
Abstract
Background: Extensor tendinosis (“tennis elbow”) is a degenerative overuse tendinopathy of the wrist extensors at their attachment to the lateral humeral epicondyle. No treatment has been universally successful. Topical application of nitric oxide has been used effectively to treat fractures and cutaneous wounds in animal models, presumably by stimulation of collagen synthesis in fibroblasts.
Purpose: To determine whether topical nitric oxide can improve outcome of patients with extensor tendinosis.
Study Design: Prospective, randomized, double-blinded clinical trial.
Methods: Eighty-six patients with extensor tendinosis were randomized into two equal groups; both were instructed to perform a standard tendon rehabilitation program. One group received an active glyceryl trinitrate transdermal patch, and the other group received a placebo patch.
Results: Patients in the glyceryl trinitrate group had significantly reduced elbow pain with activity at 2 weeks, reduced epicondylar tenderness at 6 and 12 weeks, and an increase in wrist extensor mean peak force and total work at 24 weeks. At 6 months, 81% of treated patients were asymptomatic during activities of daily living, compared with 60% of patients who had tendon rehabilitation alone.
Conclusions: Application of topical nitric oxide improved early pain with activity, late functional measures, and outcomes of patients with extensor tendinosis.
Tennis elbow, or lateral epicondylitis, is a common cause of chronic elbow pain and wrist extensor dysfunction in adults, especially those between the ages of 35 and 54 years. 10 No treatment is universally successful in managing this condition, which causes considerable time lost to work and recreation. The current best practice management of tendon rehabilitation involves relative rest, forearm bracing, and a graduated stretching and strengthening exercise program. 2
Inhibition of nitric oxide has been shown to reduce collagen content, contraction, and synthesis by wound fibroblasts in vitro. 14 In animal studies, nitric oxide synthase inhibition resulted in a significant reduction in the cross-sectional area and load to failure of healing tendon, 8 suggesting that nitric oxide stimulates collagen synthesis by wound fibroblasts. This hypothesis is a proposed mechanism for nitric oxide modulation of healing in tendons, which rely on fibroblastic production of collagen for repair. The goal of our study was to assess whether application of continuous topical nitric oxide can alter outcome measures in patients with chronic tennis elbow when compared with standard tendon rehabilitation treatment alone.
Topical application of glyceryl trinitrate has been used for over 100 years as a therapy for angina pectoris. 9 It is now accepted that the mechanism of action of the organic nitrates is through production of nitric oxide, the endothelium-derived relaxing factor. Thus, organic nitrates such as glyceryl trinitrate may be viewed as prodrugs of endogenous nitric oxide. 3 In our clinical trial we chose to deliver nitric oxide via transdermal glyceryl trinitrate patches because of the ease of dosing and of application.
The current best practice management for lateral epicondylitis involves a graduated tendon rehabilitation program that begins with relative rest of the injured tendon through avoidance of aggravating activities. Although this treatment has not been scientifically validated, it is anecdotally important, empirically effective, and logically sound. The early use of counterforce braces has been reported, through biomechanical and EMG analysis, to reduce angular acceleration at the tendon origin and to reduce muscle duration responses above the braced area.6,11
Stretching of the tendons of the elbow and wrist is thought to be important for maintaining normal range of motion at these joints, particularly during a period of relative rest, and assists in regaining flexibility. Stretching may also aid tendon healing through gentle longitudinal traction along normal lines of stress. 7
Muscle strengthening is instituted as soon as pain permits and is thought to assist in healing through tensile loading and improved tendon collagen fiber orientation, as well as by gradually restoring lost strength in forearm musculature. Initially, isometric exercises are commenced, and then, as each exercise stage can be performed without pain, increased resistance can be added. Further exercises are gradually instituted, including concentric and eccentric types. 5
In five randomized and controlled clinical trials, corticosteroids have been shown to provide some improvement in elbow pain between 2 and 6 weeks, with no improvement beyond 2 months. 1 For this reason, we decided not to use corticosteroid injections in this clinical trial and to exclude patients who had received this therapy in the preceding 3 months. There is no type II evidence to support ultrasound, laser, and electrogalvanic stimulation in the treatment of lateral epicondylitis, and, for this reason, these measures were neither actively included nor excluded in this trial.
Materials and Methods
The study was designed to meet CONSORT guidelines and was approved by the South Eastern Sydney Area Health Service Ethics Committee. A power analysis determined that, to have a 90% probability of finding a 40% difference between groups, it was necessary to recruit 80 patients for the trial. All subjects were required to be more than 18 years of age. Subjects were excluded if they had extensor tendinosis of less than 3 months' duration, current pregnancy, previous surgery or dislocation of the affected elbow or wrist, distal neurologic signs, or a local corticosteroid injection in the previous 3 months.
The 86 recruited patients were allocated to one of the two clinical trial groups through coded randomization, with 43 patients in each group. This randomization process was controlled by the senior pharmacist in our institution (JN), who also supervised the packaging of transdermal patches and their distribution to patients. Patients in one group received the active transdermal patch (one-quarter of a 5-mg/24-hour Nitro-dur patch, Schering-Plough, Sydney, Australia), and the other group received a placebo transdermal patch (one-quarter of a Nitro-dur demonstration patch, Schering-Plough).
The patches were distributed to the patients by the pharmacist along with a supply of 24 500-mg paracetamol tablets to use for possible headache. The transdermal patches were intact when distributed, and patients were required to cut the patches into quarters before application. Both the patients and the clinical examiner were blinded as to group assignment.
Patients were instructed in the application of the patches at their initial visit. They were informed that the dosing regimen was one-quarter of a transdermal patch to be applied daily to the affected elbow. The patches were to be left in place for 24 hours and then replaced with a new quarter patch. The site of application was demonstrated as immediately distal to the lateral epicondyle of the humerus, and patients were instructed to rotate the patch application site around this point with each new patch application.
At the initial clinical assessment, all patients were instructed in the performance of a tendon rehabilitation program encompassing the current best practice management for extensor tendinosis. The program involved 1) rest from aggravating activities in the early stages (particularly repetitive wrist flexion and extension, repetitive forearm pronation and supination movements, and forceful gripping), 2) the continuous use of a forearm counterforce brace until completion of the first phase of the muscle-strengthening program, 3) regular stretching of the extensor carpi radialis brevis muscle and tendon, and 4) a muscle-strengthening program involving gradually increasing resistance.
At the initial visit and at all subsequent visits, the patient was also required to complete an extensor tendinosis symptom assessment form with use of verbal descriptor scales to rate the severity (0 to 4) of their elbow pain with activity, at rest, and at night. This assessment form was also used to exclude mechanical symptoms in the elbow and to indicate changes in elbow symptoms, either improvement or deterioration.
A single examiner (JAP) assessed each patient and recorded the following: 1) the level of local epicondylar and proximal common extensor tendon tenderness by using a four-point scale (none, mild, moderate, or severe tenderness), 2) handheld dynamometer measurement of resisted third finger metacarpophalangeal extension with a fully extended elbow (Maudsley's test), 3) wrist extensor tendon mean peak force by using a modified chair pick-up test (the Orthopaedic Research Institute Tennis Elbow Testing System, ORI-TETS4,12), and 4) total work as measured by the ORI-TETS. This modified chair pick-up test was performed with the elbow flexed to 90° and with a vertically oriented hand board gripped palm downward and pulled superiorly. The hand board was linked to a load cell, and the readings were stored directly onto a computer's hard drive.
All clinical assessments were repeated at 0, 2, 6, 12, and 24 weeks with an identical format. Records of headaches, paracetamol use, and compliance with patch application and the tendon rehabilitation program were also made at these scheduled visits.
The symptoms and signs used as outcome measures for assessing response to treatment in this clinical trial were patient-rated elbow pain at rest (0 to 4), patient-rated elbow pain with activity (0 to 4), patient-rated elbow pain at night (0 to 4), local epicondylar and tendon tenderness (0 to 3), dynamometer-measured strength with Maudsley's test (measured in newtons), and wrist extensor mean peak force and mean total work as measured by the ORI-TETS (calculated with LabView 5.1 biomechanical software, National Instruments, Austin, Texas).
Outcome measures were analyzed with Sigmastat 2.0 statistical software (Jandel Scientific, San Rafael, California) with use of the Mann-Whitney rank sum test to compare differences between groups and the Wilcoxon signed-rank test to compare differences within the groups. The level of significance was defined at P = 0.05. A chi-square analysis of patient-reported symptom outcomes at week 24 was performed. Effect size estimates were calculated by dividing the mean z-score at week 24 by the square root of the sample size. 13
Results
Eighty-six patients (95 elbows) with a clinical diagnosis of extensor tendinosis were recruited through newspaper advertisements and private consulting rooms. There were 42 men and 44 women, with a median age of 46 years (range, 30 to 74). Bilateral disease was present in nine patients, all of whom were right-hand dominant. In total, 81 of the patients were right-hand dominant; in 16 of these patients, the nondominant side was affected alone. Five patients were left-hand dominant, and four of them had the dominant side affected. The median duration of symptoms was 17 months (range, 3 to 232).
Of the 86 patients originally recruited for the clinical trial, 5 patients in the glyceryl trinitrate patch group had treatment discontinued during the course of the study because of side effects (2 patients had severe and persistent headaches, 2 patients had dermatitis rash, and 1 patient experienced transient facial flushing and angiodysplasia). Of the remaining 38 patients in the glyceryl trinitrate patch group, 2 patients dropped out at the 2-week stage, with no reason given, and 1 patient dropped out at the 3-week stage because of an occupational back injury that required hospitalization. Thus, there were 35 patients (39 elbows) in the glyceryl trinitrate patch group who completed the 6-month follow-up.
In the placebo patch group there were four dropouts. Three of these dropped out within the first 3 weeks of the trial, with no reason given, and the fourth dropped out at the 14-week stage when this patient relocated to another state. Thus, there were 39 patients (41 elbows) in the placebo patch group who completed the 6-month follow-up period. There were no significant differences in the patient characteristics or the drop-out rate between the two treatment groups, and the statistical analysis was made on the basis of intention to treat.
Analysis of the clinical trial outcome measures determined that the data were not normally distributed. A Mann-Whitney rank sum test comparison of the glyceryl trinitrate group compared with the placebo group revealed a significant decrease in elbow pain with activity at week 2 (P = 0.01) (Fig. 1). It was noted that patients in the glyceryl trinitrate group had less elbow pain with activity once treatment began, and this difference continued to the conclusion of the trial at week 24. There was, however, a greater decrease in elbow pain with activity in the glyceryl trinitrate group at the week-2 stage than at any other time period.
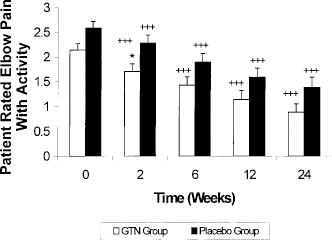
Effects of glyceryl trinitrate (GTN) versus placebo on elbow pain with activity. Statistically significant differences between groups are shown with an asterisk (*, P < 0.05), and significant differences within groups are shown with crosses (+ + +, P < 0.001).
Mann-Whitney rank sum tests comparing lateral epicondylar and tendon tenderness between groups showed a significant decrease in clinically assessed lateral epicondylar and tendon tenderness at week 6 (P = 0.02) and at week 12 (P = 0.02). There appeared to be a trend toward diminishing elbow tenderness over the course of the clinical trial in the glyceryl trinitrate group, especially when compared with the placebo group (Fig. 2).
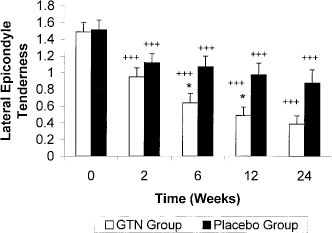
Effects of glyceryl trinitrate (GTN) versus placebo on epicondylar tenderness. Statistically significant differences between groups are shown with an asterisk (*, P < 0.05), and significant differences within groups are shown with crosses (+ + + P < 0.001). The differences at weeks 6 and 12 are significant at the P = 0.02 level.
Mann-Whitney rank sum tests comparing ORI-TETS measurements between groups showed a significant increase in mean peak force at week 24 (P = 0.03) and a significant increase in mean total work at week 24 (P = 0.03). Both the peak force and total work produced by the affected elbow increased over time, with the glyceryl trinitrate group increasing more than the placebo group (Fig. 3).
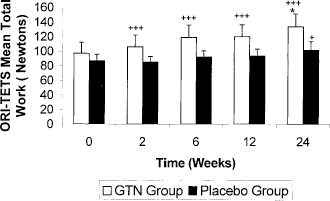
Effects of glyceryl trinitrate (GTN) versus placebo on mean total work as measured by ORI-TETS. Statistically significant differences between groups are shown with an asterisk (*, P < 0.05), and significant differences within groups are shown with crosses (+, P < 0.05; + + +, P < 0.001). The difference at week 24 is significant at the P = 0.03 level.
Within the glyceryl trinitrate group the data were not normally distributed, and analysis with the Wilcoxon signed-rank test showed that all measures at all testing periods were significantly improved compared with the baseline measures at week 0. Patient-reported outcomes at week 24 showed that 81% of patients (35 of 43) in the glyceryl trinitrate group had excellent improvement (asymptomatic with activities of daily living) over the course of the trial; 16% of patients (7 of 43) were unchanged (equivalent to less than 10% worsening or improvement) over the course of the trial; and 2% of patients (1 of 43) rated their elbow as poor (equivalent to worsening by more than 10%) after completion of the clinical trial. This result compared with 60% of patients in the placebo group rating their condition as excellent (26 of 43), 23% as unchanged (10 of 43), and 16% as poor (7 of 43). A chi-square analysis comparing outcomes between the two groups revealed that the glyceryl trinitrate group had a significantly increased (P = 0.005) chance of being asymptomatic with activities of daily living at 24 weeks.
The mean estimated effect size at week 24 was 0.12 (95% confidence interval, 0.06 to 0.19). This measure was derived from the mean P value of all outcome measures at the week-24 stage and was equivalent to a binomial effect size display, or change in patient outcome success rates, of 12%. In other words, from an estimation of the size of the mean effect on outcome measures at week 24 in the glyceryl trinitrate group, it would be expected that the between-groups difference in successful outcome (asymptomatic at week 24) would be 12% of patients.
The reported and observed side effects in the glyceryl trinitrate group included headache in 63% (27 of 43 patients), a dermatitis rash in 21% (9 of 43 patients), facial flushing and cutaneous angiodysplasia in 2% (1 of 43 patients), ipsilateral axillary sweating in 2% (1 of 43 patients), and a feeling of uneasiness/apprehension in 2% (1 of 43 patients). Only 35% (15 of 43 patients) experienced no side effects during the 6 months of the clinical trial.
In the placebo patch group, the reported side effects were headache in 58% (25 of 43 patients), and a dermatitis rash in 9% (4 of 43 patients). Between the two groups, there was no significant difference in the number of days affected by headache or of the amount of paracetamol required for headache during the course of the trial.
The glyceryl trinitrate group reported a total of 136 days with at least one headache, which was equal to an average of 5 days (2% of clinical trial days for those with headache) per person of those patients who experienced this side effect. The median was 3 days of headache, with a range of 0 to 16 days. The patients who had headaches required a total of 214 paracetamol tablets (500 mg) during the course of the clinical trial. The average number of paracetamol tablets required for headache over the 6-month period was 8 tablets, with a median of 4 tablets and a range of 0 to 38 tablets.
The placebo patch group reported a total of 166 days with at least one headache, which was equal to an average of 6.5 days (2% of clinical trial days for those with headache) per person of those patients who experienced this side effect. The median was 1 day of headache, with a range of 0 to 34 days. A total of 250 paracetamol tablets (500 mg) were used by patients who had a headache during the course of the clinical trial. The average number of paracetamol tablets required for headache over the 6-month period was 10 tablets, with a median of 0 tablets and a range of 0 to 90 tablets.
Discussion
The group of patients with extensor tendinosis at the elbow who had continuous topical glyceryl trinitrate therapy demonstrated significantly reduced elbow pain with activity at 2 weeks, reduced lateral epicondylar and tendon tenderness at 6 and at 12 weeks, and improved elbow peak force and total work (as tested by ORI-TETS) at 24 weeks. These effects of topical nitric oxide were in addition to the significant improvement of all measures at all testing periods; 81% of the patients in the glyceryl trinitrate group were asymptomatic during activities of daily living and rated their elbow as excellent after the 6-month clinical trial. This result compared with 60% of patients in the placebo group who were asymptomatic during activities of daily living at week 24. The mean estimated effect size at week 24 was 0.12, which is equivalent to a binomial effect size display or change in patient success rate of 12%. 13 This figure is comparable with the 21% improvement with topical nitric oxide therapy noted in patient-rated outcomes.
These results are consistent with the hypothesis that topical glyceryl trinitrate therapy can modulate tendon healing and lead to significant improvements in symptomatic and functional outcome measures at the 6-month stage beyond that achieved through tendon rehabilitation alone. It is known that healing tendon, like most human soft tissues, relies on fibroblastic production of collagen for repair. Perhaps provision of exogenous topical nitric oxide to the degenerated tendon can substitute for any reduced levels of nitric oxide or for nitric oxide synthase. This application of topical nitric oxide may stimulate wound fibroblasts to increase collagen synthesis and remodeling. Other potential mechanisms for this demonstrated improvement include increased blood supply to the region due to local vasodilation or increased clearance of local inflammatory mediators or bioactive proteins, such as substance P. There is also a possibility that nitric oxide has an effect on neural structures at a local level that may modulate pain.
It must be reinforced that supplementing nitric oxide through transdermal glyceryl trinitrate patches does not lessen the necessity for an accompanying tendon rehabilitation program, which includes rest from aggravating activities, early protective bracing, stretching, and a system of gradually increasing exercises. If collagen synthesis in the tendon is increased through application of topical nitric oxide, this increase, along with appropriate rehabilitation, should lead to the development of a strong scar along appropriate lines of tension for the wrist extensors.
The tendon rehabilitation program that was used in this clinical trial was home-based and not strictly controlled except through verbal checks of compliance at each examination. It still afforded excellent results and also led to increased tendon strength and ability to perform work at each testing period.
The duration of the average episode of extensor tendinosis is estimated to be between 6 months and 2 years. 10 The patients in our clinical trial had chronic extensor tendinosis, with a median duration of symptoms of 17 months. Their results indicated that a structured tendon rehabilitation program can be successful in treating extensor tendinosis, even if home-based and unsupervised. Patient compliance was excellent, with no patient excluded because of lack of compliance, and this may be because of the thorough explanation of the rehabilitation program, both verbal and written, because of the regular examinations and checks of compliance, or because of the personalities of patients enrolling in clinical trials.
The major side effects of this medication were headache, weakness or dizziness (symptoms of hypotension), and local skin irritation or rash at the application site. It is wise to exercise caution in the use of glyceryl trinitrate in patients with marked anemia, current pregnancy, a history of hypersensitivity to organic nitrate drugs with prior episodes of hypotension or of migraine headaches, or those on diuretic therapy. A relative contraindication to glyceryl trinitrate therapy is severe ischemic heart disease, especially if the patient requires other nitrate vasodilators for angina pectoris. Obviously, the use of glyceryl trinitrate therapy in patients with concomitant ischemic heart disease requires careful planning in consultation with a cardiac physician.
It was necessary to discontinue 12% of patients (5 of 43 patients) in the glyceryl trinitrate group because of the severity of side effects, most notably headache (5%) and local dermatitis (5%). The only other serious side effect (not reported previously in the literature or in product information) was facial flushing and angiodysplasia in 1 patient (2%) that was reversible after discontinuation of the glyceryl trinitrate therapy. This patient had type II diabetes, and this side effect was probably due to facial arteriolar dilatation. These side effects occurred despite a continuous dosing regimen aimed at achieving a tolerance to the vascular effects of nitric oxide and an application policy of rotating the location of the patches around the lateral epicondyle to avoid repetitive application to the same area of skin. It is important for patients to maintain adequate hydration, and hence blood volume, during nitrate therapy. 15 The incidence of side effects was not significantly different between groups, although the incidence of reversible side effects severe enough to warrant discontinuation of therapy was higher in the glyceryl trinitrate group.
Among the patients receiving topical nitric oxide therapy who remained in the study and experienced headache, the average incidence was 5 days of the 6-month period, or 1 day of headache per month. The fact that no increased incidence of side effects was noted in the glyceryl trinitrate group may explain why there was not a significant difference in drop-out rates between the two groups.
All topical therapies may cause cutaneous lesions in patients with contact allergies or sensitive skin, and this is something that cannot be easily avoided. It is known that there is variable transdermal glyceryl trinitrate absorption across a population, with five-to-tenfold individual variability, 15 and this may explain the differing severity of side effects such as headache.
Conclusions
The results of this clinical trial demonstrated that there were significant improvements in symptoms, clinical signs, provocative functional tests, and patient outcomes in patients with extensor tendinosis treated with topical nitric oxide therapy (glyceryl trinitrate application) when compared with tendon rehabilitation alone. This is the first clinical trial of this therapy that we are aware of that shows patient- and examiner-determined subjective and objective improvements in outcome for tennis elbow.
Clearly, more research needs to be done in this area to define the exact mechanism of action of nitric oxide in tendon healing, to confirm the validity and reproducibility of the results, and to delineate the most effective dosage regimen to maximize effect and limit side effects. It is also important to determine the reason for treatment failure in the 19% of patients who did not improve and to fully elucidate the role and effects of nitric oxide in tendon healing and rehabilitation. However, because this is a well-tested medication in humans and there are no irreversible side effects in healthy subjects, there does appear to be a role for use of continuous topical nitric oxide therapy in the treatment of patients with chronic extensor tendinosis in combination with a comprehensive tendon rehabilitation program.