meniscus and 10% to 20% of the lateral meniscus. In contrast, Rubman et al. 13 have shown that the majority of repaired meniscal tears that extend into the avascular segment remain asymptomatic at 2 years. Also, Asahina et al. 1 showed a 63% healing rate of locked bucket-handle meniscal tears in conjunction with ACL reconstruction. In our study, 59 of 88 patients (67%) with chronic ACL tears who had a locked bucket-handle meniscal tear underwent attempted repair. The decision to repair the meniscus was based on the ability to reduce the meniscus and not on the anatomic location of the tear. Henning et al. 9 defined the suitability of repair based on the ability to stabilize the configuration. By using this criterion, they were able to salvage the majority of menisci, many of the tears of which were in the white-on-white zone, and the menisci remained asymptomatic. Although longer-term studies are needed to determine whether these repaired menisci remain viable and if repair of these menisci decreases the rate of arthritis, repair of these bucket-handle tears may give the patient several more years of a functioning meniscus.
Patients who have a locked knee in addition to chronic ACL insufficiency seek care not because of the giving-way episodes but because their knee gave out again and this time did not return to normal. The severe loss of knee extension prevented the patients from doing simple activities of daily living. We believe that these patients are not necessarily seeking treatment to get their ACL reconstructed but instead because they want to return to the acceptable level of function they had before their recent injury. We know that the best thing for the patient's knee is to repair both the torn meniscus and reconstruct the ACL. However, one of our prerequisites for performing an ACL reconstruction is that the patient's knee must have full range of motion equal to that of the contralateral normal knee. Since we began to use this staged protocol for surgery, less than 1% of patients have required a subsequent operation for lack of range of motion after ACL reconstruction. Furthermore, when we performed both operations as an emergency, the procedures added two insults to an already inflamed knee, and patients were placed at an increased risk for developing problems with range of motion after surgery. 14
In a group of patients with chronic ACL deficiency and locked bucket-handle meniscal tears causing flexion contractures that were unresolved with physical therapy, 4 of 16 patients had severe difficulty obtaining full range of motion after surgery when they underwent simultaneous meniscal repair or removal and ACL reconstruction, compared with 0 of 16 patients who underwent staged procedures during which full range of motion was obtained after meniscal repair or removal and before ACL reconstruction. 14 By using a protocol that addressed the more emergent problem of a locked bucket-handle meniscus, we allowed patients the opportunity to regain knee motion as well as to prepare mentally, academically, and socially for an ACL reconstruction and subsequent rehabilitation.
One other study discussed the timing of meniscal repair and ACL reconstruction in patients with displaced bucket-handle meniscal tears. Costouros et al. 7 retrospectively compared the return of knee extension in patients who underwent simultaneous ACL reconstruction and meniscal repair with a control group of patients without displaced bucket-handle meniscal tears. The patients who underwent simultaneous procedures regained within –5° of extension 22% more slowly and 0° of extension 35% more slowly than the control group, but these numbers were not statistically significant. One cannot compare the study of Costouros et al. 7 with that of Shelbourne and Johnson 14 because the criteria for full range of motion was different between studies. Shelbourne and Johnson considered full range of motion to include full hyperextension of the knee, which has been shown to be 5° in men and 6° in women. In addition, the degree of preoperative knee flexion contracture in the patients of Costouros et al. was not described, whereas the mean amount of flexion contracture in the patients of Shelbourne and Johnson was 15° from 0°. It is possible for some patients to have small bucket-handle tears that are locked but cause the knee to lose only 5° of extension, and, in these cases, a simultaneous meniscal repair and ACL reconstruction can be performed if diligent postoperative rehabilitation is followed. However, our belief is that the ACL reconstruction is not an emergency situation and that delaying the ACL reconstruction until the patient has a quiescent knee with full range of motion provides the best opportunity to obtain full symmetric knee motion after surgery.
One benefit of performing a staged procedure is that the surgeon can reevaluate the meniscal repair during the second operation, and an unhealed meniscus or partially healed meniscus can be treated with further trephination or resection, if necessary. Two of the meniscal repairs that did not appear healed at the time of ACL reconstruction received further treatment with trephination. Although it is difficult to determine, we believe that trephination not only contributes to initial meniscal healing but may further help partially healed menisci to completely heal eventually. This strategy, combined with our rehabilitation protocol and stabilization of the knee with an ACL reconstruction, may have further promoted healing of the menisci. Only 1 meniscus of the 19 menisci that were partially healed at the second-look arthroscopic examination required resection at a later date. The possibility that these menisci may remain partially healed, yet function as a normal meniscus, or that these menisci eventually healed, requires further investigation.
Before we performed these staged procedures of meniscal repair and ACL reconstruction, locked bucket-handle meniscal tears that were in the white-on-white zone and considered degenerative (interbody components) were excised. Since we have observed the healing capability of these large bucket-handle tears, we have become more aggressive with repair of tears in the avascular zone. Subsequently, we have attempted to repair more bucket-handle meniscal tears instead of performing resection, regardless of whether the repair and the ACL reconstruction are performed as simultaneous procedures or are staged.
Reevaluating the meniscus with an arthroscopic examination has helped us to determine whether full range of motion and full weightbearing are detrimental to the repaired meniscus. Many rehabilitation protocols that have been reported restrict motion or weightbearing or both.4,5,7,11,13 There is a general philosophy behind our rehabilitation protocol. First, the sutures are placed to prevent a redisplacement so that the meniscus, which has been stimulated with abrasion and trephination, has time to heal. Second, we allow full knee motion because it is not only important for articular cartilage nutrition but also for prevention of knee contractures. Third, by allowing full weightbearing, the femorotibial articulation helps “push” the torn portion in direct apposition to the meniscal rim. We believe that knee motion and full weightbearing promotes rather than deters healing of the meniscus. Certainly, with an ACL-deficient knee, it is important to avoid activities or sports that could allow the knee to give way and violate the repair. In this study, our meniscal rehabilitation protocol did not appear to have an adverse effect on meniscal healing.
Performance of staged procedures of meniscal repair and ACL reconstruction does involve higher cost to the patient. However, one must also consider the enormous cost, not just financial but also emotional, for a patient who requires extensive rehabilitation or further surgery, or both, for arthrofibrosis. The number of patients who undergo staged procedures for meniscal repair and ACL reconstruction is small and is limited to those patients with severe limitation of extension. We believe our approach has been justified by our low incidence rate of less than 1% of patients requiring a scar resection after ACL reconstruction.
Conclusions
Bucket-handle meniscal tears in the white-on-white meniscal zone can be repaired and salvaged; 87% of our patients who underwent this treatment remained asymptomatic 4 years after surgery. Rehabilitation after meniscal repair can allow full weightbearing without adversely affecting the results.