
Abstract
Background: Recent concussion management guidelines have suggested that athletes with mild (grade 1) concussions may be returned to play if asymptomatic for 15 minutes. The purpose of this study was to assess the utility of a current concussion management guideline in classifying and managing mild concussion.
Hypothesis: High school athletes diagnosed with a grade 1 concussion will demonstrate measurable decline in neuropsychological functioning that persists during the 1st week of recovery.
Study Design: Prospective study designed to evaluate neuropsychological functioning both prior to and following concussion.
Methods: Forty-three high school athletes completed neuropsychological test performance and symptom ratings prior to the season and at two times during the 1st week following mild concussion.
Results: Thirty-six hours after injury, mildly concussed high school athletes demonstrated a decline in memory (P < 0.003) and a dramatic increase in self-reported symptoms (P < 0.00001) compared to baseline performance.
Conclusions: Athletes with grade 1 concussion demonstrated memory deficits and symptoms that persisted beyond the context in which they were injured. These data suggest that current grade 1 return-to-play recommendations that allow for immediate return to play may be too liberal.
Clinical Relevance: A reconsideration of current concussion grading systems appears to be warranted.
The diagnosis and management of concussion in athletes has become an intensely debated topic in sports medicine. 16 The heightened interest in this issue is a direct result of increased awareness of the potential adverse impact of sports-related concussion on brain function and is based on a desire to promote safe participation in contact sports. Over the past decade, recognition of the potential danger of concussion has lead to the development of multiple concussion management guidelines that have variably stressed the importance of the presence/absence and duration of different markers of concussion such as loss of consciousness (LOC), amnesia, or disorientation (see Johnston et al. 16 and Collins et al. 8 for a discussion of current concussion guidelines). These guidelines have undoubtedly provided valuable assistance to team medical personnel and have generally lead to a greater degree of caution in managing the injury. However, to date, none of these guidelines has undergone scientific validation, and there is continued controversy regarding their utility in predicting safe return to play.
One of the most commonly used grading systems is the American Academy of Neurology (AAN) practice parameter. 18 Although this protocol for concussion management has been adopted by some sports medicine practitioners, its implementation has not been universal and has been limited by continued questions about its ability to predict safe return to play, particularly at the mild end of the spectrum. There have also been continued questions regarding the lack of research support for this and other guide-lines.8,13,15,16 Within the AAN guidelines, diagnosis of a grade 1 concussion is made on the basis of the following criteria: 1) transient confusion, 2) no LOC, and 3) concussion symptoms or mental status changes that resolve within 15 minutes of injury. With regard to the practice options that accompany the AAN guidelines, the grade 1 practice option recommends removal from the game with return within the same contest if post-concussive symptoms (for example, headaches, dizziness) or mental status changes clear within 15 minutes of injury.
As a result of continued questions regarding the clinical management of concussion, the American Orthopaedic Society for Sports Medicine (AOSSM) sponsored a workshop in 1997 to examine current concussion management practices in sports medicine and to make general recommendations for the diagnosis and treatment of the injury. The deliberations of this workshop were subsequently published in 1999 and have been widely quoted and referenced. 29 The AOSSM workshop reinforced the need to hold athletes with any post-concussive signs or symptoms from return to play until they were asymptomatic. Similar to the AAN practice parameter, the AOSSM guidelines recommended a 15-minute cutoff period for differentiating the mildly from more severely injured athlete. It was further suggested that athletes who manifested signs or symptoms of concussion that lasted less than 15 minutes could be permitted to return to play during the same contest. However, in making this recommendation, the authors noted that this suggestion was based on prevailing clinical practice rather than on research. One of the most important outcomes of the AOSSM workshop was a call for ongoing research designed to clarify issues regarding severity classification and return to play. In addition, participants in this workshop specifically stressed the need for research with younger athletes. Finally, the use of neuropsychological testing in the clinical care of the athlete was specifically recommended, and its use in continued research was supported.
Reflecting an ongoing need to reevaluate concussion management practices, several authors of the AAN and AOSSM guidelines, as well as other concussion researchers, recently met at an international conference in Vienna and agreed that no single grading system adequately addresses all of the pertinent issues.1-3 This conference took place in October of 2001 and was cosponsored by the International Ice Hockey Federation, the International Olympic Committee, and the Federation Internationale de Football Association. In keeping with both the AAN and AOSSM workshop recommendations, the Vienna conference emphasized that symptomatic athletes should be withheld from returning to play. The Vienna group further suggested that no athlete should be returned to play until they were medically evaluated, regardless of whether their symptoms lasted 15 minutes or less. This represented a significant departure from previous concussion management guidelines and reflected recognition of the arbitrary nature of the 15-minute cutoff. As was the case with the AOSSM guidelines, the use of neuropsychological testing was recommended as a valuable tool for assisting in the return-to-play decision-making process.
The development of a better understanding of mild concussion is important for several reasons. First, concussions that fall within the grade 1 classification undoubtedly represent the most common type of concussive injury that may be difficult to diagnose on the field. Athletes who have suffered a mild injury or “ding” injury, by definition, have not experienced a LOC and may not show obvious on-field signs of concussion. The athlete may pass basic sideline tests of memory and concentration and may also deny symptoms in an attempt to hasten his or her return to play. 19 In addition, the mental status changes that occur following grade 1 concussion are assumed to resolve quickly, and injured athletes are often cleared to return to play during the contest within minutes of the injury.8,18 However, this assumption has recently been challenged by data indicating that concussion signs and symptoms may evolve over time and may not be evident initially after injury. 12 Given this presumption of rapid resolution of neurologic difficulties, mildly concussed athletes may not be provided with proper follow-up evaluation that includes medical evaluation and/or neuropsychological testing. In addition, returning a concussed athlete to the field may lead to long-term neuropsychological dysfunction or in rare circumstances severe disability or death.6–7
The study of mild concussion is particularly important with regard to younger athletes as this group represents one of the largest groups of competitive athletes at risk for injury. However, published research in this area has been scant, and almost all research has largely been limited to collegiate athletes.4-23 To date, only a handful of studies exist, and studies employing neuropsychological testing have been particularly rare. McCrea and his colleagues25–26 have recently published data on both high school and college athletes using the Standardized Assessment of Concussion, a brief mental status examination. When concussed athletes were compared to their own baseline test results, the overall total score dropped significantly when tested immediately after a suspected concussion and returned to baseline levels within 48 hours. However, more sophisticated neuropsychological testing was not conducted, so it is uncertain whether recovery was complete by 48 hours. Recently, Lovell and his colleagues 20 have documented memory deficits that persisted days after injury in mildly concussed high school athletes, but neurocognitive speed and reaction time were not specifically investigated. Along similar lines, Collins et al. 9 has also documented the relationship between a decline in neuropsychological test performance and postconcussion headache in concussed high school athletes.
The purpose of this current study is to investigate recovery from concussion in a sample of high school athletes who have experienced grade 1 injuries with no LOC and on-field signs and symptoms that resolve within 15 minutes of injury. Mildly concussed athletes were evaluated at 36 hours and 6 days postinjury via a computerized neuropsychological test battery (ImPACT), 24 and their performance was compared to preseason baseline testing. Report of post-concussive symptoms as well as changes in memory, reaction time, and processing speed are documented and compared to baseline levels.
Methods and Materials
Participants in the study were 43 high school athletes with grade 1 concussion. The average age of the subjects was 15.6 years (range, 13 to 18). Thirty-five of the concussed athletes were male and 8 female. A total of 24 athletes were injured playing American football, 8 playing soccer, 5 playing basketball, 2 playing ice hockey, 2 playing lacrosse, 1 playing baseball, and 1 playing softball. It was the intention of this study to provide preliminary data regarding the recovery of athletes with grade 1 concussion by the AAN guidelines. All subjects were screened for learning disabilities and attention deficit disorder in an attempt to limit the potential confounding effect of these variables on the recovery process. 8 Athletes with a history of either learning disabilities or attention deficit disorder were therefore excluded from this current study.
All athletes participated in a concussion safety program through the Sports Medicine Concussion Program at the University of Pittsburgh. All participants in the program had completed baseline neuropsychological tests during the preseason prior to sustaining contact. The results of this baseline neuropsychological assessment provided the standard of comparison if the athlete was injured throughout the school year. Following a suspected injury, initial sideline mental status testing and an evaluation of signs/symptom assessment are completed to assist team medical staff in making return-to-play decisions following concussion. In addition, neuropsychological testing is conducted in the days following injury to further assist team medical staff in making return-to-play decisions. Athletes were included from high schools within the states of Pennsylvania, Michigan, Illinois, Oregon, and Maine. Athletes were not financially compensated for participation in the program.
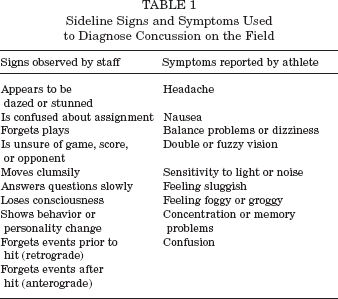
Appropriate Institutional Review Board approval was granted through the University of Pittsburgh. Administration of the ImPACT computerized neuropsychological test battery was supervised by a team of clinical neuropsychologists, athletic trainers, and/or physicians who were trained in the administration of the measures. Training was completed at each site by the primary authors (MRL and MWC). This training involved an educational program designed to teach team athletic trainers and physicians to properly identify signs and symptoms of concussion on the field and sideline (see Table 1). Team staff members were trained in administration of a brief mental status examination (see Table 2), which was completed on the sideline immediately following injury. In addition, staff members were instructed in the use of the ImPACT program by the primary authors (MRL and MWC). Data acquisition forms were standardized, and all personnel involved were also trained in their use. ImPACT is a computer-based, standardized neuropsychological test battery designed to be administered via a computer network. Therefore, all subtests were administered in a standardized manner, and the test was scored automatically by the computer program.
Sideline Signs and Symptoms Used to Diagnose Concussion on the Field
Sideline Mental Status Evaluation Used to Diagnose Concussion on the Field a
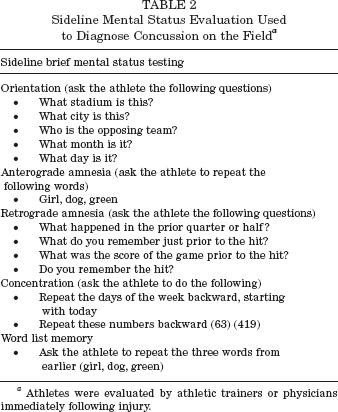
Athletes were evaluated by athletic trainers or physicians immediately following injury.
Baseline ImPACT data collection was initiated prior to the 2000 and 2001 athletic seasons. All baseline data were collected prior to preseason contact drills. Baseline testing included completion of the neuropsychological measures, the symptom inventory, and standardized collection of relevant demographic and medical history variables. Regarding concussion history, ImPACT contains a standardized concussion history questionnaire that was administered under the direct supervision of the test administrator.
Postconcussion Evaluation
High school athletes within our sample experiencing a cerebral concussion during the 2000-2001 athletic seasons were referred for postinjury ImPACT evaluation within 72 hours of injury, with the majority of athletes being evaluated within 36 hours (mean = 1.4 days, SD = 0.8, median = 1 day). A second evaluation was completed for all subjects between 5 and 10 days postinjury (mean = 6.3, SD = 1.4, median = 6). In-season concussions were diagnosed during the athletic contest based on one or more of the following criteria: 1) any observable alteration in mental status or consciousness on the field, rink, or court; and/or 2) the presence of LOC and/or presence of amnesia as identified by an on-field examination (as reviewed in Table 2); and/or 3) any signs/symptoms following a collision involving the head or body (as reviewed in Table 1). Initial diagnosis of concussion was made by certified athletic trainers or team physicians who were present on the sideline at the time of injury and who performed the initial evaluation. Even though athletes were diagnosed with grade 1 concussions, no athletes in this study were returned to play prior to completing the two follow-up evaluations.
During the course of the current study, medical staff at participating institutions carefully documented information pertaining to a concussed athletes’ immediate, on-field presentation of postconcussion markers of injury. Based on the sideline assessment, all athletes included in this study were documented to be symptom free within 15 minutes of their injury and thus were retrospectively classified as having a grade 1 concussion (according to the AAN guidelines). Specifically, no athlete in the sample exhibited disorientation, amnesia, LOC, or signs/symptoms of injury that persisted beyond 15 minutes of their concussive injury.
Neuropsychological Test Procedures
ImPACT consists of seven individual test modules that measure multiple aspects of neurocognitive functioning including attention, verbal and visual memory, reaction time, and information processing speed. The test battery yields memory, reaction time, and processing speed composite indices that provide summary information in these cognitive domains. Prior studies have examined the sensitivity of the reaction time and processing speed composite scores and have found these indices to be sensitive to the effects of concussion.9,19,20 A more thorough description of the ImPACT test battery and rationale for the development of the individual tests has been described in detail previously. 24
The memory composite index of the ImPACT test is structured to assess multiple aspects of memory including verbal (word) learning and recognition memory, visual associative memory, visual working memory, and verbal (letter) memory. This composite score is presented as the average percentage correct for these five subtests. The reaction time index consists of the weighted performance on three different reaction time subtests, and performance is expressed in the units of hundredths of a second. The processing speed index represents the weighted average of three tests that measure visual-motor speed and visual scanning. In addition to the three neurocognitive composite scores, ImPACT also yields a 21-item Post-Concussion Symptom Scale that is now being widely used throughout the National Football League, National Hockey League, and amateur sports.21,22,24 This scale consists of symptoms commonly associated with concussion (for example, headache, dizziness, nausea, sleep disturbance) that are scored from 0 (asymptomatic) to 6 (severely symptomatic).
Statistical Analysis
All statistical analyses were completed using Statistical Package for the Social Sciences (SPSS). 28 Repeated measures analyses of variance were used to determine if mean memory and symptom scores differed across the three assessments. This statistical model allows a direct comparison of postinjury test scores and symptoms to preinjury levels of functioning. In addition to allowing for a direct analysis of the overall change in test scores over the multiple assessment periods, this model also allows for a specific comparison of test scores at different points during the 1st week after injury (for example, baseline versus 36 hours, baseline versus day 6). In addition, magnitude of change is represented through effect size statistics.
Results
Prior Concussion History and Neuropsychological Test Performance
The potential importance of concussion history in determining recovery from mild concussion was evaluated by comparing the baseline neuropsychological performance of athletes with and without a history of prior concussion. Athletes with a prestudy history of concussion did not differ statistically from those with no concussion history on baseline memory testing (t = -0.14, P < 0.90) or with regard to reaction time (t = - 1.16, P < 0.26) or processing speed (t = 1.23, P < 0.22). They also did not differ significantly with regard to number of symptoms reported at baseline (t = 0.70, P < 0.50).
Postinjury Neuropsychological Test Performance
Descriptive statistics for memory processes, processing speed, reaction time, and symptom ratings are presented in Table 3. The means and standard deviations of the mildly concussed athletes across baseline and two follow-up evaluations (36 hours and day 6) are displayed in Table 3. The pairwise comparisons between athletes at baseline and the designated follow-up times are illustrated in Figures 1 through 4.
ImPACT Composite Scores and Post-Concussive Symptoms a
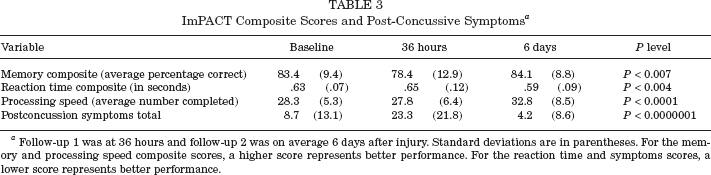
Follow-up 1 was at 36 hours and follow-up 2 was on average 6 days after injury. Standard deviations are in parentheses. For the memory and processing speed composite scores, a higher score represents better performance. For the reaction time and symptoms scores, a lower score represents better performance.
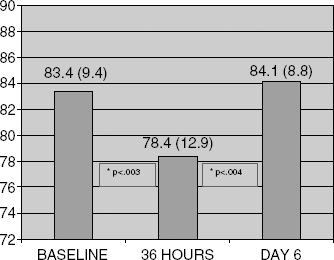
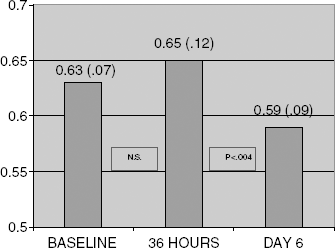
Mean performance on the ImPACT memory composite across three evaluation periods. Scores are expressed as percentage correct. Standard deviations are in parentheses. A higher score represents better performance. Pairwise comparisons are provided between baseline and 36 hours and between 36 hours and day 6. Mildly concussed athletes demonstrate significantly poorer memory performance at 36 hours postinjury and a return to baseline levels at day 6.

Mean performance on the ImPACT symptom inventory at baseline, 36 hours postinjury, and 6 days postinjury. Standard deviations are in parentheses. A higher score represents a greater number of symptoms. Pairwise comparisons are provided between baseline and 36 hours and between 36 hours and day 6. Mildly concussed athletes demonstrate significantly more symptoms at 36 hours postinjury and a drop in symptoms to below baseline levels at day 6.
Mean performance on the ImPACT reaction time composite at baseline, 36 hours postinjury, and 6 days postinjury. Standard deviations are in parentheses. A lower score indicates better (faster) performance. Pairwise comparisons are provided between baseline and 36 hours and between 36 hours and day 6. Mildly concussed athletes show no initial change followed by better than baseline performance at day 6.
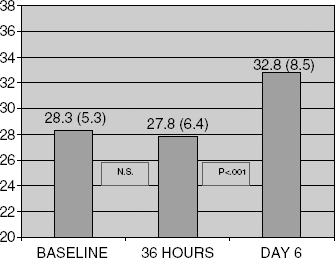
Mean performance on the ImPACT processing speed composite at baseline, 36 hours postinjury, and 6 days postinjury. Standard deviations are in parentheses. A higher score indicates better (faster) performance. Pairwise comparisons are provided between baseline and 36 hours and between 36 hours and day 6. Mildly concussed athletes show no initial change at 36 hours followed by better than baseline performance at day 6.
For the memory composite score, there was a significant difference in performance across the evaluation periods, F(2, 41) = 5.9, P < 0.007, epsilon > .93, eta squared = .22, with an initial drop in performance and return to baseline levels by the time of the second follow-up, 6 days postinjury. This is a medium to large effect size. Specifically, pairwise comparisons revealed significantly lower memory scores at 36 hours postinjury compared to baseline (P < 0.003, d = .45, medium effect size), with significantly improved memory between the first and second follow-up periods (P < 0.004). There was no significant difference between memory at baseline and at 6 days postinjury.
For the symptom total score, there was a significant overall main effect, F(1.6, 65.4) = 27.9, P < 0.0000001, indicating significant change across the assessment periods. Pairwise comparisons revealed significantly greater symptoms at 36 hours postinjury than at baseline (P < 0.00001, d = .84, large effect size), followed by a precipitous drop in the report of symptoms between the first and second follow-up evaluations (P < 0.0000001). Moreover, the athletes reported fewer symptoms at the time of the second follow-up than at baseline (P < 0.02).
With regard to reaction time, there was a significant difference in test performance between baseline and postconcussion evaluations, F(2, 41) = 6.5, P < 0.004. Pairwise comparisons revealed no difference in reaction time between baseline and the first evaluation (36 hours) but significantly faster reaction time at 6 days postinjury than at baseline (P < 0.007) and at 36 hours postinjury (P < 0.004).
For the processing speed composite score, there was also a significant main effect for time, F(2, 41) = 9.4, P < .0001, epsilon > .91, eta squared = .32, P < 0.0001. Pairwise comparisons revealed no difference in processing speed between baseline and the first evaluation (36 hours) but significantly faster processing speed at 6 days postinjury than at baseline (P < 0.002) and at 36 hours postinjury (P < 0.001).
A total of 11 subjects reported no symptoms at 36 hours postinjury and 7 exhibited normal (above baseline) neuropsychological test performance. Overall, only 4 athletes had both normal neuropsychological test performance and no increase in symptoms at 36 hours postinjury.
Discussion
This study was designed to evaluate neurocognitive recovery in high school athletes following mild (grade 1) concussion. We found a clear decline in memory processes and an increase in the self-report of symptoms during the first few days of recovery in a group of high school athletes who fit within the grade 1 concussion classification. The decline in memory and increase in report of symptoms was statistically significant and was associated with a medium to large effect size. By 6 days postinjury, the athletes had returned to at or above their baseline level of functioning in all areas.
In addition to finding large changes in memory and symptom reporting in mildly concussed athletes, this study found subtle but statistically nonsignificant declines on reaction time and processing speed tests at 36 hours postinjury. However, at the time of the second follow-up evaluation, 6 days postinjury, mildly concussed athletes demonstrated a significant improvement in both of these areas compared to initial postinjury performance levels. There are a number of possible interpretations of this finding. It may be that mental speed (as measured by the reaction time and processing speed indices) is not affected to the extent that memory processes are following mild concussion, although the reaction time and processing speed indices have been found to be sensitive to concussion in a mixed severity level group of concussed athletes. 19 It is notable that performance on the reaction time and processing speed scores did improve significantly (compared to both baseline and 36 hours postinjury) by the time of the second follow-up evaluation 6 days postinjury. This may represent a practice effect associated with the repeated evaluation of athletes over a relatively brief period of time. Practice effects represent improvements in performance as a result of the athlete's repeated exposure to the test on more than one occasion. Although computer-based programs such as ImPACT minimize these effects, some athletes may show a small improvement due to practice. Therefore, the absence of this apparent practice effect at the time of initial follow-up may be suggestive of an initial decrement in mental speed. This performance pattern has been described in prior studies of concussion. 4
This study provides evidence of statistically significant changes in symptom reporting and neuropsychological test performance during the 1st week of recovery from mild concussion. Effect size statistics are included to further demonstrate the magnitude of these changes. Regarding the clinical significance of these changes, this is an important and somewhat controversial issue. Some authors have suggested the adoption of reliable change index scores to establish cutoffs for determining abnormal performance following concussion. 15 This approach provides confidence intervals to help separate changes in test performance due to clinical change from change due to other factors such as test error. However, since recent standards for return to play following concussion have emphasized that no athlete should be returned to play while symptomatic, assigning a “minimally tolerable” level of symptoms would appear to be premature and potentially dangerous at this time.
It is an assumption of this article, as well all current including concussion guidelines, that premature return to play exposes athletes to additional risk of more serious brain injury and leads to a worsening of symptoms and lowered threshold for reinjury. This assumption has been based on clinical experience as well as on the phenomenon of second impact syndrome,6–7 which may result in the death or serious injury of younger athletes who experience a second injury following incomplete recovery from an initial injury. In addition, early animal studies have suggested that concussed injured rodents are vulnerable to further injury during the initial days following a first injury. Prospective studies with symptomatic and asymptomatic athletes who did and did not return to play would no doubt help to clarify this issue. However, research of this nature is not ethically justifiable due to the potential increased risk of injury in athletes who would be returned to play while still symptomatic.
Overall, the findings of this study suggest a delay of cognitive recovery beyond the 1st day following injury in mildly concussed high school athletes. Collectively, these findings are alarming given that athletes in this study did not show clear evidence of on-field mental status changes such as sideline confusion or amnesia lasting longer than 15 minutes and were reported to be completely symptom free within this same time period. Based on existing AAN and AOSSM classification parameters alone, all of the athletes in this study potentially could have been cleared to return to play during the contest during which they were injured, potentially risking more severe injury.6–7 However, given the individualized nature of our program, this did not occur until a postinjury evaluation, which included neuropsychological testing (ImPACT) that was completed on average within 1 week of injury. It is also important to emphasize that, based on measurable memory decline on the computerized neuropsychological battery and a reported increase in post-concussive symptoms in the days following injury, many of these athletes would have later been reclassified as grade 2 concussions. However, given the structure of existing guidelines, their injuries would have initially been classified as grade 1, and these athletes may have been returned to play during the same contest in which they were injured.
The results of this study have relevance regarding the diagnosis and treatment of mild concussion in high school athletes for two primary reasons. First, mild concussion, as defined by grade 1 classification, assumes transitory mental status changes early after injury. This represents the “ding” type of injury, which has frequently been reported in the literature and has become part of the vernacular of the sports medicine practitioner. 27 These current results challenge the assumption, common among high school athletes, that “having ones bell rung” represents an innocuous or rapidly resolving injury. Second, our results affirm the need for careful examination of mental status changes in athletes following injury to ensure that these athletes are indeed back to normal, prior to returning to play. In our opinion, this should not only involve the brief sideline assessment of the athlete's mental status and other signs and symptoms of concussion, but should, whenever possible, involve neuropsychological evaluation in the days following injury. The neuropsychological testing completed in this study detected subtle changes that were not evident following more brief initial mental status testing on the sideline or subsequently evolved in the days following injury. This finding also emphasizes the importance of reexamining the athlete at several points in time to ensure that the athlete's condition is not deteriorating. Changes in mental status may not be immediately apparent on the field and may evolve over minutes or hours. This study did not examine ImPACT performance within the same day of injury (for example, at halftime, between periods, or immediately following the contest). Examination of ImPACT performance closer to the time of injury may help to clarify our understanding of the evolution of concussive signs and symptoms within the minutes to hours following injury. This issue will be addressed in future studies.
This study suggests that the current return-to-play criteria for grade 1 concussion in high school athletes may not be conservative enough. Therefore, reconsideration or reformulation of traditional grade 1 classifications may be warranted. These results also affirm the need for continued research regarding this issue, particularly in younger athletes. The results of this study lend support to the new summary and agreement statement from the Vienna conference that recommends removal of an athlete from the game following any diagnosis of concussion on the field, rink, or court. Based on the Vienna conference recommendations and the results of the current study, the individualized medical evaluation of the concussed high school athlete is recommended using detailed on-field mental status testing, serial assessment and medical follow-up of signs and symptoms, and follow-up neuropsychological testing, whenever possible.
In addition to raising questions about the utility of the current guidelines in making return-to-play decisions, this article also suggests the need for further research in younger (high school and younger) athletes. Not only do younger athletes represent the largest group of athletes who participate in organized collision sports, but younger athletes are also less likely than college/professional athletes are to receive sophisticated on-field medical care. This is particularly true at the pre-high school and recreational level where no trained medical personnel are present to adequately assess and diagnose a concussion. Therefore, far more research effort needs to be directed toward the establishment of return-to-play practices that maximize protection of younger athletes from premature return to play. In addition, given current concerns regarding recovery from concussion in younger athletes, the concentration of research on athletes younger than the age of 18 appears to be particularly justified.
Although the data presented within this article provide support for the Vienna conference recommendations, these data represent the results of only one study and as such require further investigation and replication. It is also important to note that this study used only high school athletes, and the relevance of these findings to both collegiate and professional athletics is unknown. Given previous laboratory and clinical studies completed with more severely head-injured children.5,14 it is possible that younger athletes may be at higher risk for neurocognitive decline following concussion than adults are. However, this has yet to be established for milder concussive injury. As noted earlier in the article, we are hopeful that studies that directly address the efficacy of concussion management guidelines will lead to improvement in their diagnostic accuracy.
Finally, the use of functional neuroimaging techniques 17 and electrophysiological measures has recently proven to be useful in the evaluation of concussion and deserve further investigation. 11 This line of research should help to better establish the link between clinical indicators of concussion (such as on-field symptoms/neuropsychological test results) and changes in brain physiology. The relationship between clinical recovery and return to normal brain function is currently poorly understood, although there is an assumption that a decline in neurocognitive status reflects underlying brain dysfunction. We are also hopeful that future studies that employ functional neuroimaging technology such as fMRI will help to clarify this relationship.