
Abstract
Objective: To educate sports medicine practitioners as to length of time for an athlete to return to activity after sustaining a rupture of the plantar fascia.
Methods: Athletic patients sustaining plantar fascia ruptures and subsequent treatment were reviewed. Diagnosis was based on clinical findings, although radiographic studies were done. Patients were treated for 2 to 3 weeks with a below-knee or high- top boot, nonweightbearing, with an additional 2 to 3 weeks of weightbearing in the boot. Patients used physical therapy.
Results: Eighteen athletes, including 6 elite athletes, were evaluated. Mean age was 40.9 ± 13.2 years. There were 12 males and 6 females. Mean postinjury follow-up was 42 months. Duration of prior plantar fascia symptoms ranged from 0 to 52 weeks. All but 2 ruptures were of the medial portion. Four patients had injections prior to rupture. Five patients wore orthoses preinjury; 14 wore orthoses postinjury. All patients returned to activity after 2 to 26 weeks (mean, 9.1 ± 6.0 weeks). Running athletes predominantly composed the cohort; others played tennis, volleyball, and basketball.
Conclusion: Using the treatment protocol, patients sustaining plantar fascia rupture can achieve favorable results with complete return to activity. None of the 18 patients sustained reinjury, had postinjury sequelae, or necessitated surgery, contrary to other studies.
The plantar fascia is one of the most important supporting structures to maintain the integrity of the plantar arch of the foot. Plantar fasciitis is a well-acknowledged condition in athletes, particularly runners. Rupture of the fascia may occur spontaneously during athletic activity.1,3 It is not a commonly reported injury.
Plantar fascia rupture was first described by Leach et al in 1978.3,4 It is often described by the patient as an intense tearing sensation on the bottom of the foot. Patients may have prior symptoms of plantar fasciitis.1,3,5 Previous reports of this injury have focused on the association of prior corticosteroid injection to treat plantar fasciitis, a common athletic condition.1,2,5 The purpose of this study is to focus on the diagnosis and treatment of plantar fascia rupture in the athlete. Using the clinical symptoms exhibited by athletes who have sustained acute injury to the plantar fascia and a systematic treatment protocol, we propose that favorable results can be obtained. Not only is a history of prior plantar fasciitis and possible steroid injection important, but also the acute onset of symptoms during athletic activity is important in making the diagnosis. Evaluation of the length of time to return to the desired athletic activity will be documented to help guide sports medicine practitioners.
Methods
From 1990 to 2000, patients treated for plantar fascia ruptures associated with athletic activity were retrospectively evaluated by the authors. In addition to chart review, these patients were seen by their original treating providers for their evaluations. A minimum of 2 years postinjury follow-up was required for inclusion. Eighteen athletic patients, including 6 elite athletes, treated for plantar fascia ruptures fulfilled the inclusion criteria. (Elite athletes were defined as those who had made an Olympic or national team.) Twelve males and 6 females were evaluated. The mean age was 40.9 ± 13.2 years.
Diagnosis was based on clinical findings, including the following: patients felt a “pop” in the proximal plantar heel region of their feet during activity, inability to perform a single-stance heel raise, plantar ecchymosis (Figure 1), and pain with passive extension of the digits. Radiographs may have included finding of an avulsion of a plantar calcaneal tubercle (Figure 2). For all cases, the diagnosis was based on clinical findings. However, MRI was obtained in 5 cases (4 elite athletes), for additional documentation and verification (Figure 3). MRI showed partial plantar fascia rupture in the medial portion in all of these cases. All patients did have x-ray evaluation; however, due to the acute injury, most of the images were nonweightbearing views. Therefore, quantitative documentation (using weightbearing lateral radiographs) of foot type was not performed as in Acevedo and Beskin's study. 1

Plantar ecchymosis associated with rupture of the fascia.
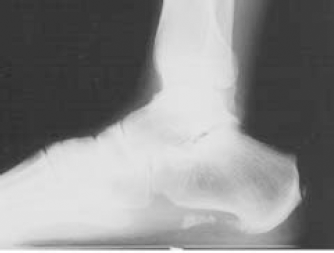
Avulsion of the plantar tubercle in a patient with a history of 5 corticosteroid injections. He sustained a lateral band tear.
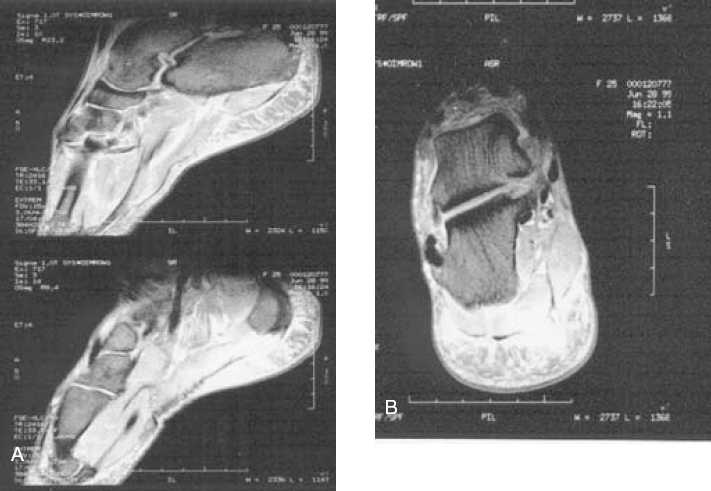
A, MRI lateral image depicting plantar fascia rupture. B, axial MRI image showing medial band rupture in the same patient.
The following data were retrospectively reviewed and recorded for each patient: date of injury; sport/activity; return to activity [RTA] (sport), which is defined as the first practice session in the desired activity; and return to competition for elite athletes. Additional data documented included age, sex, location, use of foot orthoses both preinjury and postinjury, injection prior to injury, length of symptoms prior to rupture, type of immobilization device if used, and if surgery or reinjury occurred during the follow-up period. Statistical significance was set at P < .05. Student t, Spearman correlation coefficient, and Wilcoxon tests were applied where appropriate, using the Systat Statistical Program (Cary, NC).
The authors’ preferred treatment protocol consisted of 2 to 3 weeks of nonweightbearing in a high-top or short-leg removable cast-boot. Protected weightbearing in the boot, as tolerated, followed when there was no pain at rest or with passive extension of the digits, for another 1- to 3-week period. When there was no pain with ambulating for 1 week, the boot was discontinued. Physical therapy commenced 7 to 28 days postinjury and consisted of electrical stimulation, pulsed ultrasound, ice, manual deep tissue massage, and gentle stretching as tolerated. An evaluation was included to assess any need for foot orthoses, and the appropriate recommendations were then made. Foot orthoses were generally thermoplastic, semiflexible polypropylene, with the prescription based on the patient's neutral subtalar position.
Returns to activity was guided by the patients’ symptoms; 30 minutes of stationary cycling or running in the pool without discomfort was a typical guideline to ascertain whether additional sports could be tolerated. Runners usually initiated their RTAs with a 20-minute run. The providers, who queried the patients as to when they started their sports, recorded the RTA time frame.
Results
Mean postinjury follow-up for the 18 athletes was 42 months with a range of 24 months to 10 years. Average return to athletic activity was 9.2 ± 6.2 weeks with a range of 2 to 26 weeks. Elite athletes returned to competition after 7 to 40 weeks. One elite athlete retired at the time of data collection for other reasons but qualified for 2 Olympic teams subsequent to his injury. The 17 other athletes continue to participate in their sports. None of the athletes were noted to have any postrupture unilateral arch collapse of their feet, although there remained some asymmetry as to the contour of the plantar fascia.
There were 16 medial plantar fascial tears and 2 lateral tears. One of the athletes with a lateral tear had a previous plantar fasciotomy from a medial approach. Five athletes wore foot orthoses preinjury, and 14 athletes used them postinjury. There were 12 athletes who were injured while running, including 2 triathletes. Other activities inciting rupture included hiking, basketball, tennis, and soccer. All but 1 patient experienced prior plantar fasciitis. Only 1 patient, a jogger, was currently under treatment by the authors, and she received a corticosteroid injection 2 days prior to her injury, which resulted from jumping out of the way of a rattlesnake while hiking. Four of the 18 received a prior injection of corticosteroid (ranging from 1 to 5 injections). None of these patients had been placed on restriction of activity or were immobilized postinjection, other than our patient who was told not to run for 1 week. The preinjury symptoms of all patients ranged in duration from 0 to 52 weeks.
Statistical analysis was performed to compare RTA of elite athletes (5.0 ± 3.6 weeks) with RTA of nonelite athletes (11.2 ± 6.0 weeks), which yielded P = .03. Spearman correlation coefficients were used to indicate if age was correlated with statistically significant longer RTA, which was true, P < .05. No other variables such as gender, duration of prior symptoms, prior injection, or use of a below-knee boot (vs no boot) yielded any statistical difference when comparing RTAs. In fact, 2 patients refused a boot, and although their clinical symptoms matched the others, they appeared to have sustained less severe injury. The RTA difference between those who used a below-knee boot versus those who used no boot was 9.8 weeks and 8.6 weeks, respectively (P = .32, 1-sided Wilcoxon). The RTA difference between those patients having an MRI study (7.8 ± 5.9 weeks) versus those who did not (9.6 ± 6.2 weeks) was not statistically significant (P = .58). Four of 5 of these patients undergoing MRI were elite athletes who, as noted above, had a faster RTA.
Discussion
Plantar fasciitis is one of the most common injuries in the athletic population. Treatment of patients with plantar fasciitis frequently involves local corticosteroid injection. The mechanism of acute injury to the plantar fascia may be due to an excessive overload on the weakened structure. Rupture could represent an acute-on-chronic injury as well, particularly in runners. Corticosteroid injection may accelerate the weakening effect on the plantar fascia. There has been shown to be an association in previous reports between rupture of the plantar fascia and steroid injection.1,3,5
Leach et al reported that in 6 ruptures of the plantar fascia, 5 had previously undergone injection. 3 Sellman reported on 37 patients with ruptures, which were all associated with previous injection. 5 Acevedo and Beskin reported on 51 ruptures, with 44 cases having undergone injection therapy, and stated they had a 10% rate of rupture with their injections. 1 They injected 1 mL of triamcinolone acetate (40 mg/mL) from a medial approach deep into the plantar fascia. Four of the 18 patients in our study had prior injection of the corticosteroid in plantar fascia for fasciitis. Patients, particularly athletes, should be warned of the possible adverse effect of plantar fascial rupture associated with corticosteroid injection of the plantar fascia.
RTA was similar in our 18 patients as compared to the findings of Leach et al, 3 who reported full RTA within 3 months of all 6 athletic patients. Sellman along with Acevedo and Beskin reported a 50% rate of long-term pain status postinjury.1,5 They found that the original heel symptoms were resolved, but subsequent pain was found in other areas of the feet as sequelae of the rupture, which damaged the integrity of the arch.
Acevedo and Beskin reported the use of orthoses in 22 of 40 long-term follow-up patients. 1 Perhaps our greater use of postinjury foot orthoses (14 out of 18 patients) along with our treatment protocol have contributed to the lack of sequelae in our patient population. A larger study could validate this statistically. The fact that 2 patients in our study returned to their activities slightly faster than those immobilized in a boot was likely due to their own self-treatment of limiting ambulation and possibly sustaining a less severe injury to the plantar fascia. The other articles reviewed showed variable treatment for plantar fascia ruptures.
Leach et al provided the most detailed description of any other author's treatment protocol. 3 Treatment for acute pain included crutches as long as there was pain, ice for 15 minutes 3 times per day for 8 to 15 days, and phenylbutazone 100 mgs 3 times a day for 6 to 8 days. Once the acute pain had subsided, the foot was taped with felt padding, with gradual return to weightbearing 2 to 3 weeks postinjury. Athletes were allowed to return to running and/or jumping when they could stand on tiptoes without pain. The patients of Leach et al were athletes and did not have MR imaging to confirm the diagnosis.
Acevedo and Beskin stated that all their patients received a trial of a nonsteroidal anti-inflammatory drug and/or a mild narcotic analgesic, as well as having rest and activity modifications. 1 If the patients had “a lot” of pain, then either a stiff-soled sneaker with an orthotic (no mention of custom or over the counter) or a boot walker was used until pain subsided. Sellman only mentioned the use of a boot walker in his treatment protocol but failed to mention the length of immobilization. 5
The major weakness of our study is that it was not prospective, randomized, and double blind. Often in clinical practice and certainly when dealing with elite athletes, this type of study is not realistic. Elite athletes want to “push the envelope” and often want to return to their sports as soon as possible. This produced variability in the treatment regimen, and furthermore, some patients refused immobilization and orthoses. The immobilization period was often shorter for elite athletes because they often felt asymptomatic sooner. This may be due to immediate access to medical care, diagnostics such as MRI, and rehabilitative modalities. There may have been bias in recording the RTA time frame as well because the patients were often given permission to begin their sports only after seeing the doctor at a specific time interval. We are unable to explain why 2 of our patients, despite lack of immobilization and protective support, had good results as well, other than the possibility that they had a less severe rupture; self-treatment of rest is also beneficial.
Future studies could evaluate the benefit of modalities applied sooner versus later. Also, MRI evaluation to assess the severity and degree of rupture may be beneficial. Perhaps total rupture may have prolonged recovery and sequelae. Accurate assessment of foot type and possible postrupture change in morphology could be performed as well.
Conclusion
A postinjury protocol including the use of a cast-boot, a period of nonweightbearing, physical therapy, and appropriate use of foot orthoses can lead to complete recovery from rupture of the plantar fascia. One should expect to return to athletic activity after 9 weeks following this injury. Follow-up of a minimum of 2 years shows good results with this treatment protocol, with no sequelae post-plantar fascial rupture.