
Abstract
The management of hip injuries in athletes has evolved significantly in the past few years with the advancement of arthroscopic techniques. The application of minimally invasive surgical techniques has facilitated relatively rapid returns to sporting activity in both recreational and elite athletes. Recent advancements in both hip arthroscopy and magnetic resonance imaging have elucidated several sources of intraarticular abnormalities that result in chronic and disabling hip symptoms. Many of these conditions were previously unrecognized and, thus, left untreated. Current indications for hip arthroscopy include the presence of symptomatic acetabular labral tears, hip capsule laxity and instability, chondral lesions, osteochondritis dissecans, ligamentum teres injuries, snapping hip syndrome, iliopsoas bursitis, and loose bodies (for example, synovial chondromatosis). Less common indications include management of osteonecrosis of the femoral head, bony impingment, synovial abnormalities, crystalline hip arthropathy (gout and pseudogout), infection, and posttraumatic intraarticular debris. In rare cases, hip arthroscopy can be used to temporize the symptoms of mild-to-moderate hip osteoarthritis with associated mechanical symptoms. This article discusses the current clinical and radiographic methods to detect early hip joint disease and the current indications and surgical techniques of hip arthroscopy.
Arthroscopic surgery of the hip was first introduced in 1931 by Burman, 7 but it did not begin to gain popularity in North America until 1977 when Gross 48 reported his experience with arthroscopic treatment of congenitally dislocated hips. Hip arthroscopy remained relatively obscure throughout the early 1980s, however, with only sporadic reports on the clinical application of this surgical technique.52,98 The relatively slow development of arthroscopy of the hip in North America is in stark contrast to the much more rapid development of arthroscopic techniques around the knee and shoulder. There are a number of reasons for this phenomenon. Anatomic constraints (Fig. 1) make arthroscopy of the hip significantly more challenging than similar surgery around the shoulder and knee. The femoral head is deeply recessed in the bony acetabulum and is convex in shape. The thick fibrocapsular and muscular envelope around the hip joint decreases the amount of hip distension allowed during arthroscopy; the relative proximity of the sciatic nerve, lateral femoral cutaneous nerve, and remaining femoral neurovascular structures make portal placement more challenging.29,59 The surgical evolution of hip arthroscopy has also contributed to its relatively slow development. Compared with knee arthroscopy, which evolved from more traditional open surgical procedures, arthroscopic hip procedures have generally not been preceded by open techniques. For the hip, arthrotomy has generally been reserved for more advanced disease states, while the types of injuries currently addressed with arthroscopy have historically been largely unrecognized and untreated.
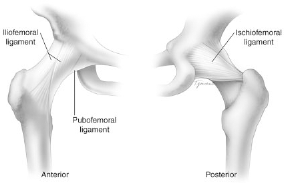
Anatomic constraints of the hip. The anterior ligamentous constraints of the hip are seen in the anterior view and include the iliofemoral and pubofemoral ligaments. The ischiofemoral ligament is the primary posterior restraint.
Within the discipline of sports medicine, the hip has received considerably less attention than other joints, largely because of the difficulty that practitioners have traditionally had in assessing intraarticular abnormalities around the hip. Over the past few years, hip arthroscopy has been gaining considerable interest. Evaluation and measurement of hip capsule distension and distraction forces necessary to adequately visualize the hip joint were performed by Eriksson and Sebik. 34 Techniques of needle positioning, anatomic landmarks, and cannula placement were described by Johnson. 57 Lateral decubitus positioning and peritrochanteric portal placement were described by Glick and colleagues,41,43 while Byrd8,10,11 and Byrd and Jones 14 have provided numerous technical suggestions for the performance of hip arthroscopy in the supine position. Philippon 82 has described the modified supine position with the hip in slight internal rotation (15°), flexion (10°), neutral abduction, and lateral tilt (10°). The advent of better diagnostic tools, especially MRI, has helped in the detection of hip labral tears in a more predictable fashion. New techniques and instrumentation have facilitated the treatment of labral tears by hip arthroscopy. Most notably, the recent adaptation of arthroscopy equipment to create flexible scopes and instruments specifically designed for the hip has led to improved safety, visualization, and accessibility of this joint (Fig. 2).
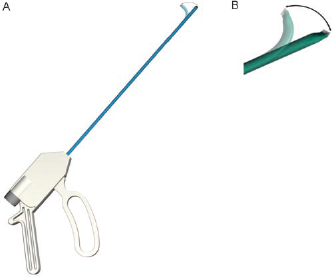
A, radiofrequency heating probe; B, close-up of flexible tip that allows for greater access to constrained regions in the hip joint.
Athletes subject their bodies to extreme forces; their lower extremity joint may experience joint reactive forces in excess of five times body weight during activities such as running and jumping. 81 The mechanisms of injuries can be from repetitive motion or direct trauma. Subtle radiographic evidence of hip dysplasia may place the athlete at underlying risk for labral injury. 13 A source of intraarticular abnormality should be investigated in patients with unremitting hip pain lasting longer than 4 weeks. One author (MJP) has had significant experience with the arthroscopic treatment of elite and amateur athletes from a wide variety of sporting endeavors including golf, football, ice hockey, baseball, basketball, tennis, skateboarding, gymnastics, weightlifting, ballet, soccer, tae-kwan-do, Olympic yachting, and figure skating (Ref. 81; S. Bharam et al., unpublished data, 2002 and 2003). In this experience, hip arthroscopy has been very effective for the treatment of several athletic injuries such as labral tears, capsular laxity with iliofemoral ligament deficiency, lateral impact injury, chondral injuries, injuries to the ligamentum teres, extraarticular conditions (internal and external snapping hip), and loose bodies. Other less common indications for hip arthroscopy include management of osteonecrosis of the femoral head, synovial chondromatosis and other synovial abnormalities, crystalline hip arthropathy (gout and pseudogout), infection, management of posttraumatic intraarticular debris, and in extremely rare cases, management of mild-to-moderate hip osteoarthritis.
This article discusses the current clinical and radiographic methods to evaluate sports-related injuries around the hip and discusses the current indications and surgical techniques of hip arthroscopy.
Anatomic Considerations
The articulation between the head of the femur and the acetabulum form the hip joint. This bony configuration is intrinsically stable except in situations where there is variation in the acetabular depth and femoral head geometry, which results in more reliance in the surrounding soft tissue. Version and inclination of the weightbearing surface affect the joint capsule and ligaments of the hip, the ligamentum teres, as well as the suction effect of the hip. 6 The femoral head normally forms two-thirds of a sphere and it is flattened in the area where the acetabulum applies its greatest load. In the neutral anatomic position, the anterior part of the femoral head is not engaged in the acetabulum and the labrum augments the femoral head coverage by its extension from the bony acetabulum.
The labrum runs circumferentially around the acetabulum perimeter to the base of the fovea and becomes attached to the transverse acetabular ligament posteriorly and anteriorly (Fig. 3). 83 Free nerve endings, including proprioceptors and nociceptors, have been identified within labral tissue, which may explain decreased proprioception and pain in an athlete with a torn acetabular labrum (Ref. 61; S. Lephart et al., unpublished data, 2002). Much like the meniscus, the labrum has a relatively low healing potential because of decreased vascularity (Fig. 4). The vessels that penetrate the labrum are found only on the outermost layer of the capsular surface, leaving most of the labrum avascular (G. S. Shapiro et al., unpublished data, 2001). The acetabular labrum is made of fibrocartilage and may enhance stability by maintaining negative intraarticular pressure in the hip joint. 96 It also may act as a tension band to limit expansion during motion between the anterior and posterior columns during loading in the gait cycle. 83
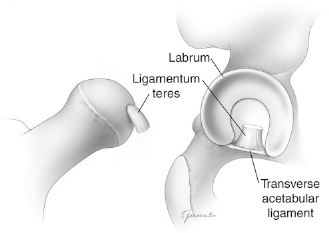
The labrum surrounds the rim of the acetabulum nearly circumferentially and is contiguous with the transverse acetabular ligament across the acetabular notch. The ligamentum teres arises from the margins of the acetabular notch and the transverse acetabular ligament.

The hip labrum is relatively avascular; however, there is increased vascularity seen arising from the capsular attachments. This may have implication for arthroscopic repair of the labrum.
Ferguson et al.36–38 have looked at the role of the intact labrum on hip joint cartilage consolidation and the formation of a labral seal in hip joint mechanics. They found that the absence of the labrum significantly increased cartilage surface consolidation as well as contact pressure of the femoral head against the acetabulum. They further demonstrated that the labrum had an important sealing function in the hip joint that limited fluid expression from the joint space and protected the cartilage layers of the hip.36,37 Ferguson et al. 38 used a poroelastic finite element model to demonstrate that the labrum provided some structural resistance to lateral motion of the femoral head within the acetabulum, thus enhancing joint stability and preserving joint congruity. In analyzing the labral capsular complex, there is a theoretical concern about the potential for rotational instability of a hip associated with a deficiency of labral tissue. This instability may be caused by redundant capsular tissue, which creates a potential abnormal load distribution from a transient incongruous joint resulting from subtle subluxation. 83
The ligamentum teres is extracapsular and may have some stabilizing effect on the hip joint with a deficient labrum. 86 The psoas tendon protects the anterior intermediate portion of the capsule and, by virtue of its anatomic location, can be subjected to increased load in athletic activities; such loads may be increased in athletes with further intraarticular abnormalities. The psoas bursa communicates with the hip joint in the adult in approximately 20% of the population. 81
Assessment and Clinical Examination of the Athlete with Hip Pain
Injuries to the hip in athletes are often categorized as muscle strains or soft tissue contusions. However, hip pain, particularly in the young adult, may arise from a number of soft tissue structures in and around the hip joint. It is important to be able to differentiate extraarticular from intraarticular abnormalities. The examination of the hip is often complicated by the relatively common incidence of referred pain from the lumbar or sacral areas and occasionally from genitourinary tract and intraabdominal or abdominal wall problems. 58 The examination may also be affected by patient age; causes of hip pain should be separated into those relevant to the pediatric and adult populations. 92 Hip pain in the pediatric athlete includes skeletal causes such as hip dislocation, bony avulsion injuries, and fractures (stress and pathologic). Soft tissue origins of pain include myotendinous strains, apophyseal insertion site injuries, and contusions. Non-traumatic causes include slipped capital femoral ephiphysis, Legg-Calvé-Perthes disease, developmental dysplasia of the hip, toxic synovitis, and septic arthritis.80,92 In the adult, hip pain may originate from articular injuries including stress reaction or fracture; hip dislocation or subluxation; femur, pelvic or acetabular fractures; labral tears; avascular necrosis; and cartilage injury or degeneration. Soft tissue causes of pain include bursitis, snapping hip from the iliopsoas or iliotibial band, contusion, myotendinous strains, piriformis syndrome, myositis ossificans, inguinal or femoral hernia, neurologic irritation, and hamstring syndrome.58,92 As mentioned previously, referred pain must also be ruled out for both the pediatric and adult populations.
In examining the athlete's hip, it is essential to possess a thorough knowledge of hip anatomy to accurately correlate physical examination findings with diagnostic imaging studies. A comprehensive patient history, physical examination, and radiographs will result in an accurate diagnosis of many painful hip conditions such as iliotibial band tendinitis, greater trochanteric bursitis, inguinal or femoral hernia, hip fractures or dislocations or both, osteonecrosis, osteoarthritis, or calcified intraarticular loose bodies. Other conditions–-such as labral tears, hip instability, iliopsoas tendinitis, inflammatory arthritis, early avascular necrosis, occult fractures, psoas abscess, tumor, upper lumbar radiculopathy, or vascular abnormalities–-may be more challenging to diagnose and usually require more sophisticated imaging techniques such as CT, MRI, and radioisotope studies. 30
The history should assess the qualitative nature of the discomfort (such as pain, clicking, catching, instability, stiffness, weakness, or decreased performance), the specific location of the discomfort, the timing of the onset of symptoms, the precipitating cause of the symptoms, and assessment of any referred or systemic causes of hip pain.16,58,92 Intraarticular causes of intractable hip pain, in the adult, can be seen in a variety of ways. Patients may have pain in the anterior groin, anterior thigh, buttock, greater trochanter, or medial knee. Other symptoms include persistent clicking, catching, locking, giving way, or restricted range of motion. Symptoms are usually preceded by a traumatic event, either a fall or twisting injury, and can be present in all age groups. In addition, symptoms are generally exacerbated with activity and improved with rest.
The initial portion of the examination should assess the patient's gait and posture. Antalgic gait patterns result in shortening of the stance phase, as well as shortening of the length of the step on the affected side secondary to pain. During a Trendelenburg's gait, functionally or physiologically weakened gluteus medius forces shift the upper body to the involved side so as to move the center of gravity over the painful hip and decrease the moment arm forces across the hip joint. 53 Evaluation of posture and limb position should focus on pelvic obliquity, limb length inequality, muscle contractures, and scoliosis. 92 Examination of the hip joint itself begins with palpation of specific regions of the hip to localize sites of tenderness, to delineate the integrity of the muscular structures about the hip, and to identify any areas of gross atrophy. If the source of the pain is truly intraarticular, palpable pain can rarely be elicited. Active and passive range of motion of both hips should be evaluated with the patient in the supine position. Any asymmetry in adduction, abduction, flexion, extension, external rotation, and internal rotation should be noted.
Several tests can be exercised to identify specific hip abnormalities. The Thomas test will help to identify the presence of a hip flexion contracture by eliminating the effects of excessive lumbar lordosis on the perceived extension of the hip. 53 Typically, passive range of motion should match or exceed active range of motion; however, provocative maneuvers performed during passive range of motion evaluation may result in limited motion secondary to pain and are highly suggestive of intraarticular abnormalities. Painful hip flexion, adduction, and internal rotation can indicate acetabular rim problems or labral tears, especially if clicking or groin pain is present. The Faber test involves flexion, abduction, and external rotation of the hip and suggests sacroiliac abnormalities or iliopsoas spasm. The Ober test is used to evaluate tightness in the iliotibial band. The test is positive when the leg remains in the abducted position after the hip is passively extended and abducted with the knee extended. The piriformis test is performed by flexing the hip to 60°, stabilizing the hip, and exerting a downward pressure on the knee. If the piriformis is tight, pain is elicited; if the sciatic nerve is compressed (piriformis syndrome), the patient experiences radicular-like symptoms.53,92 Mechanical symptoms attributable to intraarticular abnormalities can also be elicited by loading the hip joint with both a resisted leg raise in the supine position as well as forced internal rotation while applying an axial load. Both of these maneuvers can load the hip joint anterolaterally, which is the most common location for labral tears.
The complete physical examination should include motor strength testing of both hips to detect subtle differences from side to side. Finally, a neurovascular examination should be performed to rule out referred pain secondary to radicular symptoms or vascular causes. In most patients, hip pain goes away over time if the patient complies with nonoperative treatment. If a patient's hip pain persists, is reproducible on physical examination, and does not respond to appropriate nonoperative measures(includingrest, ambulatorysupport, nonsteroidal antiinflammatory drugs, and physical therapy), hip arthroscopy may be of substantial value.99,100 A subset of patients may have persistent symptoms despite negative or uncertain radiographic studies. Arthroscopy can lead to definitive diagnoses such as focal degenerative arthritis, chondromalacia, chondral flap tears, nonossified loose bodies, synovitis, labral lesions, and synovial chondromatosis in as many as 40% of these cases.71,73
Imaging of the Painful Hip
Radiologic workup of intractable pain of the hip includes plain radiographs, radionuclide bone scan, CT, ultrasound, MRI, and MR arthrography. Plain radiographs of the pelvis are the mainstay in the initial evaluation of pelvic and hip pain and are useful to diagnose acute traumatic fractures, avulsion fractures, dislocation and subluxation, osteitis pubis, and degenerative joint disease. A standard hip radiographic series should include an AP view of the pelvis and AP and “frog-lateral” views of the affected hip. 32
Bone scan or radionuclide imaging uses radiopharmaceutically labeled bone avid agents and gamma camera technology to reveal information regarding local blood flow and osteogenic activity.32,58 Technetium-labeled diphosphonate is the most commonly used agent. In the single-phase examination, pathologic abnormalities will result in areas of increased uptake relative to normal bone 2 to 4 hours after intravenous injection. Bone scan is highly sensitive for a variety of conditions including fractures, arthritis, neoplasm, infections, and vascular abnormalities; however, it suffers from low specificity and poor anatomic resolution. If increased uptake is identified, additional imaging studies often will be required to further elucidate the anatomic nature of the abnormal area of bone.
Computed tomography offers the greatest spatial resolution for assessing bony abnormalities of the hip and pelvis. The most common uses for CT around the hip include trauma, congenital hip dysplasia, preoperative prosthesis planning, evaluation of neoplasms, and hip imaging in patients who have contraindications to MRI. Axial images performed through the pelvis generally have a slice thickness of 2.5 to 5.0 mm, while slices through the hip joint should be thinner (between 1.2 and 2.5 mm). Coronal and sagittal reformatted images as well as three-dimensional reconstructions can help in further defining the anatomy of the abnormality. The CT arthrography is performed with the use of intraarticular contrast, which results in joint capsule distension as well as increased contrast between the lower attenuation of cartilage and labral tissue and the contrast medium.58,62,92
Ultrasound can be helpful for evaluation of intraarticular effusions and soft tissue swelling by providing a direct, painless, and noninvasive image of the hip joint and surrounding musculature. It may be particularly useful in the pediatric population for diagnosis of hip joint subluxation and dislocation.24,92
Magnetic resonance imaging has become the examination of choice for the evaluation of unexplained hip pain. Its unique ability to provide detailed images of soft tissue-and marrow-based abnormalities in multiple planes of view makes it superior to other modalities employed in intraarticular hip imaging. Magnetic resonance imaging has been most successful at demonstrating inflammatory arthropathies and the presence of joint effusions.5,32 However, MRI has been less accurate in detecting abnormalities of the articular surface.30,51,85 Edwards and colleagues 30 found MRI to have a relatively poor diagnostic yield in the evaluation of cartilage abnormalities. These authors prospectively studied 23 patients who underwent MRI followed by hip arthroscopy within a 3-week period. In patients with chondral softening, fibrillation, or partial-thickness defects of less than 1 cm, MRI provided a poor diagnosis. In addition, MRI was not reliable in finding osteochondral loose bodies and labral tears. Gadolinium-enhanced MR arthrography of the hip may be performed when evaluation of the capsulolabral structures or articular surfaces is most important. Intraarticular injection of 10 to 15 ml of gadolinium solution, followed by routine MRI may increase the sensitivity and specificity of detecting intraarticular hip abnormalities.32,58 Czerny and colleagues 21 compared conventional MRI with MR arthrography in the diagnosis of labral tears. They reported a sensitivity and accuracy of 80% and 65% for conventional MRI compared with 95% and 88% with MR arthrography. Results such as these suggest that MR ar-thrography may have a significant advantage over conventional MRI for the evaluation of capsulolabral structures in the hip. More recent cartilage imaging methods, described by Potter et al., 84 may obviate the need for intraarticular gadolinium in the MRI detection of chondral lesions of the hip.
Current Indications for Hip Arthroscopy in Athletes
Labral Tears
The acetabular labrum is a triangular fibrocartilage that is attached at its base to the rim of articular cartilage surrounding the perimeter of the acetabulum. At the inferior-most aspect of the acetabulum, the labrum is absent where the transverse acetabular ligament completes the circumferential rim. 70 Its presence effectively deepens the acetabulum and likely acts as a hip stabilizer by extending the surface area of the hip joint, thus assisting in constraint of the femoral head in the bony socket. In addition, the labrum provides proprioceptive feedback 61 as well as aiding in the distribution of synovial fluid and joint lubrication.
Normal hip anatomy can be overloaded during high-level athletic activities. Any imbalance between the forces acting in the hip joint, including labral injury, can disturb the buffer mechanism in the hip.82,83 Labral tears may ultimately be associated with articular cartilage lesions located on the surrounding femoral head or acetabulum (Fig. 5). Subchondral cysts may form as the result of pressurized joint fluid that burrows beneath the delaminating acetabular cartilage and subchondral bone. Labral tears that have been present for many years may contribute to the progression of hip osteoarthritis. 74 Patients at risk for this phenomenon are those with developmental dysplasia, tears more than 5 years old, or chondral full-thickness lesions. 75

Labral lesion with associated chondral lesion on femoral head. Note the appearance of the chondral lesion adjacent to the degenerative labral tear.
Dynamic forces acting across the injured hip will result in hip pain, decreased athletic performance, and limitations in activities of daily living. The diagnosis of a labral tear remains largely clinical and is analogous to those patients with meniscal abnormalities. These patients often have mechanical symptoms (catching and painful clicking) as well as restricted range of motion. The symptoms are sometimes more subtle, with dull, activity-induced, positional pain that fails to improve with rest. 70 Classic symptoms of hip clicking may be misdiagnosed as a labral tear when the cause is from a different source (snapping iliotibial tendon or a hypermobile psoas tendon). Specific traumatic events such as twisting, falling, or other lower extremity loads may precede the onset of symptoms. The most common cause of hip labral tears is the application of an external force on the hyperextended, externally rotated hip. 70 Often, no such sentinel event is identified, but rather the patient seeks medical attention for lingering hip pain after an initial diagnosis of groin pull, muscle strain, or hip contusion. It has been shown that labral tears are associated with acetabular dysplasia. 28 Certain athletes, such as dancers and gymnasts, may have a predisposition to developing labral tears. The increased flexibility that is required for these athletic endeavors may be made possible secondary to underlying mild acetabular dysplasia and diminished femoral head containment characteristic of the dysplastic hip. 70
An arthroscopic classification of labral tears has been described by Lage et al. 64 (Fig. 6). These authors divided the tears into four morphologic groups: radial flap tears (57%), radial fibrillated labra (22%), longitudinal peripheral tears (16%), and abnormally mobile tears (5.4%). Most series report that the majority of labral tears in the North American population are located anteriorly and are often associated with sudden twisting or pivoting motions.2,27 In contrast, in the Asian population, tears are more frequently found posteriorly and are associated with hyperflexion or squatting motions. 70
Arthroscopic classification of hip labral tears: A, radial flap; B, radial fibrillated; C, longitudinal peripheral; D, abnormally mobile.
Patients who have persistent hip pain for longer than 4 weeks, clinical signs, and radiographic findings consistent with a labral tear are candidates for hip arthroscopy. No radiographic study, however, including high-contrast gadolinium-enhanced arthrography MRI scanning, is entirely sensitive or specific in the detection of labral tears (J. C. McCarthy et al., unpublished data, 1998). Thus, a high clinical suspicion of positive physical findings is essential for proper treatment. The goal of arthroscopic debridement of a torn labrum is to relieve pain by eliminating the unstable flap tear that causes the observed hip discomfort. As such, the surgeon seeks to debride all torn tissue and leave as much healthy labrum intact as possible (Fig. 7). The articular surface of the labrum has limited vascular penetration and no synovial covering. The labrum is thinner in the anteroinferior section and thicker and slightly rounded in appearance posteriorly. In the posterosuperior portion of the acetabulum, an inferior recess is present. A recess between the acetabular labrum and the hip extends circumferentially around the labrum. Once the labral tear is well identified, the margins need to be defined. Probing and focal delineation by heat treatment with a monopolar flexible probe will complete this process. This allows for contraction of the torn portion of the labrum. A flexible ligament chisel is used to cut the torn part of the labrum, leaving only a small portion attached. A motorized shaver is then used to complete the debridement and to remove the torn portion of the labrum. 82
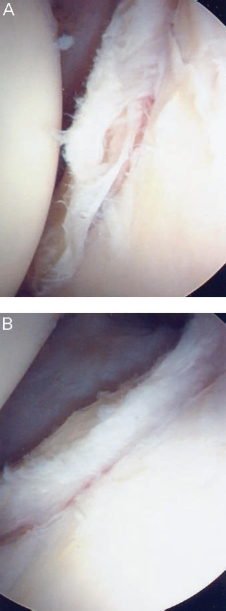
Debridement of labral tears (A) should remove all degenerative tissue and leave as much viable tissue as possible (B).
We have looked at our preliminary results of over 500 labral tear debridements performed over the past 7 years and have found nearly 90% good or excellent results with appropriately selected patients who demonstrated obvious labral abnormalities at the time of arthroscopy. Nofsinger et al. (unpublished data, 2003) found 85% good or excellent results after arthroscopic debridement of 40 patients with isolated labral tears of the hip. They reported that patients with isolated labral tears did significantly better than patients with labral tears and additional intraarticular abnormalities. One author (MJP) has had experience with labral repairs in 12 patients, including 3 professional athletes. Seven of these patients had the labrum detached from the bony acetabular rim and five had intrasubstance tears. In these cases, it was believed that complete debridement of the labrum would have deleterious effects on hip mechanics, and preservation of the labrum was performed (Fig. 8).36–38 Preliminary follow-up of these patients is favorable, with all patients demonstrating a clear improvement in their symptoms (S. Bharam et al., unpublished data, 2003).
Arthroscopic labral repair. The labrum is seen detached off of the bony acetabulum (A) and is repaired back using a suture anchor and mattress suture around the labral tissue (B).
Postoperatively, the patient starts range of motion exercises of the surgical hip within 4 hours after surgery with neutral rotation. Rotation precaution is necessary for approximately 18 to 21 days and straight-leg raising is prohibited for 4 weeks. The patient's rehabilitation emphasizes early aquatic, proprioception, and strengthening exercises. 82
Capsular Laxity
Instability of the hip joint is much less common than that in the shoulder, but can be a source of great disability. The hip joint relies much less on its adjacent soft tissue for stability because of the intrinsic osseous stability. It is apparent that any deviation from “normal” bony anatomy will lead to more dependence on the capsular tissue and labrum for stability. The labrum helps to contain the femoral head in extremes of range of motion, especially flexion. The labrum and capsule also act as load-bearing structures during flexion, causing a hip with a deficient labrum to be subject to instability if capsular laxity is present.82,83 We are currently performing biomechanical studies investigating the effects of capsular and labral injury on femoral head translation and rotation. A theoretical concern for the potential rotational instability of the hip with a deficient labrum has been confirmed by our recent cadaveric studies. Martin et al. (personal communication, 2003) have demonstrated elongation of the iliofemoral ligament when load is applied to a hip with an incompetent labrum. A deficient labrum associated with redundant capsular/ligament tissue can create a potential abnormal load distribution due to a transient incongruent joint from subtle subluxation. 83 Takechi et al. 96 have demonstrated that the labrum may enhance stability by providing negative intraarticular pressure in the hip joint. As previously mentioned, Ferguson et al. 38 have shown that the labrum provides structural resistance to lateral motion of the femoral head within the acetabulum, enhances joint stability, and preserves joint congruity. The labrum may also participate in nociceptive and proprioceptive mechanisms as free nerve endings and sensory end organs have been identified in its superficial layers. 61
Hip instability can be a difficult disorder to diagnose and can be of traumatic or atraumatic origin. Commonly, the history provides the greatest clues to the diagnosis when the patient describes the motion that reproduces the symptoms. Pelvic rotation and external rotation at the hip commonly elicit symptoms. Such maneuvers as throwing a football to the sideline or swinging a club during a golf drive will oftentimes precipitate the sense of instability. 83 Preliminary research in our neuromuscular laboratory has demonstrated decreased proprioception and balance in patients with labral tears. Also, testing of professional golfers with labral tears and associated instability has shown significant improvement after surgical treatment, which included labral tear debridement and thermal capsulorrhaphy (M. Philippon, personal communication, 2002). On examination, the patient with atraumatic instability sometimes will be able to voluntarily demonstrate subluxation or dislocation of the involved hip and may have signs of general joint laxity. Habitual or voluntary dislocation has been reported in the pediatric population as well as in patients with connective tissue disorders such as Ehlers-Danlos syndrome, Marfan syndrome, and Down syndrome. 83 Bellabarba et al. 4 recently described another source of atraumatic idiopathic hip instability secondary to subclinical capsular laxity with mild resultant acetabular dysplasia.
Several studies have reported the presence of excessive hip capsular laxity associated with previous hip dislocation or subluxation.23,69,77,87,93 Dall et al. 22 reported the presence of capsular redundancy after recurrent anterior dislocation; Liebenberg and Dommisse 68 described the development of posterior capsular redundancy after recurrent posterior dislocation. These authors suggest that subtle instability may result from the loss of suction effect of the labrum after a tear and that capsular elongation and attenuation becomes an important factor in the origin of hip pain.22,83
Professional athletes may develop overuse injuries of the hip from abnormal stresses on normal anatomy resulting in hip pain with associated subtle rotational hip in-stability. 83 Injuries or soft tissue abnormalities such as labral tears or iliofemoral ligament insufficiency can disturb the complex buffer mechanism in the hip and result in increased tension in the joint capsule and its ligament, and a decreased ability to absorb stress. Bony abnormalities such as increased superior lateral inclination can also increase tension in the joint capsule. Both situations may result in elongation of the hip capsule and subsequently create tissue redundancy and relative instability.6,83 This entity has been recognized mainly in professional and high-level athletes involved in sports requiring repetitive hip rotation with axial loading (such as golf, figure skating, football, gymnastics, ballet, and baseball). The most common injury pattern seen by one author (MJP) has been labral degeneration with combined subtle rotational hip instability, which has been successfully treated arthroscopically with labral debridement and thermal capsulorrhaphy. 83 The use of thermal capsulorrhaphy in conjunction with partial labral resection should be based on both clinical suspicion and visualization of redundant capsular tissue or attenuated capsular tissue. Early results of this treatment regimen have been very successful, with an 82% return to preinjury high-level athletics with minimal or no pain. 83
Arthroscopic thermal modification of collagen in the hip capsular tissue appears to be a treatment option for patients with hip instability. One author (MJP) has significant experience with its use in athletes with rotational instability associated with labral tears.81,83 It also may be of benefit in patients with posttraumatic instability from hip dislocation or subluxation, as well as in patients with atraumatic instability associated with generalized ligamentous laxity. Short-term results appear promising; however, more studies are required to determine the long-term efficacy and potential shortcomings of this treatment approach. 83 Recently, we have begun to perform arthroscopic capsular plication in patients with significant capsule redundancy and laxity. Further clinical evaluation of these patients is forthcoming.
Chondral Lesions: Lateral Impact Mechanism
Although chondral injury is a reported indication for hip arthroscopy, these lesions can be an elusive source of hip pain.9,10 Traditionally, chondral damage around the hip has been associated with either progressive joint deterioration (osteoarthritis or rheumatoid arthritis) or trauma. However, acute isolated traumatic articular surface injuries can occur from impact loading across the hip joint. There appears to be a particular propensity for this injury pattern in young, physically fit adult males who suffer impact loading over the greater trochanter in association with sport or activity. The so-called “lateral impact injury” occurs after a blow to the greater trochanter, which, because of its subcutaneous location, has minimal ability to absorb large forces. The high bone density of this region allows impact on this area to transfer energy and load to the joint surface, resulting in chondral lesions of the femoral head or acetabulum without associated osseous injury. Arthroscopic findings in this clinical scenario will commonly support this lateral impact mechanism. 9
In most cases of chondral injuries in the hip joint, symptom onset is immediate; however, in some cases the injury will appear innocuous with variable associated dysfunction. Persistent symptoms such as intermittent catching or pain elicited by provocative maneuvers should prompt a more extensive diagnostic workup. Although gadolinium-enhanced MR arthrography is currently the most promising imaging modality, it still has some limitations in reliably demonstrating chondral injuries, perhaps because of the static nature of the imaging study and the lack of hip joint distraction during the test. Potter et al. 84 have demonstrated the utility of cartilage-sensitive MRI for the detection of these lesions, which can be performed successfully without the use of gadolinium.
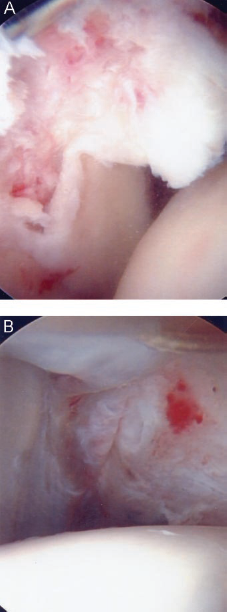
The difficulty in diagnosing these lesions as well as the inability to improve symptoms with nonoperative management provides a reasonable rationale for the use of arthroscopic hip surgery in the treatment of chondral injuries. In the presence of persistent symptoms, hip arthroscopy has been useful for the evaluation and staging of chondral injury as well as the debridement of loose flaps and removal of free cartilage fragments. Larger cartilage defects may be amenable to cartilage-resurfacing procedures that have been applied in the knee. One author (MJP) has limited experience with autologous chondral transplantation from the lateral femoral condyle. These surgeries have been technically successful, and early follow-up has been encouraging. Microfracture of medium-sized defects has been performed in many patients with full-thickness lesions (Fig. 9).
Chondral flap tear and microfracture. Loose chondral flaps (A) should be debrided back to a stable rim (B). Standard microfracture of the underlying subchondral bone will facilitate the growth of hyaline-like fibrocartilage over the defect (B).
Chondral lesions appear to be a relatively common finding during arthroscopy. McCarthy et al. 75 looked at 436 hip arthroscopies during a 6-year period and found that 261 patients (55.3%) had labral tears. There was a high association of chondral injuries with labral tears in this study: 73% of patients with labral fraying or tearing of the labrum had chondral damage. In addition, a clear decrement in outcome of patients with labral tears has been observed once an associated chondral acetabular lesion of greater than 1 cm occurs (J. C. McCarthy et al., unpublished data, 1997). As in other joints, the long-term consequences of chondral lesions are a major concern. Although symptomatic improvement from arthroscopic debridement of unstable cartilage flaps is encouraging, future advancement in surgical techniques will focus on more predictable cartilage-resurfacing procedures to not only alleviate mechanical symptoms, but also to promote the long-term overall health of the hip joint. 9
Ligamentum Teres Injuries
The function of the ligamentum teres remains unclear. The presence of arteries around the ligamentum suggests a role in providing a blood supply to the developing hip.101 In addition, it has been suggested that this ligament plays a biomechanical role, contributing significantly to the stabilization of the hip. 86 The mechanism of action of the ligamentum involves tightening in hip adduction, flexion, and external rotation. Direct observation during dynamic hip arthroscopy reveals clear tightening of the ligament with the hip in 10° of flexion and external rotation (Fig. 10). Patients suffering from ligamentum rupture as a result of trauma will oftentimes suffer from symptoms of instability and pain. Analysis of the material properties of this ligament has demonstrated similarities to other ligaments and confirms its ability to resist dislocation forces applied to the femoral head. 19 Animal studies have demonstrated significantly greater dislocation rates after surgical transection of the ligamentum teres.76,86
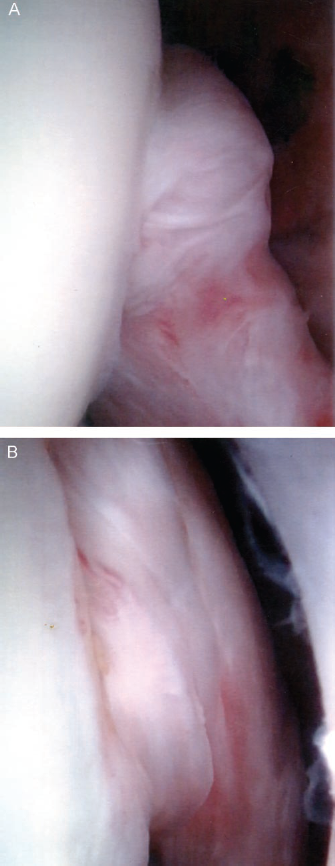
Dynamic hip arthroscopy demonstrates significant tightening of the ligamentum teres during external rotation (A) compared with internal rotation (B) of the hip. These findings support the biomechanical role of the ligamentum teres in the stabilization of the hip.
Injuries to the ligamentum are rarely diagnosed. Rao et al. 86 diagnosed ligamentum teres lesions in 8% of over 1000 hip arthroscopies performed. Gray and Villar 46 described the classification of the lesions seen at hip arthroscopy and noted three groups: complete rupture, partial rupture, and the degenerate ligamentum. Type I (complete) ruptures typically result from either major trauma or surgery and are associated with a high incidence of other hip abnormalities such as labral tears and articular damage. Type II (partial) ruptures have a long history of ill-defined hip pain and may have minor associated hip abnormalities seen at arthroscopy. Type III (degenerate) lesions typically have symptoms of an underlying osteoarthritis. Acute disruptions of the ligamentum are thought to occur as a result of exaggerated movements of adduction and external rotation, 86 although hip abduction is oftentimes the injury mechanism described with patient history. 25 One author (MJP) has seen a high incidence of partial tears of the ligamentum teres in ballet dancers.
Diagnosis of these injuries can be difficult, and a high index of suspicion with careful attention to the injury mechanism and the physical examination are critical to accurate evaluation. Patients with type I (complete) tears commonly report symptoms of painful clicking within the joint, hip stiffness, giving way, and reduced range of motion. Type II (partial) tears are usually associated with groin or thigh pain, limp, and, less commonly, painful clicks or clunks. Type III degenerate ligamentum teres are typically found in a slightly older patient population with concomitant degenerative changes in other structures within the hip joint. Physical examination may reveal decreased range of motion (particularly in extension), pain with motion and straight-leg raising, and, occasionally, locking of the joint. Computed tomography or MR scanning may be useful to identify loose bodies and osteochondral fragments; however, actual visualization of the torn ligament (especially partial tears) is difficult. 86
Arthroscopic examination of patients with persistently symptomatic lesions can clearly demonstrate ligamentum teres abnormalities. Type I ruptures are often associated with attached bone fragments from the femoral head or the acetabulum and are surgically treated with debridement of any loose pieces of ligament and bone. Type II partial ruptures and type III lesions are treated with debridement of loose, frayed tissue. The results of arthroscopic debridement are good; however, outcomes are best in patients with isolated lesions without associated ace-tabular fracture or significant osteochondral defect of either the acetabulum or femoral head. 86
Ligamentum teres injuries in high-impact sports such as football may lead to recurrent subluxation of the hip.20,91 The high incidence of degenerative arthritis associated with complete ligamentum teres ruptures has been attributed to the original injury in many cases. 86 However, recurrent instability and subluxation episodes may cause repetitive vascular compromise to the femoral head and account for an increased incidence of avascular necrosis in these patients. Further biomechanical and basic science research is required to fully delineate the function of the ligamentum teres and thus guide future treatment recommendations.
Snapping Hip
Snapping hip is characterized by an audible snap or pop that usually occurs when the hip is brought through a range of motion. It is often accompanied by pain and generally occurs during physical activity. Three sources of snapping have been described, external (lateral), internal (medial), and intraarticular, with the external type being the most common.1,49 The external type is caused by snapping of either the posterior border of the iliotibial band or the anterior border of the gluteus maximus muscle over the greater trochanter when the hip is flexed from an extended position.1,55,90 The internal type is most commonly associated with painful displacement of the iliopsoas tendon over the iliopectineal eminence 26 or over the femoral head.26,90 The intraarticular type is commonly a clicking sensation caused by a loose body in the joint, such as a fracture fragment, a torn piece of labrum, a chondral flap, or synovial chondromatosis.
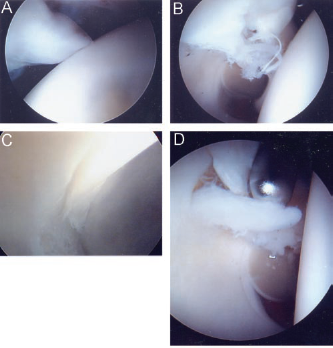
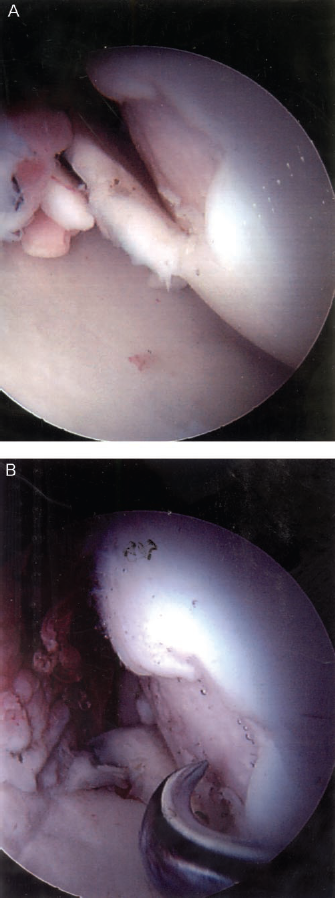
The history and physical examination are usually diagnostic of the source of the snapping hip. Internal snapping is generally localized over the anterior part of the groin, external snapping is localized over the greater trochanter, and intraarticular clicking can be elicited with hip rotation. Nonoperative management, including physical therapy and antiinflammatory medications, is often adequate to relieve symptoms; however, refractory cases may require surgical intervention. 49 Surgical treatment of these conditions has historically required open procedures to lengthen either the iliopsoas tendon or iliotibial band26,35,49,60 or remove the offending intraarticular abnormality. 49 Advancement in arthroscopic techniques has significantly improved the surgeon's ability to address intraarticular sources of hip clicking, as has been previously outlined. These advanced arthroscopic procedures now extend to nonarticular areas and have begun to include removal of posttraumatic periarticular impinging osteophytes as well as iliopsoas and iliotibial band releases for internal and external snapping hip syndromes (Fig. 11). 43 Results from these procedures are preliminary and further study is necessary.
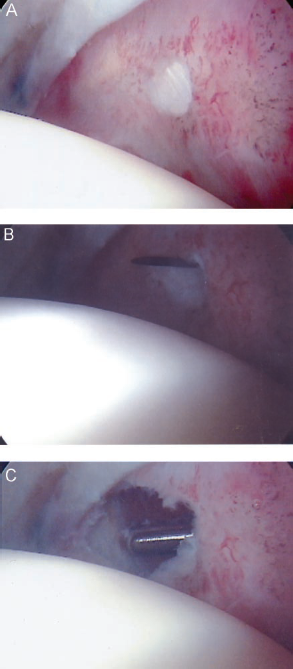
Iliopsoas tendon releases can be performed arthroscopically for symptomatic internal snapping hip. The intraarticular portion of the iliopsoas tendon can be seen in A. After localization of the tendon (B), the intraarticular portion can be released with a motorized shaver (C).
Loose Bodies
Hip arthroscopy is ideally suited for the removal of loose bodies. Loose bodies may or may not be ossified and are readily identified by radiographic studies only when calcium is present. If a loose body is not evident on plain films, CT scans are highly sensitive for visualization; intraarticular fragments may be obscured on MRI. 85 When symptoms persist, these bodies can be readily addressed with minimal associated morbidity through hip arthroscopy. Loose bodies may occur as an isolated fragment, such as after dislocation or with osteochondritis dissecans, or as multiple bodies or clusters, such as in cases of synovial chondromatosis. In cases of multiple bodies, it is essential to fully explore the joint and be sure to remove all fragments. Multiple bodies associated with synovial chondromatosis often adhere to the synovium around the fovea and must be morseled before removal by arthroscopy.
Nonossified loose bodies may be extremely difficult to visualize. In a retrospective review of 94 consecutive patients with refractory hip pain lasting longer than 6 months, McCarthy and Busconi 71 demonstrated that 67% of loose bodies may not be evident on conventional radiographic studies. When persistent symptoms of locking or catching are present, arthroscopy is a way to confirm the diagnosis suggested by clinical examination as well as provide simultaneous treatment.
Other Indications
There are several less common indications for arthroscopic evaluation and treatment of hip symptoms. These include management of osteonecrosis of the femoral head, treatment of synovial chondromatosis and other synovial abnormalities, evaluation and treatment of crystalline arthropathies (gout and pseudogout), infection, and post-traumatic intraarticular debris. In very rare, carefully selected cases, hip arthroscopy may be warranted in patients with underlying mild-to-moderate osteoarthritis when mechanical symptoms predominate.
The current indications for the use of hip arthroscopy in the management of osteonecrosis of the femoral head are narrowly focused. They include arthroscopic staging of lesions, comprehensive mapping of the femoral head and acetabular joint surfaces, and management of mechanical symptoms associated with osteonecrosis. O'Leary et al. 79 found that the presence of mechanical symptoms in patients with osteonecrosis was a favorable prognostic indicator for the success of hip arthroscopy and concluded that the identification of mechanical symptoms is a specific indication for arthroscopy in osteonecrosis. Arthroscopy has no role in end stage disease with complete collapse of the femoral head. Most diagnostic and treatment efforts for osteonecrosis of the femoral head are directed at the subchondral bone to prevent its collapse65,66,94 or toward revascularization, especially with the use of free-vascularized fibular grafting.67,97 Hip arthroscopy can be of further benefit in these cases for visualization of the intraosseous femoral head core track to identify the demarcation of the avascular zone in the subchondral bone and more accurately position the location of the decompression. Arthroscopy can also be performed simultaneously with a core decompression to accurately evaluate the cartilage overlying the necrotic bone as well as to intraarticularly confirm placement of the core track.
Arthroscopic surgery of the hip is useful to facilitate the diagnosis and treatment of both synovial-based disease and systemic diseases primarily affecting the hip joint. 63 Arthroscopy provides a means to improve diagnostic accuracy as well as to treat systemic conditions including synovial chondromatosis, crystalline arthropathies such as gout and pseudogout, and acute septic arthritis. Synovial chondromatosis is a metaplastic synovial condition that produces numerous loose bodies that may be difficult to visualize radiographically if they are nonossified (Fig. 12) (Ref. 85; J. C. McCarthy et al., unpublished data, 1998). Crystalline diseases such as gout or pseudogout can also produce extreme hip joint pain and are characterized by a large-joint effusion, elevated serum uric acid level, and high concentrations of crystal diffusely distributed throughout the joint. Arthroscopic evaluation and treatment of the septic hip allows for simultaneous diagnosis through joint fluid analysis and synovial biopsy as well as decompression and lavage of the joint with minimal morbidity. 18
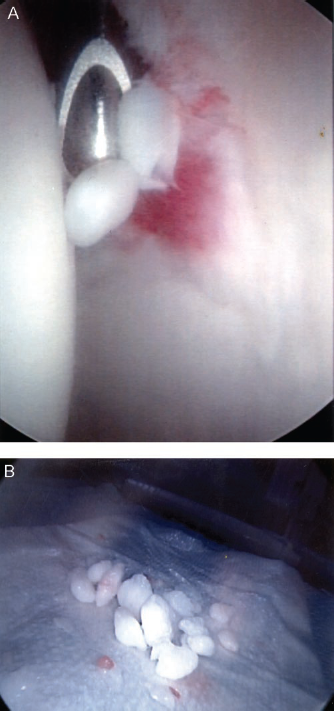
A, synovial chondromatosis results in numerous loose bodies; B, complete exploration of the joint must be performed to assure removal of all fragments.
Patients with other conditions that result in acute and chronic synovitis within the hip, such as inflammatory synovitis, pigmented villonodular synovitis, hemosiderotic synovitis secondary to hemophilia, and chondrocalcinosis, also may benefit from arthroscopic intervention. 63 These synovial and intraarticular abnormalities have all been associated with accelerated joint degeneration, and although the pathologic mechanisms have not been clearly delineated, the clinical description has been advanced by use of hip arthroscopy. 63 In addition, arthroscopy, in contrast to open arthrotomy, minimizes associated risks such as osteonecrosis, heterotopic bone formation, deep vein thrombosis, neurovascular injury, or infection.
Traumatic events around the hip joint are frequent and include fractures of the femoral neck, head, and acetabulum, as well as fracture dislocations. In addition to disruption of the bony architecture, dislocations and fracture dislocations can produce loose bodies, labral injuries, and shear damage to the chondral surfaces of the femoral head or acetabulum.12,31 Pipkin-like femoral head shear fractures can result in the displacement of bone or cartilage from the femoral head into the hip joint as well as injury to the ligamentum teres. Intraarticular foreign bodies, such as bullet fragments, can also affect the hip with or without an associated fracture. 44 Each of these examples of posttraumatic hip injury warrants evaluation and treatment of the associated intraarticular abnormality. Epstein et al. 31 reported that the incidence of chondral damage present after a fracture dislocation of the hip was so high that an open arthrotomy should be performed in every case. With the recent advances in hip arthroscopy, and the high risks of open arthrotomy in the early posttrauma period (such as infection, contracture, deep vein thrombosis, pulmonary emboli, heterotopic bone, and neuromuscular dysfunction), there is increased enthusiasm for a more minimally invasive approach. Although technically challenging, each of these posttraumatic conditions can be successfully addressed with hip arthroscopy. 8
Osteoarthritis
Osteoarthritis results in approximately 200,000 total hip replacements per year in the United States. 19 Many patients have prolonged symptoms that progress over several years and may have disease components that can be alleviated or diminished by arthroscopic surgery before the development of end stage disease. Currently, the role of arthroscopy in the treatment of osteoarthritis of the hip is controversial and needs to be better defined. 19 Several points, however, are well established. The presence of end stage disease with joint-space narrowing, impinging osteophytes, and full-thickness, diffuse cartilage wear, should be treated with total hip arthroplasty. Although it is technically possible and perhaps appealing in some instances, removal of osteophytes is not an indication for arthroscopy as these rim protuberances are late bony expressions of diffuse joint disease. McCarthy and colleagues 75 and Glick 42 have reported a direct correlation between advanced cartilage degeneration, especially on the acetabular side, and poor outcome after arthroscopy.
The appropriate use of hip arthroscopy in patients with osteoarthritis can be optimized by careful consideration of several factors, including the specific patient history, physical examination, diagnostic studies, and severity of arthritic disease. Hip arthroscopy may be considered in patients with mild-to-moderate osteoarthritis, minimal or no deformity, and persistent symptoms. Patients with mild-to-moderate disease who develop mechanical symptoms after minor trauma appear to have the most predictable and reliable relief of symptoms. 19 Arthroscopic treatment of an associated labral tear, chondral flap tear, or loose body, in this situation, can eliminate mechanical symptoms such as buckling, catching, or locking. One author (MJP) has had experience with patients who are undergoing a total hip arthroplasty on one side, with mechanical symptoms on the contralateral side. In this situation, concomitant arthroscopic evaluation and treatment of the contralateral side may be considered to eliminate mechanical symptoms and aid in postoperative rehabilitation from the arthroplasty procedure. Cheilectomy for increased femoral head/neck junction offset or an impinging osteophyte around the acetabular rim may be successfully performed arthroscopically with favorable results (Fig. 13).
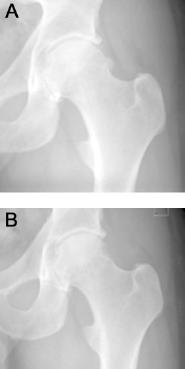
A, preoperative radiograph demonstrating an impinging osteophyte; B, postoperative radiograph after cheilectomy.
Operative Technique
Hip arthroscopy may be performed with the patient in either the supine or lateral position, depending on the surgeon's preference. In either case, distraction of the femoral head from the acetabulum must be performed to fully visualize the articular surfaces. A thorough understanding of the anatomic relationships around the hip joint, with special attention to neurovascular structures and tissue planes, is paramount. Specialized instruments, including flexible probes, extra long cannulas, and extra long specialized instruments such as shavers, burs, drills, and loose body retrievers, all have improved accessibility of the joint and increased the versatility of procedures available to the surgeon (Fig. 2). Initial insertion of long spinal needles (6-inch, 16-gauge needles) allows release of the negative pressure vacuum phenomenon created with joint distraction and also allows for injection of sterile saline for joint distension.
All arthroscopic instruments need to be long enough to traverse the thick soft tissues surrounding the hip and should be passed through sturdy metallic sheaths or cannulas. These cannulas should be kept in position throughout the procedure to prevent loss of joint capsular distension and visualization due to multiple perforations in the hip capsule. This practice also reduces the risk of other complications such as instrument breakage, periarticular soft tissue trauma, intraarticular chondral damage, and neurovascular injury. Most of the intraarticular structures in the hip joint can be seen through the combined use of 30° and 70° arthroscopes as well as the interchange of portals. 73
Patient Positioning
Supine Position.8,10
The advantage of the supine position is that it offers a familiar position for many surgeons. The setup is similar to that used for fixation of hip fractures, including a fracture distraction table with a well-padded perineal post and an image intensifier. The operative hip is placed in a position of slight extension to decrease tension on the sciatic nerve and in approximately 25° of abduction. The foot is well padded, and placed in a traction boot, and distraction of the hip joint is performed under direct fluoroscopic examination. Adequate traction typically requires between 25 and 50 pounds of force. 10 The force necessary for distraction can be reduced by releasing the vacuum within the joint with arthrocentesis and injecting saline solution into the joint. 35 The optimal vector for distracting the femoral head from the bony acetabulum is oblique relative to the axis of the body and runs parallel to the femoral neck rather than to the shaft of the femur. 10 This can be best achieved by applying a lateral force as well as a distal distraction force. Adequate distraction is confirmed with fluoroscopic visualization of joint-space widening in the anteroposterior plane. Gentle traction is also applied to the contralateral limb to provide counterforce.
The anterior aspect of the hip may be adequately visualized with minimal traction. With the hip flexed to 45° and externally rotated to 30°, the anterior capsule becomes relatively patulous and can be distended with saline, making portal entry and visualization of the hip relatively easy. The traction force can then be adjusted as needed to allow inspection of other areas, with concerted effort to limit the periods of distraction with higher forces. One author (MJP) uses a modified supine position technique in which the hip is placed in a position of 10° of flexion, 15° of internal rotation, 10° of lateral tilt, and neutral abduction.
Lateral Position.41–43
The lateral position was popularized by Glick41,42 and Glick et al. 43 and is preferred by some surgeons. The main advantage of this position is that fat drops away from the operative sight when the patient is placed on the side and it provides direct access to the joint along the superior, anterior, or posterior femoral neck. As in the supine position, a fracture table can be used to apply the necessary joint distraction. The principles of joint distraction are identical in both positions. Compared with the supine position in which the anterior portal is often used, the lateral position provides comfortable access to the hip joint via just the anterolateral and posterolateral portals. The trochanter acts as a constant anatomic landmark in this position, and the femoral neck can be used as a palpable structure with the trocar to assist with orientation during instrument placement. Principles of portal placement and arthroscopic technique do not vary with position, and the choice of setup is based primarily on surgeon preference and training.
Portal Placement
Accurate portal placement is essential for optimal visualization and safe access to the hip joint. 95 Typically, three basic portals are used: anterolateral, anterior, and posterolateral (Fig. 14). Various accessory portals have also been described but are not as clinically useful.
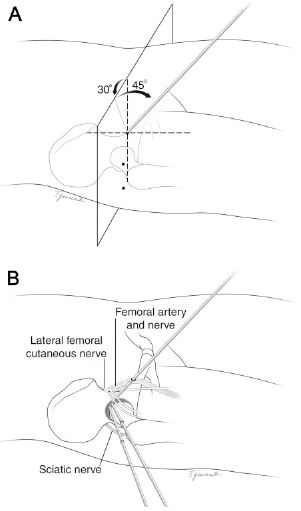
Three portals are traditionally used (anterolateral, posterolateral, and anterior). A, the anterior portal coincides with the intersection of a sagittal line drawn distally from the anterosuperior iliac spine and a transverse line across the superior margin of the greater trochanter. The anterolateral and posterolateral portals lie anterior and posterior to the superior tip of the greater trochanter. B, careful attention to proper portal placement is essential to avoid nearby neurovascular structures.
Anterolateral Portal
The anterolateral portal has also been described as the anterior paratrochanteric portal as it is referenced off the greater trochanter. This portal is placed approximately 1 to 2 cm superior and 1 to 2 cm anterior to the anterosuperior “corner” of the greater trochanter, depending on the patient's weight and size. The anterolateral portal should be established first and should be performed under fluoroscopic guidance. Initially, a spinal needle is placed in the appropriate position with use of the image intensifier. The needle is moved up the neck of the femur until it freely enters the hip joint. Once placement of the needle in the joint is confirmed, the joint is distended with approximately 40 ml of saline solution. A guide wire can then be placed through the spinal needle confirming placement into the hip joint, and a cannulated trocar can then be directly placed over the guidewire into the joint. This sequence of steps confirms appropriate placement and decreases any scuffing or injury to the articular surfaces. Care must be taken not to place this portal too anterior or deep, as this places the femoral neurovascular bundle at risk. 15 This portal allows visualization of the femoral head, the anterior neck, and the anterior intrinsic capsular folds 29 as well as the synovial tissues beneath the zona orbicularis and the anterior labrum. A 70° scope may be used through this portal to assist in visualization. 95
Anterior Portal
If used, the anterior portal is typically the second portal to be established and allows for visualization of the anterior femoral neck, the anterior aspect of the joint, the superior retinacular fold, and the ligamentum teres. 29 Adequate visualization of the anterior labrum or the anterior acetabulum may require the use of a 70° arthroscope. The portal is established by identifying the intersection of the vertical line drawn from the antero-superior iliac spine distally and the horizontal line drawn from the superior surface of the femoral greater trochanter medially. 95 A spinal needle is directed 45° cephalad and 30° medially into the joint. Placement of the needle into the joint can be confirmed with the image intensifier, or may be directly visualized from the arthroscope in the anterolateral portal. A guidewire is then placed, followed by a cannulated trocar in the same manner as previously described. This portal presents the greatest risk to the lateral femoral cutaneous nerve, which lies within several millimeters of the cannula. In addition, the lateral femoral circumflex artery and femoral neurovascular bundles must be protected. 29 The localization of the femoral pulse distal to the inguinal ligament helps prevent inadvertent injury to these structures.
Posterolateral Portal
This portal is also described as the posterior paratrochanteric portal as it is also referenced off the greater trochanter. The entry site is 2 to 3 cm posterior to the tip of the greater trochanter at the same level as the anterolateral portal. The same sequence of steps previously described should be used for establishing this portal. Direct visualization of entry into the joint is possible with the scope in the anterolateral portal. The anterolateral and posterolateral portals should be established parallel to one another. The greatest risk with this portal is injury to the sciatic nerve, which lies approximately 3 cm away.15,95 Advancing the trocar with the femur in a neutral or slightly internally rotated position can protect the nerve, as this maneuver rotates the nerve away from posterior margin of the greater trochanter. This portal is used for visualization of the posterior aspect of the femoral head, the posterior labrum, the posterior capsule, and the inferior edge of the ischiofemoral ligament. 29
Complications
Although many vital neurologic and vascular structures are at risk during hip arthroscopy, the majority of the complications associated with this surgical procedure are related to traction and fluid management. 89 Nonetheless, a thorough understanding of the anatomic vicinity of these neurovascular structures is necessary to avoid injury from inadvertent portal placement. Catastrophic complications such as femoral vascular injury and permanent femoral or sciatic nerve damage should be easily avoided with appropriate surgical planning and preparation.
Sampson 89 has reviewed complications in 530 cases of hip arthroscopy and found a total complication rate of 5.5%. Of these, 0.5% were considered permanent, and 5% were transient. The most common complications were transient neurapraxias of the peroneal, femoral, sciatic, lateral femoral cutaneous and pudental nerves secondary to traction. These complications typically resolved in 2 to 3 days. Complications related to the intraarticular manipulation of instruments included scuffing of the articular surfaces, which occurred in two cases, and instrument breakage, which occurred in two cases (Fig. 15). These complications may be minimized by passing all arthroscopic instruments through sturdy metallic sheaths to prevent multiple attempts at hip joint penetrance and perforations of the hip capsule.73,100 One case of femoral head avascular necrosis was identified. Cartilage scuffing and avascular necrosis were reported as permanent complications. Fluid extravasations into the intrapelvic or intraabdominal regions occurred as a result of either prolonged surgery time or extraarticular surgery, such as iliopsoas release. In some of these cases, paracentesis was required to relieve symptoms. Bartlett et al. 3 reported one case of cardiac arrest as a result of intraabdominal extravasation of fluid during arthroscopic removal of a loose body from the hip joint of a patient with an acetabular fracture. This case required emergent laparotomy to relieve excessive intraabdominal pressure. Careful attention to both the arthroscopy pump and fluid outflow will reduce the incidence of this complication.

Metallic debris on the labrum at revision surgery secondary to instrument breakage during the primary surgery.
Rodeo and colleagues 88 reviewed the complications from arthroscopy and also reported that most complications were neurapraxias resulting from excessive or prolonged traction. Direct trauma to cutaneous nerves, such as the lateral femoral cutaneous nerve, was also identified as a potential source of nerve injury that typically occurs during portal placement. Additional complications related to the application of traction include pressure necrosis of the foot, scrotum, or perineum. These problems can be avoided with close attention to the force and duration of traction, as well as the intermittent release of traction throughout a prolonged procedure. Careful placement and padding of the perineal post as well as adequate padding on the foot will help avoid intraoperative injury to these regions.
Infection is a potential complication of any surgical procedure; however, it has not been reported and is likely to be as rare during hip arthroscopy as it is with arthroscopic procedures of other joints because of the copious amounts of fluid used throughout the procedure. Several authors have suggested that there is a risk of accelerating avascular necrosis of the femoral head during hip arthroscopy and some have even stated that hip arthroscopy is a relative contraindication in patients with an established diagnosis of avascular necrosis.47,100
Conclusion
The application of arthroscopic techniques to the hip joint appears to be the last frontier for the minimally invasive management of intraarticular injuries in athletes. Until the recent advent of improved surgical techniques, advanced imaging modalities, and more versatile instrumentation, the hip joint was largely inaccessible because of numerous anatomic and technical constraints. With these improvements, however, hip arthroscopy can now be performed safely and effectively as an outpatient procedure. The ability to visualize arthroscopically a joint–-that at times is subjected to substantial forces of up to five times body weight during athletic activities such as running and jumping–-has significant implications for the rapid recovery from debilitating intraarticular hip injury in these patients. 81 Many of the athletic injuries to the hip joint discussed in this article, including labral tears, loose bodies, ligamentum teres injuries, chondral injuries, snapping hip, and capsular laxity with iliofemoral ligament deficiency, can be successfully treated with hip arthroscopy in the appropriately selected patient. Patients with reproducible symptoms and physical findings that reveal limited functioning and who have failed an adequate trial of nonoperative treatment will have the greatest likelihood of success after surgical intervention. Strict attention to thorough diagnostic examination, detailed imaging, and adherence to safe and reproducible surgical techniques, as described in this review, are essential for the success of this procedure.