
Abstract
Background: There has been rapid growth in the technical and physiologic demands made on skaters who perform more and more difficult jumps, spins, lifts, throws, and free skating movements.
Purpose: To investigate the frequency of injuries and overuse syndromes in elite junior skaters.
Study Design: Questionnaire.
Methods: During four consecutive Junior World Figure Skating Championships and the Croatia Cup, we interviewed 236 female and 233 male skaters by questionnaire to determine the frequency of injuries and overuse syndromes.
Results: Fifty-nine of the female skaters (25%) and 65 of the male skaters (27.9%) reported sustaining acute injuries; 101 female (42.8%) and 106 male (45.5%) skaters reported overuse syndromes. Low back pain was reported by 19 female and 23 male skaters. The most frequent acute injury was ankle sprain. In singles female skaters, the most frequent overuse injury was stress fracture (19.8%), followed by jumper's knee (14.9%). In singles male skaters, jumper's knee (16.1%) was the most frequent injury, followed by Osgood-Schlatter disease (14.2%). More than 50% of injuries in young singles figure skaters involved overuse syndromes. Pairs skaters and ice dance skaters had a higher risk of acute injury than overuse syndrome because of falls from lifts and throw jumps.
Conclusions: Programs to improve postural alignment, flexibility, and strength, especially during the asynchronous period of bone and soft tissue development, should be instituted to prevent and reduce overuse syndromes.
As a sport, figure skating is recognized as a unique combination of art and athleticism. Figure skating is popular all over the world, but it is a very demanding and expensive sport. Because there are many indoor figure skating rinks, the skating season is continuous, with ongoing various major international competitions such as the Grand Prix series, the Grand Prix finals, the European Figure Skating Championship, the World Figure Skating Championship, and the Olympic Winter Games. Figure skating includes four disciplines—singles men and ladies skating, pairs skating, and ice dancing. 20
In the past, compulsory figures were a necessary part of the training program, but since 1990, when figures were dropped from the competitive skating, skaters have spent more time training in free skating. The result has been rapid growth in the technical and physiologic demands made on skaters by the free skating programs. In the free skating discipline, a skater performs jumps, spins, and free skating movements. 20
Pairs skating combines free skating elements performed in unison by a pair of skaters, with other elements performed together, such as lifts, throw jumps, and coordinated and common-axis spins. When the partners are together or apart, their movements should be in unison. The lifts (overhead and twist lifts) in pairs skating are becoming ever more daring and are increasingly the cause of fall-related injuries. 20
Ice dancing is based on various aspects of dance and emphasizes rhythm, interpretation of music, precise steps, speed, and carriage. It includes varied dance holds, intricate footwork, deep edges, small lifts, and spins. However, because of the intricate and at times rapid and entwined footwork, falls still occur, often at high skating speeds, causing lacerations and other injuries. 20
Figure skating is a physically demanding sport that requires a unique combination of artistic ability, speed, agility, flexibility, and power, all of which can be achieved only by long-term, persistent training.4,6,9,25 The increasing technical difficulty of figure skating has resulted in heightened demands on physical fitness. Elite figure skaters train at least 4 to 6 hours per day, six times per week, for 10 to 11 months per year.20,25 Despite the amount of training and the intensity of ice skating programs, it seems that injury rates in figure skating are low compared with those of other sports.9,10,15,18
At the competitive level there are increasing demands on athletes to perform more and more difficult elements in their skating routines. This steady expansion of the “performance envelope” has placed greater demands on those who assist the athletes in gaining and maintaining the competitive edge. This includes both the coaches who manage the complex process of performance enhancement and the health professionals who work to prevent and manage injuries. Unfortunately, injuries may sometimes interfere with an athlete's performance and training. The two types of figure skating injuries are acute injuries, defined here as injuries occurring during a certain, determined, and limited time period, that cause tissue damage, and overuse injuries, which occur due to microtraumatic tissue damage in which the original cause of the injury cannot be proved and, in most cases, the skater neither feels not remembers the time of initial tissue damage.1,8,14
Because of the increasing demands on young figure skaters, some medical concerns have arisen. Because epidemiologic studies of injuries in figure skating are rare, especially in junior skaters, the aim of this study was to assess the current incidence of acute and overuse injuries in elite junior figure skaters. A questionnaire was used to collect injury data in the elite junior figure skating population.
Materials and Methods
This study was conducted at four consecutive Junior World Figure Skating Championships: Zagreb, December 1998; Oberstdorf, March 2000; Sofia, March 2001; Hamar, March 2002; and at the Croatia Cup, held in Zagreb in September 1999. A questionnaire consisting of 22 questions was distributed to all participants in all disciplines (men and ladies singles skating, pairs skating, and ice dancing) at each competition separately. The questionnaire took approximately 15 to 20 minutes to complete. Questions were included on the frequency, site, and type of injuries (in overuse injuries, the age at which the injury occurred was included) incurred by elite junior figure skaters during their skating careers. Inquiry was also made about injury treatment (nonoperative or surgical) and the amount of time skaters had to stay off the ice. In addition, skaters were asked for their current age; the age when they started to skate and when they started to compete; their training frequency, both on and off the ice; and the specific triple jumps and number of triple jumps performed. We also inquired about use of orthoses as well as the age of menarche for female skaters.
The results were collected at the aforementioned skating events for 5 consecutive years and were analyzed together at the end of the 2002–2003 skating season. Skaters who had participated in more than one Championship event completed the questionnaire just once. Subjects often responded to the questionnaire with assistance from their coaches or team physician, or both. Questionnaires were returned by the end of each competition to the International Skating Union (ISU) medical advisor in charge of the event. Descriptive statistics was used for analysis of the data.
Results
Of the 572 skaters who participated in the five events (skaters who participated in more than one event were given the questionnaire only once), 469 (82%) correctly and completely filled out and returned questionnaires: 236 were from female skaters (107 in singles skating, 61 in pairs skating, and 68 in ice dancing) and 233 were from male skaters (104 in singles skating, 61 in pairs skating, and 68 in ice dancing). All of the respondents were between 13 and 20 years of age, with a median age of 16 years for female skaters and 18 years for male skaters. Female skaters began skating when they were between 2 and 10 years of age and male skaters began when they were between 3 and 11 years of age. All of the skaters reported practicing from 2 to 6 hours per day, six times per week, 9 to 11 months per year.
Injuries in Female Skaters
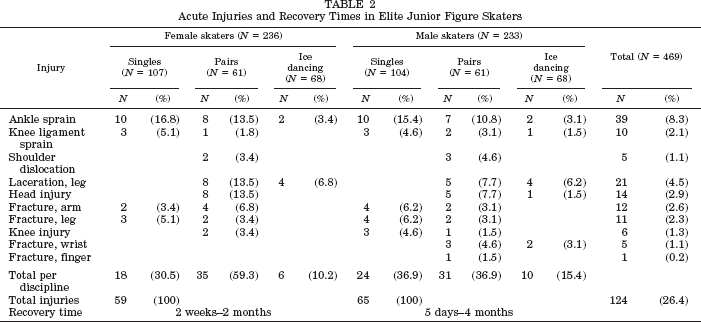
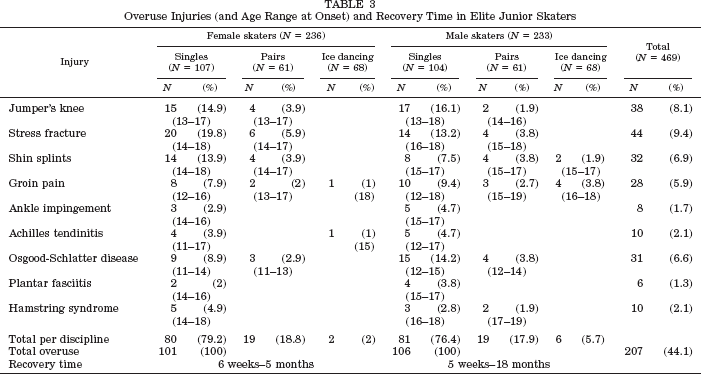
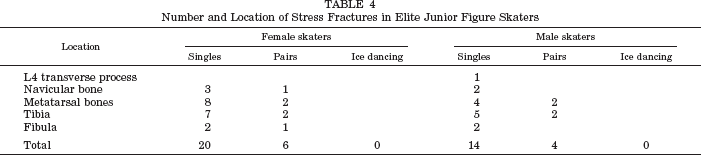
Among the 236 female respondents, 59 reported sustaining acute injuries, 101 reported overuse syndromes, and 19 reported low back pain during their junior skating career (Table 1). The acute injuries, together with recovery time (time when skaters could not train and compete because of injury), and their distribution throughout the skating disciplines are shown in Table 2. Some of the female singles skaters had more than one overuse injury during their skating career. The incidence of overuse syndromes, the time of occurrence, and the distribution of overuse syndromes throughout the skating disciplines, as well as time off the ice because of injuries are shown in Table 3. Stress fracture was the most frequent overuse injury reported by female junior skaters. They sustained a total of 26 stress fractures in various locations (Table 4). Fourteen singles skaters and 5 pairs skaters reported that they had experienced low back pain during their skating career, but they did not specify whether it was due to acute injury or overuse syndrome.
Acute and Overuse Injuries in Male and Female Elite Junior Figure Skaters

Acute Injuries and Recovery Times in Elite Junior Figure Skaters
Injuries in Male Skaters
Among the 233 male respondents, 65 reported sustaining acute injuries, 106 reported overuse syndromes, and 23 reported low back pain (Table 1). The type of acute injuries and their distribution throughout the skating disciplines are shown in Table 2. As with the female skaters, some of the male skaters reported the occurrence of more than one overuse injury during their skating career. The incidence of overuse syndromes, the time of occurrence, and the distribution throughout the skating disciplines, as well as time off the ice because of injuries are shown on Table 3. Male skaters reported a total of 18 stress fractures (Table 4). Sixteen singles skaters and 7 pairs skaters reported experiencing low back pain during their skating career, but they did not report whether it was due to acute injury or overuse syndrome.
Overuse Injuries (and Age Range at Onset) and Recovery Time in Elite Junior Skaters
Number and Location of Stress Fractures in Elite Junior Figure Skaters
Discussion
The frequency and spectrum of overuse syndromes, especially in junior singles figure skaters appear to be increasing, as evidenced by a comparison of the data of the present study with previous data. In a retrospective study, Brock and Striowski 5 reported that in 60 Canadian figure skaters, 50% of 28 injuries were acute and only 43% were overuse injuries. In another retrospective study, Brown and McKeag 6 showed that acute injuries accounted for the largest proportion of injuries in singles skating, and that the lower extremities were the site of two-thirds of all injuries. In 1999, Bloch 4 reported that figure skaters who train regularly primarily sustain lower extremity injuries, especially overuse injuries. He additionally found that foot and ankle problems may be related to the rigidity of the leather skating boot.
Our study showed that the greater percentage of overuse injuries occurs in male and female singles skaters, whereas in junior pairs skaters and ice dancers, a predominance of acute injuries is seen. Almost all of the reported overuse injuries in our study involved the lower extremities, except for one stress fracture of the lumbar spine in one male skater. Acute injuries involved the head and upper and lower extremities. Other studies have also shown that skaters predominantly incur injuries in the lower extremities, although there has been no differentiation between acute and overuse injuries.4,5,15, 21 Stress fractures in our study, except for one involving the lumbar spine, were located in the tibial, fibular, metatarsal, and navicular bones. In a previous study on stress fractures in figure skaters we saw a lower rate of stress fractures among elite seniors skaters than we found among the elite junior skaters in this study. 25 This was especially true for female singles skaters, who incurred the stress fractures in the same locations.
A number of changes in the sport have contributed to the increase in overuse injuries. 16 Along with the rapid growth in popularity of figure skating, the number of participants and the hours spent in training have increased. Skaters not only now spend more time in free skating training, but there has also been rapid progression in the technical and physiologic demands of free skating programs. There has also been a trend for children to begin training seriously at younger ages.
Over half of the injuries in the singles female and male junior skaters in this study were overuse injuries that occurred during their junior skating careers, except for nine figure skaters with Osgood-Schlatter disease that occurred when skaters were still in novice categories. It is well known that most overuse injuries can be prevented with proper education and training programs to improve flexibility, muscle balance, and jumping and skating technique.13,24–26 Only 11 of the 469 questionnaire respondents indicated that their right leg was used for landing jumps. Our study indicates that the overuse injuries were found to occur in both the landing and take-off legs. Thus, these overuse injuries occur not only because of the greater impact on the landing leg, but also because of the many jump repetitions during each practice session. Nikolic et al. 21 studied 25 figure skaters (mean age, 13.9 years) from all disciplines during a summer training camp. All 25 skaters took part in national and international competitions in the 1997 to 1998 seasons. For skaters between the ages of 8 and 14 years, 13 (60%) injuries involved the lower extremity, whereas in skaters between 15 and 20 years of age, 19 (70%) injuries involved the lower extremities. The most frequent complaints were knee pain, shin splints, and, to a lesser extent, midfoot pain. In the most experienced skaters, acute injuries and tibial periostitis occurred most frequently during summer training. The study showed that methodical “off-ice training” could be useful in preventing injuries that result from physical imbalance.
In pairs skating and ice dancing, acute injuries occurred more often than overuse syndromes. The acute injuries also tended to be more severe, because of falls from original acrobatics and complicated overhead lifts and triple and quadruple throw jumps. Smith and Ludington, 28 in a 9-month prospective study among elite pairs and ice dance skaters, reported that 11 serious injuries were caused by lifts and 7 were directly related to the skating boot. Only a few of the serious injuries appeared preventable. They suggested that only by changing the boot design and training for lifting maneuvers can the unacceptably high injury rate among elite pairs skaters be reduced. Brown and McKeag 6 reported that most lift-related injuries in pairs skaters are contusions, lacerations, fractures, hematomas, and muscle strains.
Brock and Striowski, 5 in a study of injuries in 64 nationally ranked Canadian figure skaters, found that 29 skaters (45%) sustained a significant injury over a 1-year period. There were an equal number of overuse and acute injuries. Sixty percent of the acute injuries, in nine figure skaters, were jump-related. The authors attributed the overuse injuries to the minimal time spent stretching. In another study investigating the career injuries of 19 competitive figure skaters, Smith and Micheli 29 found that there had been 52 overuse injuries and only 8 acute injuries. Both studies revealed few serious injuries, especially in comparison with sports involving similar training demands, such as gymnastics. Smith and Micheli believed that the majority of overuse injuries could be prevented with an appropriate warm-up period and improved flexibility exercises. In a later study, Smith 27 stressed that skaters who participate in a well-designed off-ice training program that incorporates maintenance of the normal flexibility of lower extremity muscles can decrease the incidence of overuse symptoms of the knee. She believed this was especially true in the growing athlete.
Figure skating is the only jumping sport that limits the movement of the ankle joint and calf muscles by the use of rigid boot support. The high heel and inflexible ankle portion of the boot do not allow skaters to use their ankles effectively in plantar flexion during jump take-offs or to cushion their landing. In our investigation, ankle sprains were common injuries in figure skaters; similar findings have been reported by Authorsen et al., 2 Bloch 4 and Danowski and Le Blond. 9 The skater's conditioning program should therefore incorporate exercises to maintain and improve on the inherent proprioception and stability of the ankle. 9
The force absorbed by the knee extensor mechanism during landing contributes to the development of anterior knee pain and overuse injuries. Symptoms can manifest as jumper's knee and Osgood-Schlatter disease, both of which were reported by the female and male junior figure skaters (singles and pairs) in our study. Such injuries have also been reported by Bloch, 4 Haspl et al., 12 Smith, 27 and Brown and McKeag. 6
Our research also revealed low back problems in elite junior skaters. This has also been reported by Omey et al., 23 who found that figure skating, as well as gymnastics and dancing, was associated with a high risk of spondylolysis, or a stress fracture of the posterior vertebral elements. Other than overuse and acute injuries, low back pain was found to be the most frequent complaint in singles and pairs figure skaters; they believed this was due to the repeated hyperextension and disc loading of the low back during frequent jumping and landing. It is recognized that, in many sports, indiscriminate, repetitive training regimens are associated with pathologic lesions at the tendinous junctions, tendoperiosteal attachments, and immature epiphyseal plates.7,8,14
The median age of menarche in our study group was 15 years. Lockwood, 16 in 1997, reported that the mean age at puberty of male and female skaters was 14 ± 1.73 (Tanner stage 3). Ross et al. 26 also, as Lockwood 16 in 1997, found that both male and female figure skaters matured later than the average population. Stress, intensive physical training, and lean body mass are associated with delayed menarche, by a couple of years, in women figure skaters, gymnasts, rhythmic gymnasts, synchronized swimmers, divers, distance runners, and ballet dancers when compared with the normal, noncompetitive population.3,11,17,19,21,32,33 Vadocz et al. 31 observed in 159 competitive figure skaters (national level, pre-elite, and elite) that girls who matured early (menarche <12.0 years) were not represented in competitive figure skaters, and they reported that later maturation was characteristic of competitive figure skaters, particularly in elite, more specialized pairs skaters. Ziegler et al., 33 who studied associations between body image, dieting behavior, and nutritional status in junior figure skaters, also found that inadequate energy intake and delayed menarche were widespread in women in this athletic group.
Asynchronous development of bone and soft tissue during this stage of maturation, in which there are periods of rapid growth (growth spurts) and loss of flexibility, provides significant additional risk of injury. During such developmental phases, it is clinically sensible to reduce the training load imposed on young athletes. Oleson et al. 22 measured the bone mass density in competitive figure skaters and found that skaters without history of stress fracture have significantly greater estimated bone mass density compared with skaters with a history of stress fracture and compared with age-matched, nonathletic control subjects. They concluded that stress fractures in adolescent skaters are not caused by low bone mass density but by excessive forces placed on a normal skeleton. By directly comparing the take-off and the landing foot, they found that the landing foot had a greater estimated bone mass density than the leading one. They suggested that coaches place greater emphasis on strengthening the lower extremity and musculature of the take-off foot, even before the skater starts to land double jumps.
It is recognized that correcting the lower extremity biomechanics can prevent overuse injuries and that skaters frequently have anomalies of their feet.7,24,25 At the championships in which our 236 female subjects competed, only 55 wore orthoses, and, of the 233 male subjects in this study, only 58 used orthoses. This was despite the fact that 98 of the female and 96 of the male skaters reported feet anomalies. Orthoses were made either by footprint mold, especially for an individual skater, or by computerized walking analysis, and then placed either in the figure skating boot or in other walking and training shoes.
Most of the injured skaters who responded to our questionnaire were treated nonoperatively with various physical therapy modalities. In the acute stage, rest, ice, compression, and elevation, combined with use of nonsteroid antiinflammatory drugs was the main method of treatment. Later on, modalities were used such as electrotherapy, ultrasound therapy, laser therapy, magneto therapy, electrical stimulation of hypotrophic muscles, hydro-kinesitherapy, and kinesitherapy. Emphasis was placed on strengthening and stretching exercises. Some of the injuries were also treated by acupuncture therapy. 30 Some injured skaters needed minor surgical treatment (to repair lacerations of the scalp and leg) and, because of the severity of injury, four skaters needed major surgery—one female skater underwent hip surgery and three male skaters had knee surgery (arthroscopy for meniscal and ligament repair).
In light of the increasing demands on young elite figure skaters and because of the increasing overuse injury incidence, medical care and preventive measures should be emphasized. It is important to stress that good postural alignment, adequate flexibility, and sufficient strength are basic requirements for the athletic and artistic components of figure skating. Correct biomechanics, gradual increases in training time and intensity, as well as progressive development of muscle strength and flexibility are the keys to avoiding overuse injuries. The areas that predominantly require flexibility are the lower extremities (quadriceps muscles, gastrocnemius-soleus muscle complex, and hamstring muscles), trunk (extensors and flexors and lumbosacral fascia), and upper extremity (rotator cuff and other shoulder muscles). The areas that require strengthening are the primary muscles for jumping (gluteus maximus, gluteus medius, hamstring, quadriceps, gastrocnemius-soleus, and tibialis anterior muscles) and trunk stability, as well as the abdominal muscles, which work to stabilize the spine. In pairs skaters, upper body strength is particularly important for preventing injuries that occur during lifts. Figure skaters should work on increasing ankle strength and proprioceptive ability so that active muscular stability and response time is developed and maintained.20,24
Conclusions
It is important to stress that there is a tendency toward an increasing incidence of overuse injuries in junior singles skaters and acute injuries in pairs skaters. Of the 469 junior figure skaters in this study, 79.5% had acute injuries, overuse syndromes, or low back problems during their skating career. Among overuse injuries in singles female skaters, stress fractures had the highest relative frequency (19.8%), followed by jumper's knee (14.9%). In singles male skaters, jumper's knee was the most frequent injury (16.1%), followed by Osgood-Schlatter disease (14.2%). More than 50% of injuries in singles figure skaters involved overuse syndromes. Among pairs skaters and ice dance skaters, acute injuries were more frequent than overuse syndromes, with the reason being falls from lifts and throw jumps. Almost all overuse injuries were located in the lower extremities, except for one stress fracture of the lumbar spine in one male skater. Acute injuries involved the head and upper and lower extremities.
Physicians, physiotherapists, and physical educators must be responsible to advise, guide, and monitor the training of young skaters. It is also important to educate coaches, administrators, and parents about the susceptibility of young athletes to both acute and overuse types of injury. A multidisciplinary approach to children in sport must address both the external precipitants of injury (footwear, surfaces, weight training) and the intrinsic factors (growth, muscle-tendon imbalance, flexibility), which are unique to immature athletes and skaters. Only through good postural alignment, adequate stretching and strengthening training programs, especially during the asynchronous development period of bone and soft tissue, can overuse syndromes be prevented and reduced.
Competitive sport for children must integrate both safety and fun to have long-term positive impact on development. Only those with talent and patience for adequate training programs will become the stars of the future.