
Abstract
Background: Criteria are needed for measuring the effects of exercise and fatigue on proprioception.
Purpose: To measure knee joint proprioception in healthy subjects before and after exercise and to establish a reference for further comparisons of patients with knee injuries.
Study Design: Controlled laboratory study.
Methods: We tested proprioception in the knees of 24 healthy subjects with a mean age of 24 years and median Tegner score of 5. Subjects were tested to estimate their thresholds for detecting slow passive motion, from starting positions of 20° and 40° before and after cycling on an ergometer bicycle until the pulse rate reached a steady state level and they reached a score of 14 to 17 on Borg's Ratio of Perceived Exertion scale.
Results: After cycling, significantly higher threshold values were found for perception of movement toward flexion from both 20° and 40°. No significant differences were seen in measurements of movement toward extension.
Conclusions: Knee joint proprioception seems to be impaired by exercise or training.
Clinical Relevance: This impairment may lead to defective dynamic stabilization of the joint, leading to an increased risk of injuries.
Stability of the knee joint depends on passive soft tissue restraints, joint geometry, compressive forces, cartilage friction, and tension in the surrounding muscles. 15 It has been shown that activity in the muscle spindles is influenced, via gamma motoneurons, by joint and ligament receptors.15,16,29,32 These receptors are located in different joint structures, such as the capsule, menisci, collateral ligaments, and cruciate ligaments and contribute to the overall proprioception of the knee.14–17,32 The aim is to maintain balance and control of limb movements to attain optimal stability and minimize the risk of injury in any situation.12,16 This balance and control also requires input from receptors in other joints, muscles, and skin, as well as from visual and vestibular information.8,15 Fatiguing exercise increases joint laxity24,31,33,34,36 and modifies the afferent information from the muscles via chemical agents such as lactic acid, which may affect joint stability.5,8,15,25,26
Skinner et al. 30 found a significantly poorer ability to reproduce a given change in joint angle after fatigue, as did Lattanzio et al. 20 However, Marks and Quinney 23 noted no change in subjects’ ability to reproduce angles after exercise. Skinner and colleagues 30 reported that the threshold for detection of passive movement in the knee joint did not change significantly after fatigue. Exercise, without fatigue, has been shown to improve the position sense in active positioning measurements. 3
As in studies of proprioception in ACL-deficient knees, the lack of criteria for measurements makes the results difficult to interpret and compare.8–11,27,28 Therefore, more studies are needed to determine possible effects of various types of exercise and fatigue on proprioception and to arrive at standardized measurements for estimating knee joint proprioception. The aims of this study were to 1) measure knee joint proprioception in healthy persons before and after a short period of exercise with methods that have been shown in our previous studies to be both sensitive and reproducible,8-11,27,28 and 2) establish a reference point for further comparisons of patients with knee injuries.
Materials and Methods
Twenty-four healthy young persons, mainly students at the University Hospital in Lund, were tested. Their mean age was 24 years (range, 20 to 32), and 13 were women. Most of them participated in various sports. Their median score on the Tegner activity scale was 5 (range, 2 to 9), equal to strenuous work or leisure time sports such as running on uneven ground about twice a week. 35 The subjects had no history of major orthopaedic lesions or general diseases that would interfere with peripheral proprioception. The Research Ethics Committee at Lund University Hospital approved the study, and all subjects gave their written informed consent to participate.
Proprioception Test
Before exercise we measured proprioception on a specially designed apparatus consisting of a platform on the floor (Fig. 1). Mounted at one end was an electric motor with a wire connected to a movable T-shaped sled with a plastic splint attached to it for fixation and positioning of the lower limb and foot. A metal bar in the center of the platform fixed the sled, and a pull by the wire in either direction made it turn like the hand of a clock along the natural arc of extension or flexion of the knee. The arrowshaped tip of the sled pointed to an analog scale to record movements in increments of 0.25°. The use of ball bearings allowed movements with little friction. The subject lay in the lateral decubitus position, with the lower foot in the plastic splint. The splint supported the posterolateral part of the lower leg but also had a slight anterior curve. The oversized construction allowed for differences in the girth of the lower leg. Two bars mounted on the platform served as guides for placing the thigh and trunk in a standard position, with the hip joint semiflexed. The knee joint was carefully positioned in the rotator center. Tape marks on the surface allowed proper positioning of the knee in the different starting positions of knee joint flexion: 20° and 40°. The upper thigh and hip rested on a rubber pillow (which could be adjusted for different heights, due to more extreme varus/valgus angulations), and pillows were also placed under the back to help the subject relax during the test. Care was taken to eliminate any external stimuli to limb movement except those from the knee joint and surrounding structures. All subjects wore short pants and thick woolen socks, and the knee had no contact with the underlying surface to minimize cutaneous sensations during the tests. Visual control of the leg was eliminated by the subject's position, and auditory impulses were prevented during the threshold trial by use of earmuffs and by playing a tape recording that imitated the sound of a motor.
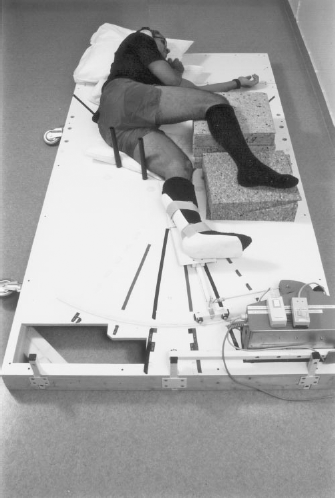
The setup for proprioception testing.
The threshold measurements were made of movements of the knee toward extension and flexion from two starting positions, 20° and 40°. The subjects were asked to close their eyes, concentrate on their knee, and respond when they felt any sensation of movement, changed position, or “anything going on” in their knee. The tape recorder was then turned on, and, with a delay of 5 to 15 seconds, the motor started to move the leg with a calibrated angular velocity of 0.5 deg/sec in the knee. When the subjects responded, the motor was stopped, and the movement was registered in degrees. The median value of three consecutive trials was used for statistical analysis.
The different starting positions were chosen to be within the working range of the knee during ordinary weightbearing activities or training. Because range of motion may differ between individual subjects, the most extreme joint positions were excluded. Thus, tensions in the muscles, capsule, and ligaments were kept below high levels, and more variable tissue tensions between individual subjects were avoided, so that the subjects could relax without having their leg forced into maximum extension.
A slow speed was chosen to ensure that the subjects could not detect a sudden onset of motion and to make testing more difficult than if a higher speed had been used. 11 Because the subjects had been placed in a lateral decubitus position, comparisons between flexion and extension could be made without any uncontrolled effect of gravity. 11
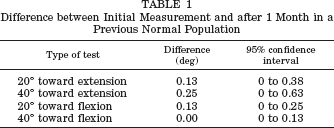
The tests were made on both the left and the right legs by shifting the apparatus arrangement from one side of the platform to the other. This type of apparatus has been used in previous investigations.8-11,27,28 No statistical differences were found between two measurements with an interval of 1 month when subjects in a previous control group were measured, 11 as seen in Table 1. The standard error of the mean was calculated for all the measurements and ranged between 0.04° and 0.11°.
Difference between Initial Measurement and after 1 Month in a Previous Normal Population
Exercise Protocol
A bicycle ergometer was used to exercise the subjects. The aim was not for the subjects to perform strenuous exercise causing extreme fatigue but to approximate the level of normal leisure sports such as jogging, aerobics, or tennis. The subjects wore a heart-rate monitor during the entire trial. The load on the bicycle was first adjusted to fit the subject's approximate ability by asking whether it was too light or too heavy. Subjects were asked to cycle energetically for 5 to 10 minutes with a constant pedaling speed of 60 revolutions per minute. The median effect was 150 W (range, 100 to 200), equal to 900 kpm/min. The initial pulse rate before cycling was a mean value of 98 beats per minute (range, 61 to 152). Some subjects had rather high initial pulse rates; this may have reflected high mental tension and nervousness among them because they were unused to testing situations, as some commented. When the clock was started, they began to cycle. Their pulse rate was taken every minute. They were asked to estimate their level of exhaustion on Borg's Ratio of Perceived Exertion (RPE) scale, 2 which ranges from 6 to 20; 6 is “no exertion at all,” 13 is “somewhat hard,” 15 is “hard,” 17 is “very hard,” and 20 is “maximal exertion.” This scale is closely related to physiologic variables affected by exertion, such as heart rate and blood lactate concentration. 2 When subjects reached a steady state of pulse rate, with no difference in heart rate exceeding 5 beats per minute between measurements at 1-minute intervals, and a level of exertion of 14 to 17 on the RPE scale, the subjects immediately lay down on the apparatus for measurement of proprioception. The pulse rate after cycling was 163 beats per minute (range, 138 to 196) and after the measurement was 93 beats per minute (range, 63 to 121). The median cycling time was 6 minutes (range, 5 to 8), long enough to increase blood lactate levels. 18
Statistical Analysis
Because there seemed to be no proprioceptive difference between the left and right legs, 11 the mean of both legs (right + left/2) was used for the analyses. Comparisons between the measurements were performed by using pairwise t-tests. The significance level was set at P < 0.05. Statistical analyses were performed with the Minitab 10 (Minitab, State College, Pennsylvania), SAS 6.10 (SAS, Cary, North Carolina), and SPSS 11.0 (SPSS, Inc., Chicago, Illinois) program packages.
Results
When the measurements for each starting position were analyzed before and after cycling, comparisons showed no significant effect on threshold of perception of movement toward extension from 20° and 40°. Toward flexion, significantly higher threshold values, indicating poorer proprioception, were found from both starting positions (P = 0.025 for 20° and P = 0.003 for 40°) (Table 2).
Comparison of Threshold Values (in Degrees) before and after Exercise

Mean ± standard deviation.
Significant difference.
Discussion
A matter of concern when these results are discussed is the small magnitude of observed differences, in mean values, between the measurements and the clinical relevance of these possible changes. Within the limitations of what is currently known, we cannot establish using our measurement method how much proprioception may be decreased before the result is clinically relevant. However, it is important to note that group comparisons may show discrete, but statistically significant, differences in threshold values, whereas comparisons between individual subjects may show large differences.8-11,27,28 It should also be emphasized that the estimated conscious proprioceptive ability, in this case the threshold to detection of movement value, likely is the “tip of the iceberg” in the complex conscious and unconscious neuromuscular system controlling balance, joint movement, and stability. It is very difficult to estimate to what degree the observed changes reflected the status of the whole system.
The results of the present study indicate that short-term cycling may reduce knee joint proprioception. This result is supported by a previous experimental study that showed primary muscle spindle afferents, which contribute to proprioception, have reduced capability to discriminate between different muscle lengths after fatigue. 26 Gamma motoneurons that innervate the muscle spindles and affect the spindle outflow are often referred to as the fusimotor system. 12 The activity in the fusimotor system is increased because of fatigue, and the effect seems to be reflex-mediated by chemosensitive group III and IV muscle afferent fibers.21,22 Metabolic products of fatigue, such as bradykinin, 5-hydroxytryptamine, and lactic acid, are thought to cause this effect. A resultant, mainly excitatory, effect on the primary and secondary muscle spindle afferents has been observed in both heteronymous, homonymous, ipsilateral, and contralateral muscles.4,5 The effect on proprioception is suggested to be negative because of an increased similarity in the fusimotor drive on individual afferents in ensembles of muscle spindle afferents, producing a decrease in the response variability. 26 We have no evidence that we actually caused fatigue in the study setup, but earlier findings imply that an increase in blood lactate is likely to occur during these circumstances. 18
Thus, it seems to be well established that local muscular effects occur during fatigue that may negatively affect proprioception,4,5,13,21,22,25,26 but little is known about joint receptors during exercise. No biochemical changes in the synovial fluid associated with muscular fatigue that may affect joint receptors have, to our knowledge, been described. However, a direct effect on the knee joint receptors may occur because fatigue increases joint laxity,24,31,33,34,36 which, by changing the elastic properties of the ligaments containing collagen, may modify the response of the receptors.
Clinically, we have found three studies evaluating the effects of fatigue on knee joint proprioception20,23,30 and one on the joint position sense during nonfatiguing exercise. 3 The findings of Lattanzio et al., 20 who reported a reduction in proprioception after fatigue, support the results of our study to some extent.
Skinner et al. 30 reported that healthy subjects had more difficulty in reproducing a knee joint angle after fatigue but showed no significant change in threshold. They interpreted their findings as supporting the view that muscle receptors play a significant role in the conscious appreciation of joint position.
In contrast, Marks and Quinney 23 detected no effect of muscle fatigue on knee joint position sense. However, they induced fatigue by having the subject contract the quadriceps muscle 20 times, which likely was less fatiguing than the exercise used by Skinner et al. This exercise also mainly affected the anterior structures of the thigh. Therefore, the posterior structures, which are of afferent importance during extension, were probably less affected by fatigue. Moreover, Marks and Quinney used active positioning and active reproduction, whereas Skinner et al. 30 used passive positioning and active reproduction, which may also explain the difference in results. In the study by Bouët and Gahery, 3 the participants improved their joint position sense (active reproduction) after a warm-up exercise, cycling on the ergometer bicycle for 10 minutes at their own pace. With regard to the results of Marks and Quinney 23 and Skinner et al., 30 this raises the question of whether an initial improvement is followed by a “fatigue threshold,” above which muscles perform worse, functionally and proprioceptively.
The lack of difference in threshold before and after fatigue in the study by Skinner et al. 30 does not conflict with our findings because they measured the threshold only toward extension; we also did not detect differences between before and after exercise of perception of motion toward extension. Our measurements showed a significant reduction in thresholds only for motion toward flexion, which again may underline the role of the muscle spindles. Our fatigue test was cycling, which, in our setup without toe clips, can be thought to activate the quadriceps muscle more than the hamstring muscles.6,7 The measurements of flexion, which stretch the quadriceps muscle, may therefore be more affected if muscles play a significant or dominant proprioceptive role. In the study of Skinner et al., 30 the fatigue protocol, including running, probably affected the hamstring muscles more, which was one of their aims, and they ascribed their intact threshold values after fatigue to an enhancement of capsular receptors due to inadequate muscle receptor function. Even though the lack of knowledge about joint receptor characteristics during exercise is obvious, as mentioned earlier, some authors seem to believe in reduced activity of these receptors during fatigue, rather than an enhancement.1,19,20
In the present study, an effect of laxity on the knee joint receptors was unlikely. Fatigue-induced laxity may not have occurred; Nawata et al. 24 have shown that laxity does not occur until after 20 minutes of running, and no subject in the present study cycled more than 8 minutes.
Theoretically, fatigue may increase the time of reaction, which, in the present setup, would be seen as higher threshold values. However, this would presumably affect both flexion and extension measurements, which was not seen.
In conclusion, we found that a short period of moderate exercise can reduce proprioception, which may affect the neuromuscular control of the knee joint and, thus, may make it more susceptible to injuries. No conclusions regarding the origin of the proprioceptive loss can be drawn from the results in this study, nor about the effect of fatigue on subconscious reflective afferent information.