
Abstract
Background: Optical coherence tomography is an echograph of infrared light that can yield microscopic cross-sectional images of articular cartilage without removing or damaging the tissue.
Hypothesis: To determine whether optical coherence tomography images of human cartilage can be acquired arthroscopically and whether the resulting images have high correlation with histopathology.
Methods: Optical coherence tomography was configured into an arthroscope and used to image 2 human cadaver knees and 45 cores harvested from 9 osteoarthritic knees. The imaged cartilage was then processed for histological analysis. Optical coherence tomography images and histology were graded using a modified Mankin structural score. Agreement was determined using weighted kappa statistics. Morphometric analysis performed on optical coherence tomography images was correlated with histomorphometric analysis using linear regression.
Results: Imaging of the medial and lateral femoral condyles and trochlea was readily accomplished using the optical coherence tomography arthroscope. Modified Mankin surface scores for specimens with the earliest structural changes (grades 0-3) had high agreement with scores assigned to histology ([.kappa] = 0.87). Fibrillation indices calculated from optical coherence tomography had near-perfect correlation to that of histology (R = 0.98)
Clinical Relevance: Arthroscopic optical coherence tomography may be clinically useful for early detection of articular cartilage injury and nondestructive assessment of articular cartilage repair.
Keywords
Articular cartilage damage frequently accompanies sports and activity-related injuries. 7 Although patients may experience pain and dysfunction resulting directly from acute cartilage injury, many more will eventually suffer from degenerative arthritis.6,17 Early signs of cartilage degeneration do not affect the full thickness of the tissue and may include blistering, fibrillation, and flaps. Debridement is commonly used in an attempt to slow progression of these lesions. 24 In addition, advances in cell-based therapy, cartilage transplantation, and tissue engineering have increased potential treatment options for focal chondral defects.2,4,10,28 As new treatments arise, there is an increased need for improved accuracy in grading and assessing damaged articular cartilage to measure treatment effects and to develop appropriate treatment algorithms. 19 For these reasons, new technology for early detection of articular cartilage damage has high clinical relevance.
Optical coherence tomography (OCT) is an echograph of near-infrared light that can yield cross-sectional images of a variety of tissues at a high spatial resolution (4-20 μ) comparable to histology and in near-real time without damaging the tissue.13,14,27 The technology is described as being analogous to ultrasound except that the image is generated from measuring the back reflection of near-infrared light instead of sound waves. In addition, OCT is a fiber optics-based imaging technique that can be easily integrated with conventional arthroscopy for in vivo diagnosis. For these reasons, the OCT image has been described as a noninvasive “optical biopsy.” 9
Applying OCT to articular surfaces, we recently assessed articular repair tissues in a rabbit model and determined that the OCT images had a high correlation with histology. 12 Unlike histology, which necessitates removal of tissue from the body, the OCT “biopsy” was obtained in situ and close to real time with no damage to the cartilage. These results raised the possibility of assessing articular cartilage using arthroscopic OCT (AOCT). We subsequently developed a handheld AOCT probe and used it to image articular cartilage arthroscopically within intact porcine knee joints. 26 Using this novel arthroscope, we were able to obtain cross-sectional images of porcine articular cartilage before and after arthroscopic wounding using surgical instruments. This study was conducted to determine the utility of the OCT arthroscope in arthroscopic examination of human articular cartilage and to test the hypothesis that images of human articular cartilage obtained using a handheld OCT arthroscope correlate with histopathology.
Materials and Methods
Arthroscopic Optical Coherence Tomography System
The AOCT system consists of a fiber-optic OCT setup connected to a handheld probe optimized for insertion into human joints. The principles of OCT and the technical details of our real time OCT setup have been previously reported.25,27 A schematic of the optical layout within the probe and a photograph of the handheld AOCT probe are depicted in Figures 1A and 1B. A self-focusing mechanism was built into the probe, enabling a surgeon to obtain a high-resolution cross-sectional image by touching the surface of the cartilage. By sealing the probe tip with an angled glass window, we increased the focal length of the scan lens to either 40 or 60 mm, depending on the focal length of the scan lens used. This length was further increased to 70 or 110 mm by inserting the custom scan lens in the middle of the tube, thus enabling the focal length to be of a sufficient magnification for intra-articular examination of most human joints (Figure 1C). Sealing the probe tip also protected the optical components from fluid contamination during arthroscopic examination and substantially improved the signal-to-noise ratio by minimizing specular back reflection and water absorption at a 1300-nm wavelength range. A computer with Pentium IV processing capability displayed and stored the 2-dimensional OCT image sequences acquired during the arthroscopic examination.
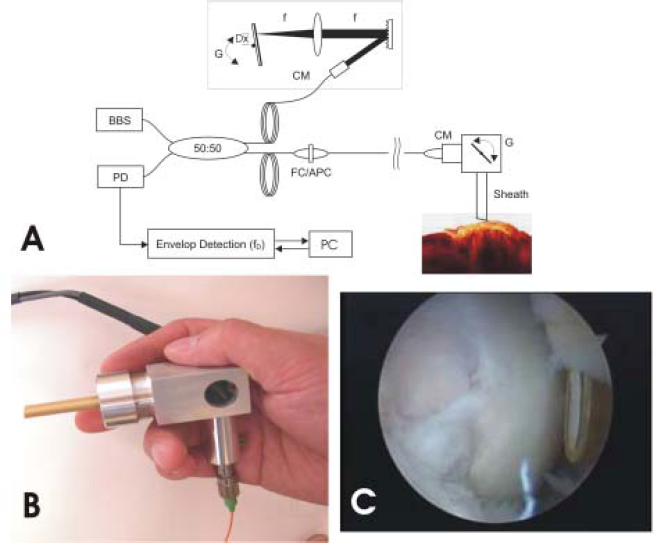
Arthroscopic optical coherence tomography (AOCT) system. A, a schematic diagram of the OCT setup with AOCT probe; B, a photograph of the handheld AOCT probe; C, the AOCT probe inserted into a human knee joint. The angled glass window sealing the probe tip can be seen
Arthroscopic Assessment
To determine whether usable optical biopsies of articular cartilage could be obtained arthroscopically using the AOCT, we performed arthroscopic assessment of cadaver knees. The use of donated human cadaver knees for AOCT was approved by the University of Pittsburgh Committee for Oversight of Research Involving the Newly Dead. Two human cadaver knees—a right knee and a left knee from different donors—were mounted onto a modified vise grip. Standard size anterolateral, anteromedial, and transpatellar portals were made. A conventional surface imaging arthroscope (Dyonics, Smith and Nephew Richards, Memphis, Tenn) was first placed into the anterolateral portal. By conventional arthroscopic surface imaging and probing methods, neither knee appeared to have areas with identifiable articular cartilage damage. Next, OCT optical biopsies of the medial femoral condyle were obtained using the AOCT. Repositioning of the OCT arthroscope into the anterolateral and transpatellar portals enabled OCT imaging of the lateral femoral condyle and trochlea, respectively. To facilitate histological correlation, an area in the medial femoral condyle to be scanned was therefore designated using an 8-mm osteochondral coring device (Figure 2A). The OCT probe was then inserted into the knee joint via the medial portal to scan the pre-marked area (Figure 2B). Cores were harvested by arthrotomy and prepared for cross-sectional analysis.
Arthroscopic optical coherence tomography (AOCT) system. A, the designated area for assessment was precored using a standard osteochondral coring device. This area was assigned grade 0 chondromalacia based on arthroscopic surface and tactile assessment. B, the AOCT probe was inserted into the joint and placed on the cartilage. The probe has a self-focusing mechanism that allowed the surgeon to obtain a nondestructive optical biopsy. C, the AOCT optical biopsy revealed fine surface fibrillations. D, removal of the core followed by histological analysis confirmed that the articular surface was not intact
Ex Vivo Assessment
To image human tissues with a broader spectrum of pathology, the in situ arthroscopic assessment was complemented with ex vivo assessment using the AOCT probe. A total of 45 cores from 9 osteoarthritic human tibial plateaus excised at total knee replacement were obtained through an exempt protocol approved by the Institutional Review Board of the University of Pittsburgh. The plateau was excised and immediately placed in physiological saline (Hank's Balanced Salt Solution/Gibco, Invitrogen, Carlsbad, Calif) for transport from the operating room to the laboratory. The tissue was refrigerated until use. Within 8 hours after surgery, the plateaus were examined using conventional arthroscopic surface imaging (Dyonics Arthroscope, Smith and Nephew Richards) to identify areas appearing to have intact surfaces (chondromalacia grade 0/1), areas with fine fibrillations (chondromalacia grade 2), and areas with deep clefts (chondromalacia grade 3). Probe palpation was not performed. Areas appearing to have exposed bone (chondromalacia grade 4) were avoided. This grading system represents a common clinical modification of the Outerbridge classification for chondromalacia patellae. 23 Full-thickness cylindrical osteochondral plugs were harvested from the previously identified areas of each plateau using an 8-mm-diameter osteochondral coring device (Mitek, Norwood, Mass). The osteochondral samples were removed from the coring device by tapping on the bone side of the coring sleeve to avoid damage to the articular surface. During the coring procedure, the cartilage was kept moist with physiological saline. Osteochondral cores were then sectioned in the midsagittal plane using a bone cutter. One half was placed into physiological saline to be scanned by the AOCT and processed for histological analysis. The other half was prepared for fluorescent viability staining.
Optical Coherence Tomography
The OCT arthroscope was mounted on a custom jig (a 3-dimensional motored stage) allowing for adjustments in the x-y planes. Hemicores for OCT scanning were placed in a flat-bottom tissue culture plate (Falcon by Becton Dickinson, BD Biosciences, San Jose, Calif). The samples were set in soft silicone or vacuum grease to position the cartilage surface perpendicular to the mounted OCT arthroscope. Physiological saline was added until the surface of the sample was submerged. The path of the scan was monitored using a red aiming laser. The cartilage was positioned so that the near-infrared beam scanned parallel to the cut edge of each hemicore. Six scans were taken per sample, beginning at the cut edge and radiating back into the tissue. Initial scans were kept as close to the cut edge as possible to facilitate correlation with the red/green staining and histology.
Histology
After scanning with OCT, the hemicores were placed in a 12-well flat-bottom tissue culture plate (Falcon by Becton Dickinson, BD Biosciences) and fixed in 10% formalin (Fisher, Pittsburgh, Penn) for histological processing and staining. Formalin-fixed sections were decalcified, dehydrated, and processed using an automatic processor (Tissue-tek, Sakura, Torrance, Calif). The samples were then embedded in paraffin and sectioned into 7-μm slices. Twenty serial sections were obtained from each specimen. Two sections were placed on each slide. Alternate slides were stained with either hematoxylin and eosin or safranin O and fast green (Fisher). The sections were analyzed using a microscope equipped with a digital-imaging system (Nikon, Tokyo, Japan).
Fresh Cross Sections
Three 1-mm-thick samples were taken from the flat cut edge of the opposing hemicore using a number 22 scalpel blade and a dissection microscope for accuracy. The slices were then placed in a 24-well flat-bottom tissue culture plate (Falcon by Becton Dickinson, BD Biosciences), 1 slice per well. These slices were covered by a solution of minimal media (Dulbecco's Modified Eagle Medium, BD Biosciences) containing 1% penicillin/streptomycin (BD Biosciences) and 10% fetal bovine serum (BD Biosciences) to be used in fluorescent viability staining. 3 The green fluorescing stain, 5-chloromethylfluorescein diacetate, is a membrane-permeant fluorescein-based product that is cleaved by active enzymes present in healthy cells and is therefore used to identify viable cells. Propidium iodide, a red fluorescing nucleic acid stain, is excluded by healthy cell membranes and is used to identify unhealthy cells. The 1-mm sections were incubated in phosphate-buffered saline (PBS) (Sigma, St. Louis, Mo) containing 5-chloromethylfluorescein diacetate and propidium iodide (both from Molecular Probes, Eugene, Ore) for 30 minutes. The samples were then washed twice with PBS. The washed samples were fixed in 1 mL of 2% paraformaldehyde (Sigma) for 1 hour at room temperature. Finally, the samples were again washed twice with PBS and then stored at 4°C in 1 mL of fresh PBS until they could be imaged using a fluorescent microscope equipped with epiflourescence and a digital-imaging system (Nikon).
Comparison of OCT with Histology
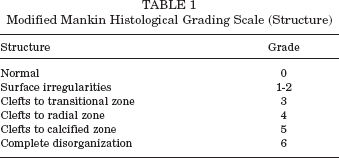
The cross-sectional images were graded according to a modified Mankin histological scoring system for articular cartilage. 20 This scoring system is a recognized standard for comparing different histological grades of articular cartilage degeneration. There are 4 general categories by which the score is computed. Subscores are assigned for the categories of structure, cells, safranin O staining, and tidemark integrity. Because the OCT images provided primarily structural information to a depth of 1.0 to 1.5 mm, only the structural category was used in this study. The Mankin structural category was further modified to combine grade 1 (surface irregularities) with grade 2 (pannus and surface irregularities), because none of the specimens had evidence of pannus. The modified grading scale is summarized in Table 1.
Modified Mankin Histological Grading Scale (Structure)
Modified Mankin structure grades were first assigned to each specimen based on evaluation of the OCT images by an orthopaedic surgeon (CRC). Using the same criteria, grades were independently assigned to histopathology by a pathologist (CTC) blinded to the OCT results.
Weighted kappa statistics were calculated to determine the degree of agreement between the OCT-assigned grades and the grades assigned using histology. A weighted kappa value of less than 0.00 indicated poor agreement, a value of 0.00 to 0.20 indicated slight agreement, a value of 0.21 to 0.40 indicated fair agreement, a value of 0.41 to 0.60 indicated moderate agreement, a value of 0.61 to 0.80 indicated substantial agreement, a value of 0.81 to less than 1.00 indicated almost perfect agreement, and a value of 1.00 indicated perfect agreement. 29
Image Analysis
The OCT images were compared with fluorescent-stained cross-sectional images and with histological sections. Images from OCT and from histologic sections were analyzed using custom image analysis software. The specific parameter of interest was quantification of articular surface topography. Root mean square is a statistical measure of the magnitude of a varying quantity. It has been used in histomorphometric measurements of regenerating cartilage to quantify the degree of repair tissue deviation from an idealized original surface.5,11 When assessing damaged and degenerating cartilage, however, determining where the idealized original surface should be is frequently not possible. We therefore defined the fibrillation index (FI) to be the root mean square of the deviation of the cartilage surface profile from an idealized smooth surface following an ideal debridement. For this application, Fn represents the measured deviation in microns of the actual surface from a line drawn to simulate creation of a smooth surface through an ideal debridement (Figure 3). Measurements were taken at 50-μm intervals. The FI or root mean square smoothness was then determined by the following equation: FI = 1/N (S Fn2)1/2. Results from OCT images were correlated with those of the corresponding histology using linear regression.
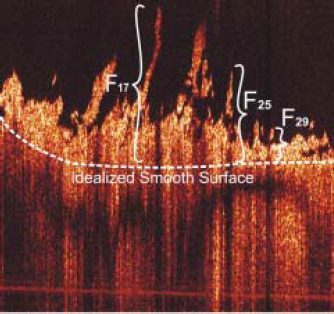
The fibrillation index (FI) is a measure of surface topography. We defined FI as the root mean square of the deviation of the cartilage surface profile from an idealized smooth surface following an ideal debridement. For this application, Fn represents the measured deviation in microns of the actual surface from an idealized smooth surface following an ideal debridement. Three of the 34 measurements used to calculate the index for this particular image are depicted.
Results
Arthroscopic Optical Coherence Tomography Assessment
AOCT imaging of the weightbearing regions of the medial and lateral femoral condyles and of the central trochlea was readily accomplished using the OCT arthroscope. The self-focusing mechanism allowed the surgeon to easily obtain focused images by touching the tip of the scope to the articular surface (Figure 2B). Varying the flexion angle of the knee allowed for ready coverage of a 24 × 12-mm area of each condyle and an 18 × 12-mm area of the central trochlea. It was not possible to image the tibial plateaus using this OCT probe through standard portals.
Comparison to Surface Imaging
The OCT arthroscope provided near-immediate assessment of the surface and subsurface characteristics of the articular cartilage. OCT imaging revealed that cartilage appearing normal using surface imaging techniques frequently had surface and subsurface abnormalities. When compared to histopathology, surface imaging frequently underestimated the degree of damage, whereas OCT detected fine surface fibrillations that were confirmed by histology (Figures 2 and 4). Fine fibrillations as well as isolated gaps were also revealed by OCT and histology in cartilage that had been classified by surface imaging to have an intact surface (Figure 4). Only 2 out of 15 cores deemed to have intact surfaces based on surface imaging alone had intact surfaces by histological assessment. OCT identified the remaining 13 as having superficial fibrillations consistent with histopathology. In addition, subsurface damage undetectable by surface imaging was readily detectable by OCT.
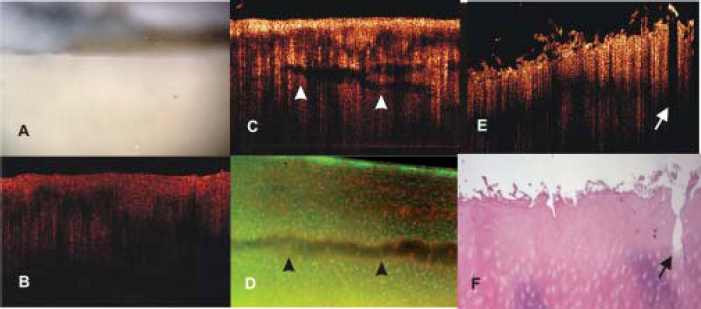
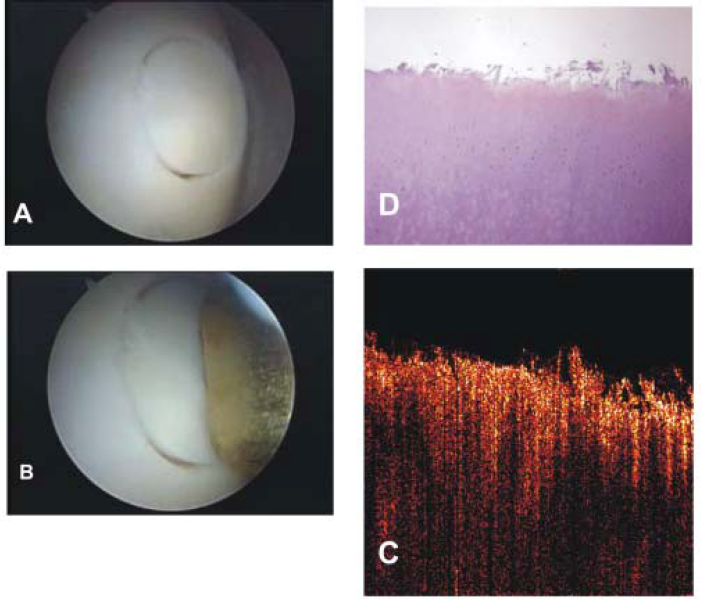
Chondromalacia grade 0/1 (intact surface). The high axial resolution of optical coherence tomography (OCT) reveals surface and subsurface abnormalities to articular cartilage that are not apparent with conventional surface imaging. A, a specimen assigned grade 0/1 by surface imaging. B, the same specimen viewed by OCT reveals an intact surface. C, OCT image of a second specimen also assigned grade 0/1. Note the subsurface defects (white arrowheads) not apparent to surface imaging. D, the subsurface defects are confirmed by the fresh cross section of the same specimen. E, a third specimen graded 0/1 by surface imaging. The OCT image shows fine fibrillations of less than 1 mm along with a partial-thickness tissue cleft (white arrow). F, the corresponding histological section for this specimen confirms the presence of the gap and the fine surface fibrillations
Fine surface fissuring could be differentiated from deeper clefts using OCT (Figure 5). For cartilage identified by surface imaging to have deep fissures, OCT was consistent with deep clefting, and histopathology confirmed fissuring to subchondral bone in nearly all cases (Figure 6).
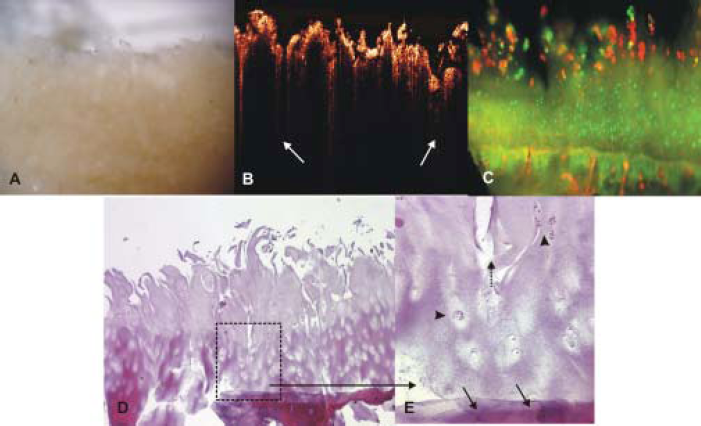
Chondromalacia grade 2 (superficial fibrillation). A, by surface imaging, this specimen was judged to be grade 2 chondromalacia; B, the optical coherence tomography image revealed deeper clefts (white arrows); C, the corresponding fresh cross section also seemed to show near full-thickness involvement; D, histology confirmed deep clefts; E, detail of the boxed area reveals deep chondrocyte clones (arrowheads) and clefting (dashed arrow) nearly down to subchondral bone (arrows).
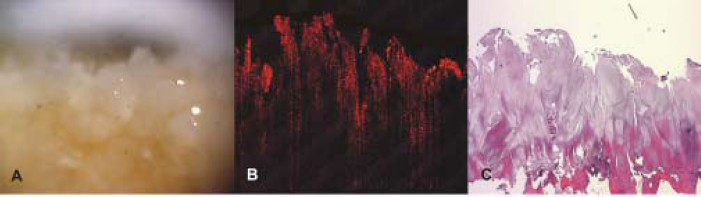
Chondromalacia grade 3 (deep clefts). A, for cartilage identified by surface imaging to have deep fissures; B, optical coherence tomography was consistent with deep clefting; C, histopathology confirmed fissuring to subchondral bone.
Comparison to Microscopic Cross-Sectional Analysis
Images obtained with the OCT arthroscope both arthroscopically and ex vivo were comparable to histology. Structural details seen at the microscopic level correlated well with OCT optical biopsies of articular cartilage.
Fibrillation detail was seen better in the OCT image than in the fresh cross sections stained with fluorescent viability stains (Figure 5). On viability staining, chondrocytes within the more fibrillated areas of cartilage had reduced evidence of viability when compared with chondrocytes in the deeper layers. Cell morphology and cell viability were not discernible through OCT imaging.
Modified Mankin surface scores assigned to the 45 tibial plateau specimens based on OCT images revealed good agreement with scores assigned to the corresponding histology (κ = 0.80). Substantial agreement between OCT and histopathology was seen for specimens assigned grades 0 to 3 (κ = 0.87). The distribution of Mankin structural scores for the 45 cores is summarized in Table 2.
Modified Mankin Structural Score Distribution a
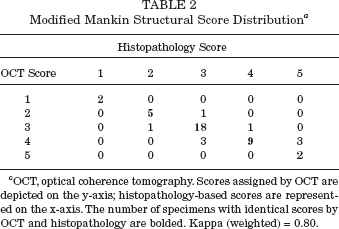
OCT, optical coherence tomography. Scores assigned by OCT are depicted on the y-axis; histopathology-based scores are represented on the x-axis. The number of specimens with identical scores by OCT and histopathology are bolded. Kappa (weighted) = 0.80.
The cross-sectional nature of the OCT images enabled in situ measurements of the depths of fibrillation for partial-thickness fissuring. Comparative histomorphometric analysis was performed on the 6 specimens in which histology definitively matched OCT. For the remaining 39 specimens, the images were qualitatively similar. However, they lacked specific identifying features such as an odd-shaped gap or fibrillation in the same location and orientation for both histology and OCT to permit accurate quantitative comparison.
Measurements taken from OCT images had good correlation with histomorphometric analysis of the corresponding histological sections (Figure 7). Measurements of Fn on OCT images differed at times from histomorphometry despite apparent excellent qualitative correlation between OCT and histopathology. This discrepancy may be attributed to a slight flattening of the fibrillations during histological processing (Figure 7). Quantification of surface smoothness using the FI was comparable for nondestructive AOCT and for histology. The FIs calculated from OCT images and the histology for specimens ranging from smooth to deep fibrillations had near-perfect correlation by linear regression, with R = 0.98 (Table 3).

Quantification of surface smoothness. Image analysis could be performed on optical coherence tomography (OCT) images to quantify surface smoothness. A, an OCT image generating a fibrillation index (FI) of 108. Note that fibrillations are fully extended in the in situ OCT image because the specimen is in saline. B, image analysis of the corresponding histological section yielded a lower FI of 84. C, linear regression revealed good correlation between measurements of Fn on OCT and histology, with R = 0.82. This discrepancy with apparent excellent correlation by qualitative inspection may be attributed to slight flattening of the fibrillations during histological processing.
Comparison of FIOCT With FIHistology a
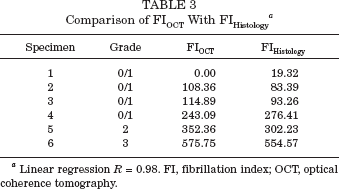
Linear regression R = 0.98. FI, fibrillation index; OCT, optical coherence tomography.
Discussion
The results of this study indicate a high potential for clinical use of AOCT as an adjunct to conventional arthroscopy for improved diagnosis and assessment of early-stage articular cartilage injury. As a microscopic cross-sectional imaging technique, the OCT arthroscope revealed surface and subsurface changes to articular cartilage that was in good agreement with histopathology (κ = 0.80). Substantial agreement (κ = 0.87) between OCT and histology was seen for specimens assigned modified Mankin structural grades 0 to 3. OCT imaging was also able to quantify surface fibrillations with near-perfect correlation to histomorphometry (R = 0.98). Overall, images of human knee cartilage obtained close to real time using the OCT arthroscope showed a high correlation with histology.
To our knowledge, this is the first report of nondestructive arthroscopic imaging of human articular cartilage using OCT. As with any new technology, it is important to begin defining it against established techniques. Optical coherence temography is unique in providing microscopic-scale cross-sectional images, which have been termed optical biopsies. 9 At an axial resolution of 10 μm, the images are more detailed than clinical MRI and ultrasound. Although the images are comparable in structural detail to low-power histology, the OCT system used in this study did not allow for resolution of cells. With respect to articular cartilage, we therefore were not able to assess chondrocyte cloning or chondrocyte viability. Use of improved laser technology may permit this in the future. In addition, the use of special stains such as alcian blue or safranin O on tissue cross-sections can give histological information on proteoglycan content. Because proteoglycan distribution was not seen well on the OCT images in this study, improving the system by using different infrared wavelengths and image construction algorithms may allow proteoglycan to be detected and quantified in the future. Although we were able to compare structural grades assigned by OCT and histology using a modified Mankin grading system, calculation of a complete Mankin score was not yet possible because of these current limitations. However, OCT has the advantage of being capable of yielding microscopic resolution cross-sectional images in near real time without damaging or excising the articular cartilage. The ability to acquire OCT images arthroscopically increases the potential clinical applications.
Using the current OCT arthroscope, AOCT imaging of the medial and lateral femoral condyles and trochlea was performed in both a right human knee and a left human knee, thereby demonstrating feasibility for arthroscopic use of OCT in human patients. Despite being from different donors, neither cadaver knee had substantial degeneration of the articular surfaces. In contrast, tibial plateaus from total knee replacements provided a consistent source of articular cartilage with varying surface topographies. Use of tibial plateau cartilage from total knee replacements therefore allowed us to perform comparative studies of cartilage with a wider spectrum of structural changes. Although we were unable to arthroscopically image the tibial plateau of the cadaver knees using the current AOCT, OCT images of the tibial plateau cartilage were of similar quality to images obtained arthroscopically of the distal femoral cartilage.
It is important to note that the OCT arthroscope can be potentially modified to image the tibial plateau and other areas of human joints. Using this initial arthroscopic design, OCT images of the tibial plateau could not be obtained through conventional arthroscopic portals because of the 0° inclination of the probe. This flat angle allowed OCT imaging only of areas that could be brought perpendicular to the probe. As a fiber-optic technique, the potential exists to modify the OCT probe into more traditional 30° and 70° arthroscopes. Such angular modifications should allow for OCT imaging of areas in human joints more comparable to what can be seen using conventional arthroscopes. Additional improvements include incorporating OCT fiber optics into a standard arthroscopic device for simultaneous arthroscopic surface and cross-sectional imaging.
Although this OCT arthroscope provided detailed information concerning surface and subsurface structure to a depth of 1.0 to 1.5 mm, the attenuation of backscattered light reduced the ability to image to greater depths. 30 In addition, the refractive index of normal versus osteoarthritic cartilage may vary based on the degree of matrix change in the arthritic cartilage. This will also affect imaging depth. In an ex vivo OCT study imaging a variety of human cartilage including hip, knee, ankle, elbow, and fingers, Herrmann et al were able to clearly identify the cartilage-bone interface in images of talus cartilage and of toe cartilage, areas with thinner cartilage than in the human knee. 13 They also imaged a patellar specimen averaging 1.66 mm in the center by analysis of OCT images that compared well with histological measurements averaging 1.77 mm. Our arthroscopic system was capable of imaging to comparable depths. Because human knee joint cartilage can exceed 3 mm in depth, we do not consider our current AOCT to be capable of depth measurements in all cases. This depth limitation does not, however, interfere with the ability of the OCT arthroscope to detect fine surface fibrillations and subsurface gaps at microscopic resolutions.
The ability of AOCT to detail surface and subsurface topography suggests a potential role for OCT in guiding articular cartilage debridement. Although arthroscopic debridement is one of the most commonly performed orthopaedic procedures, studies show that debridement is unlikely to be effective when significant cartilage damage or osteoarthritic changes are present.21,22,34 With regard to focal chondral defects and early chondrosis, the literature on debridement indicates positive effects.1,8,15,16,31 Although the goal of debridement is to retard progression of the cartilage lesion by removing loose and frayed cartilage, animal studies show that arthroscopic debridement is frequently suboptimal, resulting in residual cleavage planes or collateral damage to healthy cartilage.18,32,33 Improved image guidance may allow the surgeon to more precisely identify, remove, and stabilize damaged articular cartilage.
Debridement is currently performed using only arthroscopic surface cameras for image guidance. Significant barriers to precise debridement of diseased cartilage include the absence of updated cross-sectional image guidance in the surgical suite. The AOCT probe can potentially be used to better identify appropriate lesions for debridement and to assess the completeness of the debridement. Through image analysis, the quality of the debridement can also be quantified using measures such as the FI defined in this study. Because the FI allows for quantification of surface irregularity at the earliest stages of chondrosis, it also represents a potential tool for staging early disease and for assessing the effects of other surgical and medical treatments.
Another emerging quantitative method to assess articular cartilage is the use of indentation probes. The data from these probes can provide quantitative information to complement the surgeon's assessment of cartilage softening. Indentation probe technology has been applied to postoperative assessment of the repair tissue following autologous chondrocyte implantation. 28 Repair tissue stiffness from 8 of 11 patients evaluated using an electromechanical indentation probe was found to be 90% or greater than that of normal cartilage. We also obtained 2-mm osteochondral biopsies from the central portions of the repair sites for histological and immunohistochemical analysis. Although the current OCT has not been shown to provide information on collagen type and proteoglycan content, OCT optical biopsies can potentially complement biomechanical probe studies by providing microscopic structural information at precisely the same location as the indentation probe without removing the tissue. Although we did not directly compare OCT with conventional arthroscopic examination using surface imaging and probe palpation, further studies are planned to determine whether differences in quantitative measures of OCT FI and indentation probe stiffness correlate with chondromalacia grades assigned by conventional arthroscopic examination.
The ability to obtain arthroscopic optical biopsies of articular cartilage can facilitate longitudinal assessment of articular cartilage injury and repair. Arthroscopic analysis of human knee joints using the current OCT arthroscope revealed ready access to the medial femoral condyle, the lateral femoral condyle, and the trochlea using conventional arthroscopic portals. These are precisely the areas in which chondral defects commonly repaired using autologous chondrocyte implantation are located. Our earlier assessment of rabbit repair tissues following chondrocyte implantation confirmed the value of OCT in assessing key repair tissue parameters of repair tissue fill, surface hypertrophy, subsurface collagen architecture, and integration. 12 We found no degradation of image quality when the OCT system was used for arthroscopic analysis of porcine knees. 26 This study revealed the ability of the current OCT arthroscope to provide high-resolution images of human articular cartilage. These findings indicate a high potential for using AOCT for nondestructive assessment of chondral repairs following cartilage repair procedures such as autologous chondrocyte implantation or a future tissue-engineered repair. With the ability to image the lateral femoral condyle, OCT arthroscopy also provides a potential means to assess for subsurface cartilage damage in areas overlying MRI-detectable bone bruises following ACL injury.
In summary, we confirmed that this handheld OCT probe can be used arthroscopically in human knees to provide high-resolution nondestructive optical biopsies of human articular cartilage. Specifically, OCT arthroscopy can detect and quantify surface and subsurface changes to articular cartilage at microscopic resolutions exceeding the current capabilities of clinical MRI or ultrasound. Further study is needed to optimize OCT technology for arthroscopic microscopy of articular cartilage and to better understand the relationship between OCT back reflectance and articular cartilage degeneration and repair. The results of this study indicate a potential for clinical use of OCT as an adjunct to conventional arthroscopy for improving diagnosis of early stage articular cartilage damage, guiding arthroscopic interventions, and quantifying treatment effects in athletes and individuals with joint injuries.