
Abstract

Posterior dislocation of the shoulder is a rare and often overlooked injury. 7 Posterior dislocations represent only approximately 2% of shoulder dislocations and can be missed in up to 80% of cases.2,7 The mechanisms responsible for posterior dislocation of the shoulder include axial loading of the adducted and internally rotated arm, violent muscle contractions caused by seizure convulsion or electrocution, and direct force applied to the anterior shoulder.6,7
Complications commonly associated with posterior dislocations of the shoulder include fractures of the humeral proximal shaft, tuberosities, and head. Fractures of the glenoid are also commonly encountered.7,10 Recurrence of this dislocation can be a common late complication. Neurovascular injuries are rare with posterior dislocations. 7 Instances of interposed soft tissue structures have been reported.3,5,8 To our knowledge, the only reported case of a documented isolated rotator cuff tear associated with a traumatic posterior dislocation of the shoulder is the compound injury described by Moeller 6 in his 1975 case report.
We report the case of a young man who sustained a closed traumatic posterior dislocation of the shoulder. This injury was associated with a massive rotator cuff tear requiring operative repair.
Case Report
A 27-year-old professional football player intercepted the ball and was carrying it in his right (dominant) hand when he was hit from behind on the left side. He fell onto his left outstretched arm, and the opposing player landed forcefully on him, loading his posterior thorax on the left side. Clinical suspicion of a posterior shoulder dislocation was entertained because of complete loss of passive external rotation combined with severe pain; diagnosis was confirmed with plain radiographs (Fig. 1). An atraumatic closed reduction was performed after the patient was placed under sedation and had been administered muscle relaxants. Radiographs confirmed the reduction. A CT scan performed the next day confirmed the absence of associated fracture. The axial MRI scan did show minimal posterior subluxation of the glenohumeral joint (Fig. 2). The patient remained neurovascularly intact (that is, he had a normal neurovascular examination) both before and after the reduction maneuver.
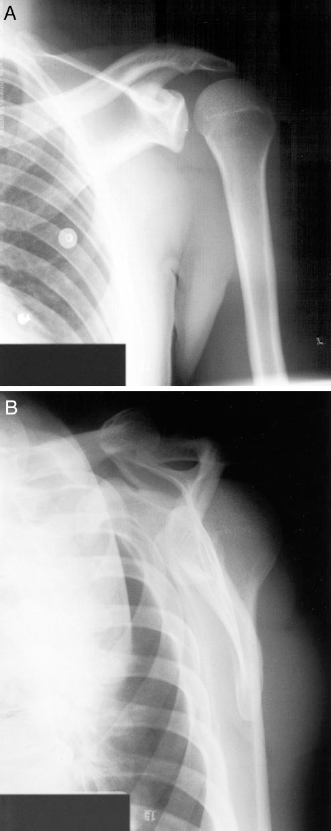
Anteroposterior (A) and transcapular view (B) radiographs of the injured shoulder showing posterior subluxation after initial closed reduction.
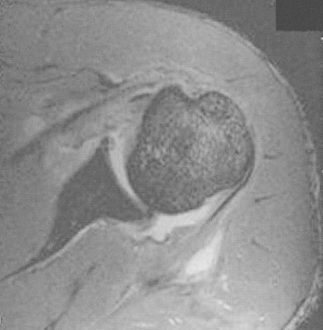
Axial MRI of the shoulder revealed minimal posterior subluxation after closed reduction.
Follow-up examination at 1 week after injury revealed gross weakness in external rotation and abduction. Another MRI scan confirmed a massive global tear 12 of the rotator cuff involving the subscapularis, supraspinatus, and infraspinatus muscles (Fig. 3). The biceps tendon was displaced from its groove anteriorly but remained intact. The transverse ligament was also torn.

A global tear of the rotator cuff seen on MRI scan.
Surgery was subsequently performed, and a primary cuff repair to bone was performed for the subscapularis, supraspinatus, and infraspinatus muscles (Fig. 4). Statac suture bone anchors (Zimmer Canada, Zimmer McCarthy and Associates, Mississauga, Ontario, Canada) were used to insert the muscles into a bony trough. The torn rotator cuff interval was repaired, the biceps tendon was replaced in its groove, and its sheath was repaired. Progressive shoulder rehabilitation was initiated.
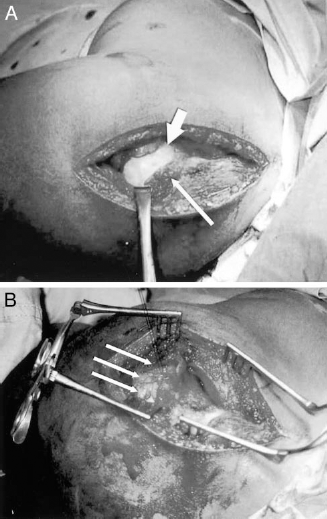
A, intraoperative findings of a large tear of the cuff. Articular cartilage of the humeral head is easily seen in the wound (large arrow). The small arrow indicates the anatomic insertion site of the rotator cuff. B, sutures in place allowing advancement of the cuff into a trough (multiple arrows) fashioned in the humeral head adjacent to the cartilage surface.
The patient's arm was kept in a sling with pendular and passive range of motion for 6 weeks. At 8 weeks, active assisted range of motion exercises were initiated, and at 10 weeks active range of motion was allowed. At 3 months, the patient returned to full contact practice with the team but did not start a regular season game until the next year because the injury occurred 3 months before the season ended. The patient currently has full external and internal range of motion as well as full flexion compared with the other side. At 1 year after injury, isokinetic concentric contraction testing of the arm at varied speeds revealed that internal rotation on the injured side was stronger than that of the nonoperated side and external rotation was comparable. The patient has returned to full-time professional sports.
Discussion
Traumatic posterior dislocation of the shoulder is a rare injury. 7 Closed posterior shoulder dislocation has never been reported in association with a massive rotator cuff tear without fracture. Other soft tissue injuries or interpositional abnormalities after posterior shoulder dislocation have been described. Subluxation of the biceps tendon has been reported previously in patients with anterior, 5 inferior, 10 and posterior 3 dislocations of the glenohumeral joint. These, however, are commonly associated with a fracture of the lesser tuberosity, greater tuberosity, or both. One case report described a posterior dislocation in which the humeral head had buttonholed through the infraspinatus muscle and precluded closed reduction. 8 This dislocation involved fractures of both the greater and lesser tuberosities. Simons and colleagues 11 presented a case in which a posterior dislocation of the glenohumeral joint caused detachment of the posterior portion of the labrum and avulsed a sleeve of periosteum from the posterior portion of the glenoid. However, this posterior labrocapsular periosteal sleeve avulsion was not associated with a rotator cuff tear.
A prospective study of 167 patients with primary traumatic anterior shoulder dislocations revealed an overall incidence of 31% with full-thickness rotator cuff tears. 1 A similar rate of rotator cuff tear (35%) with anterior shoulder dislocation has been previously demonstrated in skiers more than 40 years of age. 9
Biomechanical studies have shown that posterior instability is a continuum between subluxation and dislocation. 12 Progressive posterior force causes posterior capsular injury as well as labral injury; these structures are the primary restraints to posterior displacement. 13 The typical pathologic findings seen on MRI after an acute traumatic posterior shoulder dislocation are tearing or shredding of the posterior labrum 4 ; this has been termed a reverse Bankart lesion. 7 Damage to other posterior supporting structures is considered rare. 4
The mechanism of the injury presented here was a combined proximally directed loading force on an outstretched, adducted, and internally rotated arm combined with a posterior loading force on the thorax. These forces were presumably in the same plane and caused significant shear force at the glenohumeral joint, leading to complete capsular disruption with a global rotator cuff tear. This injury occurred in the course of normal athletic activity with a mechanism that is presumably not uncommon to the sport of football. This injury could thus be more widespread than previously reported.
Patients who exhibit signs of weakness in external rotation or abduction during clinical examination after posterior shoulder dislocation may have injured the rotator cuff mechanism. Early MRI investigation in patients with high-energy injuries may be prudent.