
Abstract

The formation of a venous false aneurysm is an uncommon but well-recognized complication of trauma. Partial disruption of a vessel wall, after trauma, causes an out-pouching of the traumatized portion of the vessel. Because of the blood flow from a feeder vein, this segment gradually expands, forming a false aneurysm.
Patients with a venous false aneurysm may remain asymptomatic for a long period or report swelling over the area of recent injury. Alternatively, they may be seen with a complication of the false aneurysm, such as deep vein thrombosis, pulmonary embolism, rupture, or pain.1,3,4,7,8 Once a venous false aneurysm has been diagnosed, the management may vary from nonoperative treatment to surgical excision in symptomatic cases.
A traumatic false aneurysm of the saphenous vein is a rare entity. We describe a case of a traumatic false aneurysm of a saphenous vein tributary, in which the patient, a cricketer, came in with swelling over the left medial malleolus. It is rare for a traumatic false aneurysm to occur in this area; nevertheless, this diagnosis should be among the differential diagnosis of a posttraumatic swelling.
Case Report
A 34-year-old international cricketer was referred to our unit with a cystic swelling over the left medial malleolus. She had sustained a cricket ball injury to the same area 2 months before the referral. The swelling appeared about a week after injury and had gradually increased in size. On examination, the swelling measured about 4 by 5 cm, was well defined, fluctuant, mildly tender, nonpulsatile, and nontransilluminant. Bruits were not present and she did not have varicose veins. Sensations of the limb were normal and all peripheral pulses were present and normal.
The results of baseline blood tests, including clotting profile, were normal. Ultrasound scan demonstrated a cystic swelling that was not communicating with either the joint or juxtaarticular tendon. Contrast MRI was performed for further evaluation. The axial fat-suppressed gadolinium images demonstrated cyst wall enhancement with a homogeneous appearance within the cyst as well as within the surrounding subcutaneous edema (Fig. 1). The proton-density coronal sequences also demonstrated the well-encapsulated cyst with intermediated changes within it (Fig. 2). The differential diagnoses of the swelling, as visualized on MRI scan, were either a posttraumatic seroma or some form of fat necrosis.

Axial fat-suppressed gadolinium image of the left ankle demonstrating cyst wall enhancement with homogeneous appearance within the cyst and surrounding subcutaneous edema over the medial malleolus.
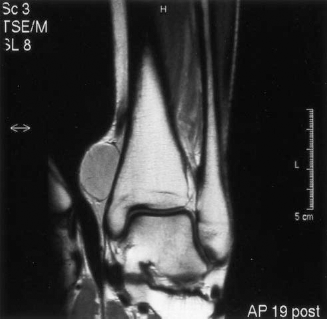
Proton-density coronal sequence of the left ankle demonstrating the well-encapsulated cyst over the medial malleolus, with intermediated changes within it.
The patient underwent surgical exploration and the swelling was found to be a false aneurysm that was communicating with one of the tributaries of the saphenous vein. The false aneurysm was resected and the communicating vein tied off. Histologic examination of the resected specimen confirmed the surgical finding. The patient had an uneventful recovery postoperatively and has been well with no sign of recurrence. She has also resumed playing cricket at an international level.
Discussion
Venous injuries after trauma are common. Most minor venous injuries are easily repairable. Although the mode of trauma may not always be straightforward, it is important to understand the ways in which a vein can be traumatized, because possible complications can then be anticipated. Venous injuries may be classified according to the mechanism of injury sustained. These mechanisms can be broadly divided into five categories; namely, incisional injuries, lacerations, contusions, overstretching, and complete division of the veins. 2 A vein gets overstretched when it lies close to a bone or joint. 2 A severe stretch causes an intramural tear that leads to exposure of the collagen, formation of thrombus, and, finally, a false aneurysm. 2
The first clinical report of a venous aneurysm was made in 1913 by Osler, who described an aneurysm of the axillary vein. 6 Formation of a false aneurysm is a well-recognized, delayed complication of vascular injury and is more frequently encountered in an artery. This is because arteries are high-pressure systems compared with veins. 1 Venous aneurysms may either be congenital, where there is vessel wall weakness, or traumatic.1,4,7 There may also be an inflammatory or degenerative origin.1,4,7 A number of predisposing factors have been described, including the presence of varicose veins and infections. 4 The differential diagnoses of venous aneurysms, which vary depending on the location, include arterial aneurysms, enlarged lymph nodes, arteriovenous fistulas, abscesses, seromas, and venous spaces within hemangiomas and tumors.1,3,4 The literature contains several reports of venous aneurysms, with the minority being traumatic in origin.
Posttraumatic venous false aneurysms typically develop over a period of weeks and appear as nonpulsatile cystic swellings that decrease in size on elevation of the limb. A high index of suspicion is essential to diagnose this condition, especially when the aneurysm is in an atypical location. The diagnosis can be confirmed by investigations such as MRI scans, Doppler ultrasonography, and venography.5,8 Magnetic resonance imaging is a good scanning technique for soft tissue swellings because it indicates the anatomic location and extent of involvement of adjacent structures. However, MRI may not always accurately identify a venous aneurysm. This is because an MRI scan may fail to show a feeder vein and because the absence of a thrombus within the aneurysm, in combination with surrounding edema, makes the swelling appear to be a homogeneous, well-encapsulated mass. 4 Duplex scanning and venography are better tools for diagnosis, with the latter being the standard. 5 Once the diagnosis is confirmed, symptomatic false aneurysms should be treated surgically. 8
In retrospect in this case, we would have considered traumatic venous aneurysm among the differential diagnoses, had we suspected such a condition existed. The history and examination were compatible with the diagnosis; also, careful evaluation of the MRI scan did reveal the presence of a vein distal to the aneurysm, although it is difficult to detect a communication between them. However, the rarity of the condition rendered preoperative diagnosis challenging.
In conclusion, to the best of our knowledge, this is the first reported case of a posttraumatic aneurysm of a distal tributary of the saphenous vein. Although this is an extremely uncommon occurrence, it is an important diagnostic consideration when examining a patient with a post-traumatic swelling.