
Abstract
Background: Ligaments and tendons do not gain mechanical properties of the native tissue after injury or grafting.
Purpose: To determine the influence of platelet-derived growth factor on tendon graft remodeling.
Study Design: Laboratory animal study.
Methods: Forty-eight sheep underwent anterior cruciate ligament reconstruction and were sacrificed after 3, 6, 12, and 24 weeks. In 6 animals at each time point, platelet-derived growth factor was locally delivered via coated sutures. After mechanical testing, tissue samples were taken for histologic, immunohistochemical, and electron microscopy evaluations.
Results: With platelet-derived growth factor treatment, cross-sectional area was significantly lower at 3 and 12 weeks. Load to failure was significantly higher at 6 weeks. Tensile stress was significantly higher at 3 and 12 weeks. Crimp length was significantly higher at 3 and 6 weeks. Vascular density was significantly higher at 6 weeks. Electron microscopy showed a significantly higher collagen fibril amount at 12 weeks. Differences in these parameters at other time points were not significant.
Conclusions: There were alterations in several but not all time points. The local application of platelet-derived growth factor alters the tissue’s mechanical properties during free tendon graft remodeling after anterior cruciate ligament reconstruction. Growth factors present a promising tool toward the complete mechanical restitution of a healing ligament substitute.
The replacement of the ruptured ACL by a free autologous tendon graft is a well-established procedure to restore normal knee stability. 17 The nonvascularized tendon graft subsequently undergoes a process of remodeling after implantation into the intra-articular environment by means of reorganizing its cellularity and extracellular matrix structure, the so-called ligamentization.3,56 The process of graft tissue remodeling has been extensively studied in the past with respect to revascularization, changes in cell morphology and distribution, collagen fiber reorganization, and restoration of extracellular matrix protein distribution.2,9,10,14,32,38,39 During this remodeling period, the grafted tissue shows a decrease of its mechanical properties, and it might be vulnerable to a mechanical overload, possibly leading to injury in terms of early rerupture or persistent tissue elongation. Therefore, today's rehabilitation protocols protect the grafted tissue from repetitive overloading during that vulnerable period, and the return to strenuous activities is delayed to a later point in time.
In recent years, the use of growth factors has been thought to accelerate ligament and tendon healing to allow for an earlier return to unrestricted activity.22,23,34,36,55 Growth factors such as platelet-derived growth factor (PDGF), transforming growth factor-B (TGF-B), basic fibroblast growth factor (bFGF), and epidermal growth factor (EGF) have a well-known positive effect on fibroblast proliferation, the synthesis of extracellular matrix proteins, and revascularization.15,21,25,31,47,48 The local application of PDGF has been shown to successfully improve mechanical properties of the medial collateral ligament (MCL) after injury.7,19,28 Although a positive effect of PDGF on ACL fibroblasts has also been demonstrated,18,26,31,44,47 no data on its potency to improve ACL healing or free tendon graft remodeling after ACL reconstruction are available.
Therefore, our research question was whether the local long-term application of PDGF using a biodegradable drug delivery tool biomechanically and histologically influences free tendon graft remodeling after ACL reconstruction in a sheep model.
Materials and Methods
Study Design and Operative Procedure
Forty-eight skeletally mature female sheep were used in this study. Animals underwent replacement of the ACL in an open fashion, using an ipsilateral flexor tendon graft. 50 All animals were screened to ensure good physical condition. Procedures were performed with approval of the local institutional review board (Reg. No. 0325/98) in accordance with the National Institute of Health guidelines for the use of laboratory animals.
Four groups were assigned, and animals were sacrificed after 3, 6, 12, and 24 weeks (n = 12 for each group). At each time point, 6 animals received the growth factor, and 6 animals served as an untreated control.
Anesthesia was induced intravenously with thiopental sodium. After intubation, anesthesia was maintained with isoflurane and nitrous oxide. The left hindlimb was shaved and prepared in the standard sterile fashion. Through a posterolateral skin incision, the calcaneus communis tendon was exposed, and the Achilles tendon was carefully separated from the superficial digital flexor tendon. The superficial digital flexor tendon, approximately 7.5 cm in length and having a diameter of approximately 6 mm, was sharply dissected. The incision was closed in layers using polyglactin and polyamidic sutures. Two strong polyester sutures (No. 5 Ethibond) were passed through each end of the tendon grafts in an interdigitating whipstitch fashion.
Using straight needles, 4 polyglactin sutures (2-0 Vicryl rapid, Ethicon GmbH, Norderstedt, Germany) were longitudinally inserted into the center of the graft. Before insertion, sutures were coated with poly(D, L-lactide) (molecular weight 30 KD; Boehringer Ingelheim KG, Ingelheim, Germany) as a drug delivery vehicle (300 μg/suture) in a technique described by Schmidmaier et al. 46 In 6 animals at each time point, recombinant human PDGF isoform BB (R&D Systems GmbH, Wiesbaden, Germany) was incorporated into the coating (5% total coating mass), resulting in approximately 60 μg of growth factor per grafted tendon. Finally, the graft diameter was determined, and the tissue was kept moist in saline-soaked gauze until insertion.
The knee joint was exposed through an anteromedial incision. 1 The patella was displaced laterally, the anterior fat pad was sharply separated, and the plica synovialis and the ACL were exposed and removed. A tunnel was drilled from the original tibial insertion site of the ACL in an inside-out direction in 90° of knee flexion. The tunnel diameter was sized in increments of 0.5 mm according to the previously measured graft diameter. In maximum knee flexion, the femoral tunnel was created in the 1-o'clock position in the same fashion, leaving approximately 2 mm of the dorsal femur cortex. The graft was then inserted via the holding sutures using a Beath pin.
For femoral graft fixation, a suture button (EndoButton, Smith & Nephew Inc, Andover, Mass) was attached, so that a minimum of 2 cm of the graft tissue was in the femoral tunnel. The knee was then taken through several full ranges of motion under 90 N of graft pre-tensioning using a tensiometer (Sulzer Orthopedics Ltd, Baar, Switzerland). For tibial fixation, the sutures were tied over a bony bridge that was created at the tibial tunnel exit site (Figure 1). Graft fixation was performed in 60° of knee flexion. The incision was closed using polyglactin and polyamidic sutures. The animals were then returned to their cages and were allowed to bear full weight without restriction of motion.

Schematic drawing of the ACL reconstruction technique used in the present study.
Mechanical Testing
Animals were sacrificed with thiopental sodium followed by an overdose of potassium chloride. The knees were harvested, leaving the joint capsule, the collateral ligaments, the menisci, and the cruciate ligaments intact. The specimens were wrapped in saline-soaked gauze and were stored at −20°C until testing. Twelve hours before testing, the knees were thawed at 4°C. The tibial and femoral bone ends were cleaned from all remaining soft tissue and were embedded in aluminum cylinders using polymethyl- methacrylate. During all preparations and testing, specimens were kept moist with saline spray. All mechanical testing was performed according to a consensus recommendation for ACL testing in sheep.12,13 As a control, 10 intact ACLs and 6 time zero reconstructions were tested in contralateral knees harvested at sacrifice.
The drawer tests were performed in 90° of flexion and neutral rotation with an anteroposterior (AP) femoral load application. The knee was mounted to a materials testing machine (Zwick 1455, Zwick GmbH, Ulm, Germany) in a custom-made adjusting device. 50 To determine neutral knee position, an AP force of 25 N in both directions was applied. The construct was then adjusted in a way so that the area of linear laxity in the hysteresis curve was parallel to the x-axis. After adjustment, an AP force of ±50 N was applied 3 times with a load displacement rate of 1 mm/s. The third hysteresis curve was recorded and transferred to in-house software, and the AP displacement was quantified. After AP drawer testing, all soft tissue including the menisci was removed, leaving only the ACL, while the specimen was still mounted to the testing machine. Each specimen was visually checked in the apparatus before testing to ensure that the femoral condyles were congruent with the tibial plateau without any compression force between them, so that the graft was directly exposed to the applied load. The anterior drawer test (50 N, 1 mm/s) was then repeated, and drawer stiffness and absorbed energy were calculated from the hysteresis curve.
After drawer testing, the tendon cross-sectional area was determined, according to the technique described by Ellis. 16 An area micrometer (Mitutoyo Inc, Osaka, Japan) with different-sized slots and a force transducer (±0.1 N) was used. After resecting the medial femoral condyle, each measurement was performed 3 times at the midsubstance portion of the graft, and the average was recorded.
For failure testing, specimens were mounted to a custom-made adjusting device that allows free rotation of the construct in different knee flexion angles. 50 The ACL graft was carefully aligned parallel to the axis of the applied load in 60° of knee flexion. With a preload of 1 N and a load displacement rate of 1 mm/s, specimens were loaded until failure. Maximum load to failure and stiffness were determined from the load displacement curve. Maximum load to failure and cross-sectional area data were used to determine tensile stress.
Histology
Tissue samples, approximately 5 mm in length, for histologic examinations were taken from the midsubstance portion of the grafted tissue away from the failure site after mechanical testing was completed. Samples were fixed in 5% buffered formalin at room temperature for 48 hours. For conventional light microscopy inspection, staining was performed according to Masson Goldner's trichrome stain and hematoxylin and eosin. Samples were evaluated using a high-resolution microscope (Leica DMRB, Leica GmbH, Bensheim, Germany) linked to a digital image analyzing system (KS 400 Imaging System Release 3.0, Carl Zeiss Vision, Eching, Germany) using conventional and polarized light microscopy. Two longitudinal sections were evaluated per specimen, and cell counts were performed at regular intervals along the length of the section. Five randomly chosen regions were evaluated per section, and the mean cell density was calculated. Measurement of crimp length was performed with the use of a calibrated scale under polarized light. Ten regions (0.44 × 0.44 mm2 each) were measured in each section, and the mean crimp length was determined.
Assessment of Vascularity
After sacrifice, the contralateral flexor tendon, the native contralateral ACL, and the graft tissue were harvested from the midsubstance portion and fixed in 5% formalin for 48 hours at room temperature. The samples were sliced into longitudinal and cross sections. Thereafter, specimens were dehydrated and embedded in paraffin. The 4-μm- thick sections were cut and mounted on slides coated with 3% silane (Sigma Chemical, St Louis, Mo).
For detecting the endothelial surface cells of blood vessels, tissue was immunostained with antihuman von Willebrand factor (rabbit antihuman von Willebrand factor, Kat No: A 0082, DAKO, Glostrup, Denmark).49,51 The slides were hydrated and pretreated with 0.1% protease (protease, type XIV: bacterial, Sigma-Aldrich Chemie GmbH, Steinheim, Germany) for 10 minutes at 37°C. After blockage of nonspecific binding sites with 10% normal horse serum (Vector Lab Inc, Burlingame, Calif) for 20 minutes at room temperature, the antibody was diluted 1:200 and applied to the samples overnight in a humidity chamber at 4°C. The tissues were then rinsed in TBS buffer and incubated with biotinylated horse antimouse immunoglobulin G secondary antibody (Vector Lab Inc) for 30 minutes at room temperature. Slides were again immersed in TBS buffer, after incubation for another 50 minutes with an avidin-biotin complex (ABC kit, Vector Lab Inc) linked with alkaline phosphatase as a reporter enzyme. Staining was visualized using Neufuchsin as a chromogen. Finally, the sections were counterstained with methylene-green for a few seconds, dehydrated, and mounted in a xylol-soluble mount (Vitro-Clud, R Langenbrinck, Emmendingen, Germany).
To analyze revascularization, 2 transverse sections of each specimen were evaluated. First, in routine stains, the margin between the synovial surface and the collagen fibers of the graft was identified. For immunohistochemical evaluations, each section was subdivided into a subsynovial (adjacent to the synovial layer) and a central zone. To do so, the midpoint of the cross sections was defined, and the distance between the synovial/subsynovial margin and the midpoint was divided into the 2 distances. Five representative regions (0.06 mm2 each) in the subsynovial and in the central zone were evaluated. Every positively stained vessel section was counted. To control background staining due to unspecific binding sites, negative control specimens were incubated with buffer instead of using the antibody. As positive controls, well-vascularized skin samples of sheep were used. There were no vessels without a clear positive signal after immunostaining.
Transmission Electron Microscopy
To study collagen fibril characteristics and composition, tissue samples from the midsubstance portion were fixed in glutaraldehyde and prepared for transmission electron microscopy (TEM). The fixed specimens were longitudinally cut into 4 to 6 sections under a stereomicroscope (Leica, Wild MPS 28, Heersburg, Switzerland) to confirm cross-banding as proof that collagen fibrils were being viewed and for proper longitudinal sectioning. The sections were then rinsed 3 times, 10 minutes each, in 0.1 mol/L sodium cacodylate buffer solution, followed by postfixation overnight with 1% OsO4. After rinsing them 3 times again the following day, the samples were dehydrated in graded alcohols and embedded in epoxy resin (Agar 100, DDSA, MNA mixture, Agar Scientific Ltd, Essex, UK).
Cross and longitudinal 1-μm sections were cut for light microscopic inspection using an ultramicrotome (Ultracut, Reichert-Jung, Vienna, Austria). After detecting the region of interest, this region of each specimen was manually trimmed with a razor blade, and ultrathin sections (35 nm) were cut using an ultramicrotome and a diamant knife (Diatome MX3474, Diatome, Fort Washington, Pa) and transferred onto coated 3-mm 100-mash nickel grids (Graticules Ltd, Tonebridge, UK). Floating on droplets of uranyl acetate and lead citrate, the sections were stained. Electron microscopic examination took place using an electron microscope (Zeiss EM 10, Karl Zeiss, Jena, Germany). Six photographs of randomly selected areas of each ACL, flexor tendon, and graft tissue were taken at a magnification of 8000. Locations of all specimens with artifacts and cellular components were excluded.
The negatives of each photomicrograph were transferred onto a light box, and 2 regions of each micrograph were photographed using a 1600 × 1200-pixel digital camera (Nikon CoolPix 990, Nikon, Düsseldorf, Germany). When possible, areas of obliquely cut and blurry fibrils were excluded to prevent measuring mistakes. Each of these digital images was composed of 9 μm, out of which a standardized field corresponding to 2 μm was analyzed at a magnification of 80 000, using interactive image- processing software (KS 400 Rel 3.0, Carl Zeiss Vision, Jena, Germany). To prevent errors due to obliquity of sectioning, the minimum diameter of each fibril was measured. Fibrilar structures with a diameter of 20 μm or less were excluded to prevent wrong results due to measurement of microfibrils or of noncollagenous components. A minimum of 5000 fibrils was assessed per specimen to ensure correct fibril distribution. The collagen fibril diameters of each analyzed graft were grouped into 6 size ranges, using intervals of 40 nm, starting at a diameter >20 nm and including an open class (>220 nm) as previously described by Bosch et al. 9 The following parameters were determined: amount of fibrils per μm2, individual collagen fibril diameters, and percentage of area covered by collagen fibrils in 2 μm2. From each specimen, 12 regions (2 μm2 each) were measured at a magnification of 80 000. The total amount of fibrils, fibril diameter distribution, and total fibril area were calculated.
Data Analysis
Data were analyzed for equal distribution using the Kolmogorov-Smirnov test. Because equal distribution testing failed, unpaired comparisons between the control groups and changes between the groups over time were performed using the Mann-Whitney test. Overall, differences between the study and the control groups were tested using Kruskal-Wallis analysis of variance. Failure modes during mechanical testing were compared using x2 analysis. The differences were considered to be significant at a probability level of P ≤ .05.
Results
Biomechanics
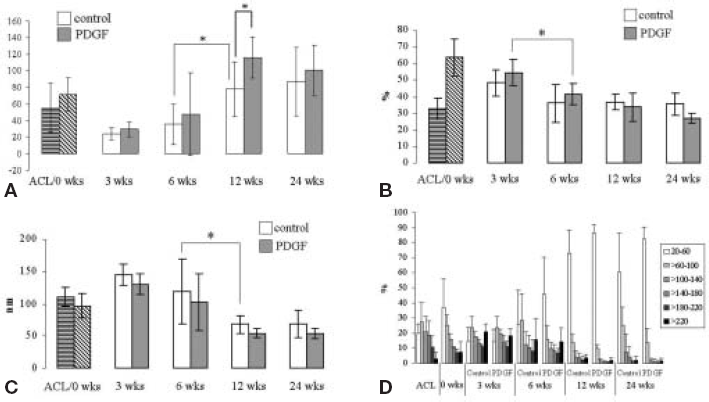
For AP displacement, there was no significant difference between the study and the control groups. Furthermore, there was no difference between the reconstruction at time zero and the intact ACL and the study and control groups over time (Figure 2A, Table 1).
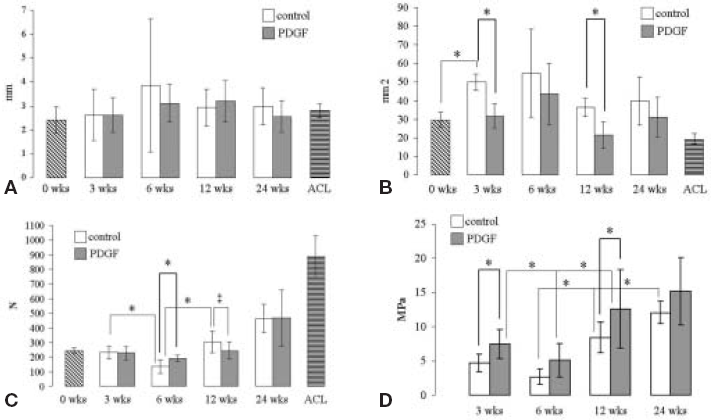
A, diagram showing anteroposterior displacement of the study and control groups, the intact ACL, and the reconstruction at time zero. Statistical analysis revealed no difference between the study and the control groups over time. B, diagram showing tissue cross-sectional area of the study and control groups, the intact ACL, and the reconstruction at time zero. C, diagram showing the failure load of the study and control groups, the intact ACL, and the reconstruction at time zero. The ‡ indicates trend toward significant difference (P = .065). D, diagram showing the tensile stress of the study and control groups. PDGF, platelet-derived growth factor. All data are given as mean ±SD. Asterisks indicate significant differences between 2 groups; statistcally significant differences were only indicated between the study and the control group or if there was a significant change between 2 time points.
Results for Biomechanical Testing (mean ± SD)
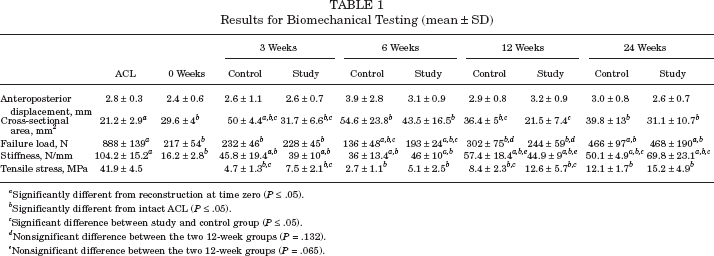
Significantly different from reconstruction at time zero (P ≤ .05).
Significantly different from intact ACL (P ≤ .05).
Significant difference between study and control group (P ≤ .05).
Nonsignificant difference between the two 12-week groups (P = .132).
Nonsignificant difference between the two 12-week groups (P = .065).
There was no significant difference for intraoperatively determined graft diameter between the study and the control groups. Cross-sectional area in the study groups was significantly lower at 3 weeks (P = .002) and 12 weeks (P = .002) as compared with the control groups. There was a significant increase of cross-sectional area between the graft tissue at time zero and the control group at 3 weeks (P = .002) (Figure 2B, Table 1). The cross-sectional area of the intact ACL was significantly lower compared with all groups, except the study group at 12 weeks.
Compared with the control group, stiffness in the study group was significantly higher at 24 weeks (P = .038) (Table 1). There was no significant difference at all other time points. Maximum load to failure was significantly higher in the study group at 6 weeks (P = .026). There was no significant difference at all other time points. At 6 weeks, the study and the control group showed a significantly lower failure load compared with the time zero reconstruction (P = .004 and P = .002, respectively). In the control group, there was a significant drop of failure load between 3 weeks and 6 weeks and a subsequent increase after 12 weeks, which was not found in the study group (Figure 2C, Table 1). The intact ACL showed a significantly higher failure load compared with all other groups.
The tensile stress in the study groups was significantly higher at 3 weeks (P = .004) and 12 weeks (P = .025) (Figure 2D, Table 1). At 6 weeks, we found a trend toward a higher stress in just the study group. There was a significant drop of stress in the study group between 3 and 6 weeks, followed by a significant increase at 12 weeks. In contrast, the control group showed a significant increase of stress between 6 and 12 weeks and between 12 and 24 weeks. In the study group, there was no further change between 12 and 24 weeks. The intact ACL showed a significantly higher tensile stress compared with all groups (Table 1).
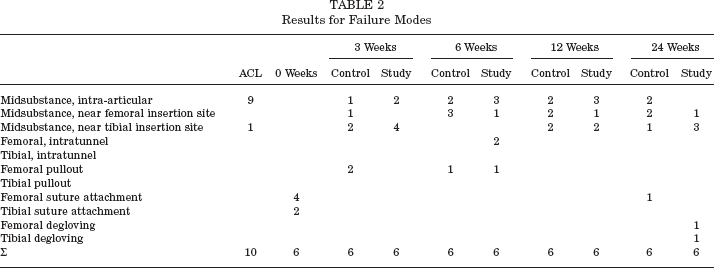
There was no significant difference for failure mode between the groups (Table 2).
Results for Failure Modes
Histologic Results and Vascularization
The intact ACL contained a significantly higher number of cells compared with the flexor tendon graft at time zero (Table 3). At 3 weeks, cell density in the control as well as in the study group increased significantly compared with the graft tissue at time zero. There were no significant differences between the study and control groups at all time points. At all measured time points, cell numbers in the study and the control group were significantly higher than in the flexor tendon graft and the intact ACL.
Results for Cell Density and Crimp Length Measurements
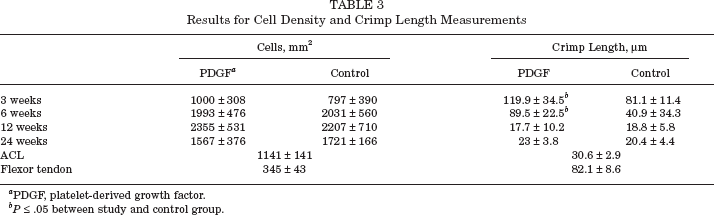
PDGF, platelet-derived growth factor.
P ≤ .05 between study and control group.
Crimp length measurements showed a significantly higher crimp length in the flexor tendon graft as compared to the intact ACL. At 3 weeks, crimp length in the study group as well as in the control group was not different compared with the flexor tendon graft but was significantly higher than in the intact ACL. At 6 weeks, there was a significant drop of crimp length in the control group, whereas the study group remained unchanged. Crimp length in the PDGF-treated grafts was significantly higher at 3 and 6 weeks compared with the control specimens (Table 3). In the study group, crimp length dropped significantly between 6 and 12 weeks. At 12 and 24 weeks, crimp length in the study groups and the control groups was lower compared to that of the ACL but not significantly different.
Vascular density of the intact ACL was significantly higher compared with the flexor tendon graft at time zero. At 3 weeks, the vascular status of the graft tissue in the study and the control groups remained unchanged compared with the graft tissue before implantation. At 6 weeks, there was a significant increase in vascularity in both groups, whereas in the study group vascular density was significantly higher in the central and subsynovial area as compared with the control (Figure 3). At 24 weeks, there was no significant difference between the graft tissue in both groups and the intact ACL.
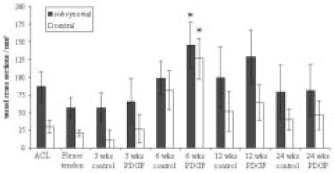
Diagram showing vessel density of the study and control groups, the intact ACL, and the flexor tendon graft at time zero. Data are given as mean ± SD. Asterisks indicate significant differences between the study and the control groups. PDGF, platelet-derived growth factor.
Transmission Electron Microscopy
The TEM data showed that the native ACL and the flexor tendon graft differ significantly in terms of percentage fibril area (P = .029). Between the study and the control groups, there was a significantly higher total fibril number in the study group at 12 weeks (P = .041) (Figure 4). There were no further differences for percentage of fibril area and mean fibril diameter. After 3 weeks, total fibril amount dropped significantly in the study as well as in the control group as compared with the graft tissue at time zero (P = .029 and P = .041, respectively). In the study group, there was a significant decrease of percentage fibril area between 3 and 6 weeks (Figure 4). In the control groups, there was a significant change between 6 and 12 weeks for total fibril amount and mean fibril diameter (P = .026 and P = .041, respectively). Analysis of collagen fibril diameter distribution showed a constant increase in small diameter fibrils in both the study and the control groups (Figure 4).
A, diagram showing total amount of collagen fibrils per μm2 in the study and the control groups, the intact ACL, and the flexor tendon graft measured by transmission electron microscopy (TEM). B, diagram showing the percentage of area covered by collagen fibrils in the study and control groups, the intact ACL, and the flexor tendon graft measured by TEM. C, diagram showing the mean collagen fibril diameter in the study and control groups, the intact ACL, and the flexor tendon graft measured by TEM. D, diagram showing the percentage of collagen fibril diameter distribution of the study and control groups, the intact ACL, and the flexor tendon graft measured by TEM. All data are given as mean ±SD. Asterisks indicate significant differences between 2 groups; statistcally significant differences were only indicated between the study and the control group or if there was a significant change between 2 time points.
Discussion
We have demonstrated that the local long-term application of PDGF-BB via a biodegradable drug delivery tool influences structural and mechanical properties during free tendon graft remodeling after ACL reconstruction. To our knowledge, this is the first study that has used a growth factor to accelerate graft tissue remodeling in an intra- articular setting using a large animal model.
The influence of various growth factors such as bFGF, TGF-B, EGF, insulin-like growth factor (IGF), and PDGF on wound healing has been extensively studied in the past.6,27,29,30,33,41,42 Their ability to promote fibroblast proliferation and migration as well as the production of extracellular matrix proteins offers the possibility to use these substances to accelerate healing of other soft tissues such as injured ligaments. 53
In recent years, different growth factors have been applied to enhance MCL healing.7,19,28,54 In these in vivo studies, different combinations and dosages of growth factors have been investigated, and PDGF isoform BB has been identified to be the most effective growth factor to enhance the quality of the healing MCL.19,27,28,54 Letson and Dahners 28 described an increase of failure load and stiffness up to 80% and 100%, respectively, in a rabbit model. These results encouraged us to use PDGF-BB to enhance ACL graft remodeling, although the healing MCL and an ACL substitute may display vastly different healing capabilities in terms of biological response and mechanical boundary conditions. Because MCL and ACL cells have different intrinsic properties regarding proliferation and migration,18,35 they also show vastly different responses to growth factors.4,15,25,26,31,44,47,57 These data may suggest that the differences in cellular properties explain why we have not seen such an intensive effect of PDGF on ACL graft remodeling as compared to its effect on MCL healing. However, because we used a free tendon graft in the present study, the principal differences between MCL and ACL fibroblast response to growth factors may be of minor importance. To explain this difference, Spindler et al reported that fibroblasts from patellar tendon origin have a better response to PDGF and TGF-B as compared with those from the ACL; thus, it might be suggested that a tendon graft is more likely to respond to the local application of a growth factor. 48
Although the MCL is embedded in good vascularized connective tissue, which is essential to provide the healing tissue with nutrients, a free tendon graft in ACL reconstruction stays in an intra-articular synovial environment and needs to be revascularized. In the present study, vascular density at 3 weeks was already comparable to the flexor tendon graft at time zero, which is in contrast to previous studies that have investigated ACL graft revascularization.5,14 Thus, there might be an early supply of nutrients at 3 weeks. At 6 weeks, we found significantly higher vascularity in the PDGF-treated grafts, which may indicate that PDGF treatment promotes revascularization of the graft tissue in the present model. Similar to our findings were the results of a study by Nakamura et al, which described an increased vascularity of a patellar ligament wound after PDGF gene transfer in rats. 36 Because it has been demonstrated that PDGF promotes proliferation of smooth muscle cells and endothelial cells, it is accepted that PDGF may also be involved in revascularization.8,36
To find the appropriate time point for the administration of growth factors to promote healing, investigators have shown that the level of endogenous growth factors is elevated by 3 to 7 days after ligament injury.26,37,40 Thus, delivery tools such as fibrin sealant or collagen emulsions have been proven to be effective in delivering the growth factors to the MCL injury site,7,19,28,54 although their delivery kinetics may be poor in terms of a long-term delivery (>72 hours). However, for an ACL injury model, a longer delivery of growth factors might be required because the biological response as well as the environmental conditions of the healing ACL are inferior compared with those of the MCL. 55 Kobayashi et al used polymer pellets to deliver bFGF to the injury site in a canine ACL-defect model. 21 They found that bFGF promotes defect filling between 1 and 24 weeks. However, short-term delivery vehicles have not been investigated for their effectiveness. Furthermore, the native ACL tissue has been studied by Kobayashi et al, not a free tendon graft as in the present study.
It has been thought that repopulated cells in the reconstructed ACL are of extrinsic origin. It is further believed that after revascularization and repopulation of fibroblasts into the grafted tissue, it takes a certain time period for the reconstructed ligament to remodel to the type of ligament that has similar characteristics of the native ACL. 3 Thus, distinct differences exist between the intrinsic healing of the injured ligament and that of the remodeling ACL graft, in which most cells are replaced by regenerative cells over time. To study this difference in terms of growth factor expression, Kuroda et al studied immunohistochemically the presence and the level of bFGF, TGF-B, PDGF-AA, and PDGF-BB expression in a model of ACL reconstruction in dogs using a free patellar tendon autograft. 22 They found that all tested growth factors were upregulated with a maximum expression at 3 weeks. They further described that compared to the graft tissue at time zero, the strongest increase in protein expression was found for PDGF, with up to 60% of all cells stained positive at 3 weeks. 22 This finding supports our hypothesis that PDGF should be viewed as one of the most effective growth factors during free tendon graft remodeling after ACL reconstruction.
The observations of Kuroda et al further imply that if a growth factor is administered to the free tendon graft, its tissue concentration should be highest around the third week to enhance the effect of the intrinsically present growth factors. To reach this goal, delivery vehicles other than collagen or fibrin sealant are required that will show a more protracted release. Moreover, it has been shown that PDGF undergoes a rapid clearance at the site of injury.11,43 The delivery tool used in the present study, a low molecular weight poly-a-hydroxyacid, has been shown to be effective in continuously delivering other growth factors such as IGF-1 and TGF-B over a period of 7 weeks, with a peak release around the third day. 46 This tool was further effective in enhancing fracture healing in rats. 45 However, the desired peak release of the growth factor to optimize ACL graft remodeling might be around the third week; therefore, the delivery vehicle used in the present study needs further improvement by means of an even more protracted delivery kinetic. As an alternative, other authors have thought to use gene transfer as a technology to overcome the limited-release kinetics of today's drug delivery vehicles.24,34,55
Although we administered approximately 60 μg of PDGF-BB to the graft tissue before implantation, we do not know how high the tissue level was during the following period of intra-articular remodeling. Thus, we do not know if the dosage we used was appropriate to maximally enhance graft remodeling in the present model. For the healing MCL, it has been described that there is a dose- dependant response to PDGF, reaching a plateau after a certain dosage. 7
During ACL graft remodeling, the tissue loses strength owing to reorganization of its extracellular matrix proteins, showing a maximum drop of its mechanical properties around the sixth to eighth week after implantation.10,17,20,51 In the present model, the grafts in the control group showed a significant drop of failure load between the third and the sixth week, followed by a significant increase of failure load at 12 weeks. In contrast, the PDGF-treated grafts did not show a significant drop of failure load between 3 and 6 weeks. Furthermore, there was a significantly higher failure load at 6 weeks compared with the control specimens (+42%), which may indicate that PDGF treatment improves structural properties in this vulnerable phase of free tendon graft remodeling.
An increase in tissue cross section, up to 185%, during cruciate ligament graft remodeling has been reported in the past. 20 The area increase was associated with a subsequent increase of tensile strength. 20 In the present study, the effect of PDGF treatment on the tissue's structural properties was mainly presented by a reduced cross-sectional area. Although the control grafts showed an increase of their cross sections at 3 and 6 weeks compared to the tissue at time zero, the PDGF-treated grafts remained almost unchanged. Consequently, the PDGF-treated grafts showed an improved tensile stress. This finding indicates an improvement of the structural properties of the graft tissue, which undergoes no compensative hypertrophy. In contrast, Chan et al (unpublished data, 1999) found a significantly increased tissue cross section after PDGF treatment of patellar tendon defects in rats. Nevertheless, we found a reduced cross section throughout the whole experiment, which shows that this effect was constantly present. There was no further increase of tensile stress in the study group between 12 and 24 weeks, whereas the control specimen still showed a significant improvement. This finding suggests that the PDGF treatment in the present study led to an early termination of remodeling.
With respect to the collagen structure of the free tendon graft tissue, we found that the local application of PDGF increased crimp length at 3 and 6 weeks as compared with the control tissue. Other authors have observed that the natural drop in crimp length, as a sign of functional adaptation, is associated with the maximum loss of mechanical properties.3,51,52 In the PDGF-treated animals, crimp length at 6 weeks remained unchanged compared with the graft tissue at time zero, whereas the control group showed a significant drop. At that time, the tensile strength was significantly higher in the PDGF-treated specimens. However, it remains unclear how crimp length affects tensile strength and how PDGF influences this parameter.
The TEM analysis showed that at 12 weeks, the total collagen fibril number was significantly higher with PDGF treatment. Thus, we suggest that PDGF treatment of a free tendon graft changes mechanical properties of the tissue by influencing collagen fibril structure, although other parameters, such as percentage of fibril area and mean fibril diameter, showed no significant difference between the study and the control groups. However, because TEM data show only a limited area of the whole remodeling ligament, and the fact that vastly different zones can be found in the graft, especially during early healing, 51 TEM data should be interpreted with caution. The general observation that collagen fibril diameter shows a shift toward smaller fibrils is in line with previous reports. 9
In the past, most studies investigating ligament healing or graft remodeling described inferior structural properties, such as a reduced tensile strength or an increased cross-sectional area, compared with the uninjured native tissue. This observation has a tremendous clinical consequence for the functional restitution of injured knee joints. Therefore, there is a strong need to improve structural properties of healing or remodeling ligament tissue. The use of growth factors solely or in combination may thus present a promising tool toward the complete structural and mechanical restitution of healing soft tissue. We have demonstrated that the local application of PDGF to a free tendon graft is effective in changing certain structural and mechanical properties, although the tissue was in an avascular and intra-articular environment. If this effect can further be improved by, for example, refining the drug delivery tool, finding the most effective dosage, or combining different growth factors, it should encourage further research.